
Abstract
Objectives:
The development of pneumolabyrinth without previous head trauma is a rare event; the associated symptoms may be nonspecific, and they can simulate various cochleo-vestibular pathological entities. The aim of the present study is to describe one of these rare occurrences, characterized by a peculiar onset.
Methods:
We report a case of stapes fracture secondary to ear pick penetration into the middle ear with a pneumolabyrinth that caused a recurrent paroxysmal positional vertigo (PPV) mimicking a canalolithiasis.
Results:
The patient developed a profound left sensorineural hearing loss and an intractable PPV with “migrant” features. A pneumolabyrinth was visualized with high-resolution computed tomography. A perilymphatic fistula (PLF) with stapes fracture was found while performing an explorative tympanotomy. After the surgical treatment of the PLF, the patient no longer complained of vestibular symptoms.
Conclusions:
To our knowledge, this is the fifth case of traumatic pneumolabyrinth simulating a canalolithiasis without previous history of temporal bone trauma and/or middle ear surgery. A pneumolabyrinth should be suspected in case of patients presenting recurrent intractable PPV after ear trauma.
Introduction
With the term pneumolabyrinth, we refer to the presence of air bubbles into the labyrinth, generally due to barotraumas, fractures of the temporal bone, dislocation, or fracture of the stapes with the consequent creation of a perilymphatic fistula (PLF). The iatrogenic causes comprehend ossiculoplasty, stapes surgery, and cochlear implantation surgery. 1
We distinguish a vestibular form (when air bubbles occupy the vestibule and/or the semicircular canals), a cochlear form, and combined forms with the presence of air in both vestibule and cochlea. 2
The clinical manifestations include vertigo, dizziness, combined or sensorineural hearing loss, and tinnitus. 3
The treatment of choice is based on a conservative therapy or an explorative tympanotomy (ET) with eventual repair of the defect, according to the type and entity of the damage. 3
The high-resolution computed tomography (HRCT) is mandatory to point out the presence and the extension of the air and the possible stapedial damage. 4 We report a case of pneumolabyrinth provoked by a middle ear trauma mimicking an intractable canalolithiasis, with a review of the literature regarding the cases of pneumolabyrinth with features of paroxysmal positional vertigo (PPV).
Case report
In 2014, a 36-year-old woman experienced a left ear injury provoked by an ear pick. Then she complained of left otalgia, ipsilateral hearing loss, with tinnitus and vertigo. She was evaluated in an ENT department of a regional hospital: The otoscopic examination detected a perforation of the antero-inferior quadrant of the ear drum. Pure tone audiometry demonstrated a left-sided pantonal severe sensorineural hearing loss. A spontaneous horizontal right beating nystagmus was initially described at bedside examination. A pneumolabyrinth of the left vestibule was detected by HRCT scan, so an ET was performed in general anesthesia: A fracture of the crus posterior and the footplate of the stapes was found as well as a PLF of the oval window. The fistula was repaired with tragal pericondrium, and a miringoplasty was performed with underlay technique. During the following 3 years, the left tinnitus associated with ipsilateral hearing loss persisted; furthermore, the patient described recurring transient episodes of vertigo triggered by supine position. A new audiological assessment demonstrated a left-sided pantonal severe combined hearing loss with a bone-conduction pure tone average (PTA) of 64 dB and an air-conduction PTA of 91 dB. Cervical vestibular evoked myogenic potentials conducted with 130 dB and 500 Hz click stimuli showed normal bilateral response. The neurologic examination was normal. Positional vestibular testing showed a linear-horizontal and direction-changing positional apogeotropic nystagmus more intense on the right side. A diagnosis of apogeotropic left-sided lateral canal PPV was made, and the patient was treated for months with forced prolonged position and/or Gufoni manoeuvre without any improvement. The patient alternatively presented episodes of left down-beating positional nystagmus due to a left anterior canal canalithiasis and a left horizontal canalithiasis. Finally, a clear episode of posterior canalithiasis with a rotatory down beating positional nystagmus in left Dix-Hallpike maneuver was observed. Consequently, HRCT scan was repeated, showing a mild subluxation of the crus anterior of the stapes and an increase of the previous left pneumolabyrinth, with the involvement of the entire vestibule and the crus communis (Figures 1a, 1b); a recurrence of PLF of the oval window was suspected, maybe due to an involuntary Valsalva maneuver performed shortly thereafter the previous surgery or, more probably, for an incomplete closure of the fistula. The patient was sent to our attention for a second ET. A preoperatory pure-tone audiometry revealed a severe pantonal sensorineural hearing loss. A transcanal approach with tympano-meatal flap elevation allowed to observe the persistence of the stapes fracture with perilympathic leakage from the oval window (Figure 2). During the procedure, a brief and soft aspiration on the vestibule was performed. The stapes was left in place, and the fistula was sealed with bone wax, fibrin glue (Tissucol), reinforced by bovine pericardium graft (Tutopatch). The next day, the positional vestibular symptoms were considerably decreased, and the patient was discharged from the hospital.
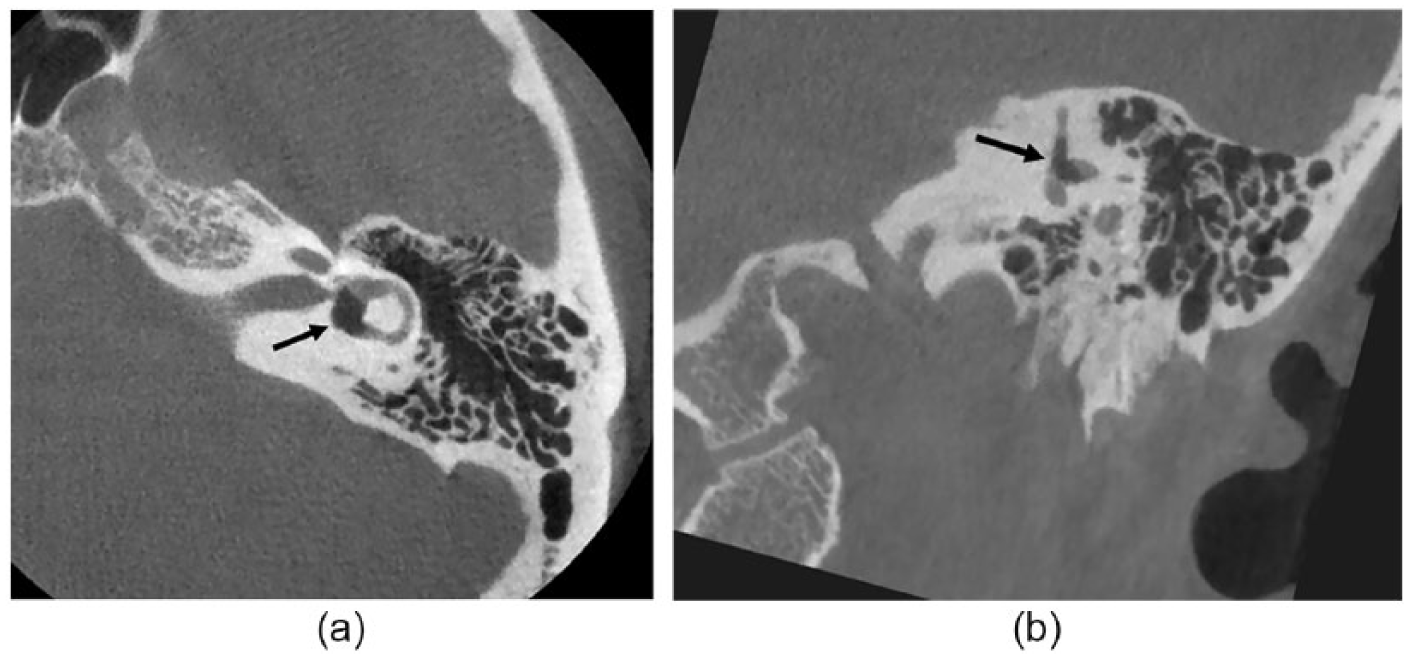
(a) Axial high-resolution computed tomography (HRCT) image of patient’s left temporal bone with the presence of pneumolabyrinth, characterized by air occupying the entire vestibule (arrow). (b) Coronal HRCT image of patient’s left temporal bone with the presence of pneumolabyrinth, characterized by air occupying the crus communis and extending in the posterior and the superior semicircular canals (arrow).
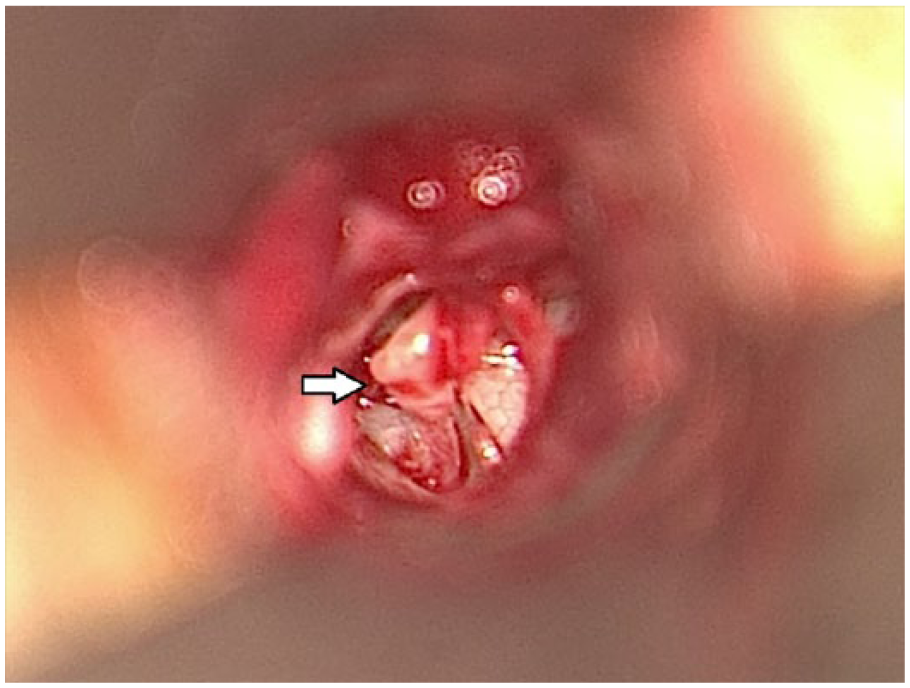
Explorative tympanotomy showing stapes footplate fracture and perilympathic leakage (arrow).
Ten days after the procedure, the patient showed a low-amplitude spontaneous right beating horizontal nystagmus but no positional nystagmus. The postoperative audiogram revealed no change in the pure tone levels. A video head impulse test showed bilaterally a normal lateral semicircular canal (SC) response and a slight impairment of anterior and posterior SC of the left ear.
The persistence of the vestibular symptoms after the first surgical procedure had suggested the recurrence of the fistula; likewise, the relief experienced after the second treatment was a clear sign of a correct repair of the defect. The immediate relief of the PPV after surgery in our opinion cannot be ascribed to a central vestibular compensation due to the too brief period of onset. The slight impairment of vertical canal functions may be considered as a collateral damage of the surgical procedure.
Pneumolabyrinth and paroxysmal positional vertigo
The review of the literature demonstrated that the cases of pneumolabyrinth associated to a PPV are only 4,1,5-7 in addition to our report (Table 1). In particular, 1 article 1 reported a case of bilateral pneumolabyrinth, but the features of PPV were presented only when the damage occurred in the right ear.
Summary of 4 Previous Cases and Our Report of Pneumolabyrinth Mimicking a PPV.
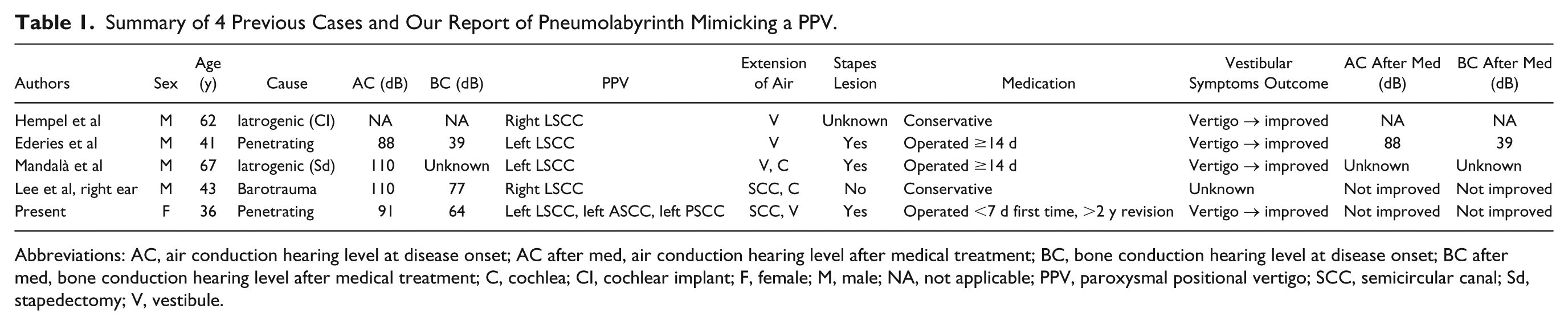
Abbreviations: AC, air conduction hearing level at disease onset; AC after med, air conduction hearing level after medical treatment; BC, bone conduction hearing level at disease onset; BC after med, bone conduction hearing level after medical treatment; C, cochlea; CI, cochlear implant; F, female; M, male; NA, not applicable; PPV, paroxysmal positional vertigo; SCC, semicircular canal; Sd, stapedectomy; V, vestibule.
Only our report involved a female patient. Mean age at the time of the injury was 50 years (range, 36-67 years).
Regarding the causes, 2 cases (40%) were iatrogenic (1 after cochlear implantation surgery and 1 after stapedectomy), 2 (40%) resulted from penetrating injuries, and 1 (20%) was caused by a barotrauma.
All the cases showed the characteristics of a PPV involving the lateral SC, while our case presented “migrant” features: Initially, the positional testing revealed a horizontal apogeotropic nystagmus more intense on the right side; conversely, during a following videonistagmoscopy, an up-beating torsional clockwise nystagmus was evoked by the positioning maneuver on the left side.
The HRCT revealed air bubbles only in the vestibular organs in 3 patients (60%), while in 2 of them (40%), the pneumolabyrinth involved both vestibule and cochlea.
Three subjects (60%) underwent surgical treatment, while in 2 cases (40%), a conservative management was preferred.
After the therapy, the vestibular symptoms subsided in 4 patients, while 1 report 1 did not specify this aspect.
Three cases did not show any improvement in the hearing level; in 1 case, this parameter was not applicable, 5 and in 1 article, 7 the hearing outcome was unknown.
Discussion
The pathological presence of air into the labyrinth implies an abnormal connection between the inner and the middle ear, generally provoked by a trauma, a PLF, or the displacement of a stapedial prosthesis in cases of previous stapedectomy. 6
In their meta-analyses, Hidaka et al 8 demonstrated that the prevalence of blunt head traumas was similar to that of penetrating injuries and most such penetrating wounds were caused by an ear pick, as shown in our case. In almost all cases presented by the authors, 8 vestibular symptoms receded after the treatment while hearing outcomes were more heterogeneous: For pneumolabyrinths limited to the vestibular organs, the hearing level improved in 48% of the patients, while no hearing improvement was demonstrated in pneumolabyrinths extended in both vestibule and cochlea.
Tsubota et al 9 proposed 3 predictive factors of hearing improvement after pneumolabyrinth: bone conduction hearing level at disease onset, interval between injury and surgery, and presence of stapes lesions.
Kobayashi et al 10 experimentally demonstrated that intrusion of air into the scala tympani was associated with a decrease of cochlear potentials, but this change in compound action potentials was reversible with the air absorption. On the contrary, drastic hearing loss is provoked by the intrusion of air into the scala vestibuli; from a histological point of view, this is associated with a collapse of the Reissner membrane. 11
Previous studies demonstrated that vestibular outcomes are generally better than the hearing results after the treatment in case of rupture of the oval window,8,12 and our report confirms this aspect. According to Prisman et al, 13 the performance of an ET and the sealing of the PLF did not correspond with a significant improvement in the hearing; furthermore, the meta-analyses of Hidaka et al 8 showed no consistent differences between conservative and surgical management. However, in our opinion and in agreement with several studies, the persistence of an abnormal communication between the inner and middle ear can lead to an irreversible cochlear damage, so surgical exploration is justified in case of history of blunt traumas, barotraumas, penetrating or iatrogenic injuries followed by fluctuating, progressive or persistent hearing loss associated with vestibular symptoms.14-17
In the entire literature, the cases of pneumolabyrinth mimicking a PPV are only 4,1,5-7 apart from our report. Ederies et al 6 hypothesized a “pneumopositional” theory whereby a positional induced vertigo was elicited by the movements of the air bubbles within the SC. This hypothesis was based on HRCT images showing the air migration within the SC in response to variation of body position: the air movements led to cupular deflection and ampullary stimulation, with consequent onset of nystagmus and vertigo. 6 According to this assumption, recurrent PPV of anterior SC should be explained by the antigravitational motion of air bubbles in the upper regions of the labyrinth when the patient is placed in a supine position. Moreover, bubbles’ movements could create an endolymphatic flow mimicking an intractable PPV of the posterior SC due to an utriculofugal deflection of the cupola. The multiple involvement of different canals in a short time could be strongly suggestive for the presence air bubbles, as demonstrated by the migratory nature of the PPV described in our patient. For these reasons, liberatory maneuvers give often unsuccessful results due to the incapacity of the air to overcome the endolymphatic density, staying in the upper region of the SC.
Mandalà et al 7 proposed another pathogenic theory for this positional vertigo: Only the structures not affected by the pneumolabyrinth could be involved in a form of PPV, and recurrent pathological stapes footplate excursions could cause traumatic detachments of otoliths. Our experience would not confirm this theory: The soft intraoperative suction of air from the vestibule and not the liberatory maneuvers has been demonstrated to be the cause of the postoperative resolution of the vertigo.
Conclusions
This is the fifth case of pneumolabyrinth simulating a PPV without previous history of barotrauma, temporal bone fractures, and/or middle ear surgery, likely caused by the presence of air bubbles in the SC. 6 When pneumolabyrinth is suspected, the HRCT is mandatory to clarify the presence and the extension of the air into the involved structures. An ET is recommended in case of persistent hearing loss with intractable vertigo after ear and/or temporal bone traumas and/or surgery. Furthermore, a pneumolabyrinth should be suspected in patients presenting recurrent intractable PPV after ear trauma.
Footnotes
Authors’ Note
The research has been conducted in full accordance with ethical principles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.