
Abstract
Objectives:
To systematically review the success rate and safety profile of the available endoscopic surgical options for radiation-induced dysphagia in head and neck cancer patients following organ preservation treatment, including upper esophageal sphincter (UES) dilation, cricopharyngeus (CP) myotomy (CPM), and CP intramuscular botulinum toxin (Botox) injection.
Methods:
A search of MEDLINE, Scopus, Google Scholar, and Cochrane databases was done to identify articles published between January 1980 and December 2017. Pediatric series, foreign language articles, series with Zenker’s diverticulum or following primary surgical treatment including laryngectomy, open UES/CP surgery, or samples with fewer than 5 patients were excluded.
Results:
An initial search identified 539 articles. All titles and abstracts were reviewed. One hundred and sixteen potentially relevant articles were inspected in more detail, and 14 retrospective studies met eligibility criteria. Dilation group included 10 studies on anterograde and/or retrograde dilation, with an overall 208 patients. Success rate ranged from 42% to 100%. The endoscopic CPM group included 3 studies with a total of 36 patients, and the success rate ranged from 27% to 90%. In the Botox group, 1 one study with 20 patients met our inclusion criteria, with an overall 65% success rate (13/20). Major complications were only reported in the dilation group, which included esophageal perforation and death.
Conclusions:
The lack of consistency across trials indicates insufficient evidence for guiding clinical practice. This systematic review suggests the need for greater standardization of outcomes and instruments. Future prospective evaluation should use validated patient-rated and clinician-rated assessment tools to optimally measure postoperative swallowing outcomes of head and neck cancer dysphagic patients following organ preservation therapy.
Keywords
Introduction
Head and neck cancers (HNCs) including oral cavity, pharynx, and larynx added up to a total number of approximately 690 000 new cases worldwide in the year of 2012, which comprises 4.9% of total cancer incidence. 1 External beam radiotherapy (RT), with or without concurrent chemotherapy (CCRT), is the primary organ preservation treatment for many patients with head and neck squamous cell carcinoma (HNSCC). The choice of treatment modality depends on many factors, including primary tumor site, clinical stage, and resectability of the tumor. For many of the early stage HNCSS, RT can be the only treatment required.
The upper aerodigestive tract is highly susceptible to radiation-induced injury.2-4 Despite advances in RT/CCRT planning and delivery, dysphagia is one of the most common side effects. 5 Up to 50% of the HNC patients treated with RT/CCRT experience moderate to severe dysphagia that may persist months to years following therapy.2,6-8 These symptoms impair normal swallowing, leading to weight loss, dietary changes, and social isolation. The severity ranges from minor swallowing difficulties taking a long time to finish meals and tolerating a regular diet to aspiration and complete feeding tube dependence. Whereas dysphagia that begins early in radiation therapy is usually temporary, late dysphagia, developing long after the completion of radiotherapy, often results from chronic inflammation and fibrosis. This late onset dysphagia is much more difficult to manage. Previous studies demonstrated that dysphagia is detrimental to the quality of life after treatment of HNC.2,6,9
RT/CCRT can result in stricture or stenosis at the level of the upper oesophageal sphincter (UES) and particularly the cricopharyngeus (CP) muscle, being the main target for surgical intervention. 10 Surgical approaches for the treatment of postradiation CP dysfunction and/or UES stenosis or stricture demonstrate mixed results. The current study aimed to systematically review and characterize the safety profile and efficacy of the available endoscopic options for the treatment of RT/CCRT-induced dysphagia in HNC patients, including UES dilation, CP myotomy (CPM), and CP intramuscular botulinum toxin (Botox) injection.
Methods
We performed a comprehensive, systematic search in PubMed databases, Cochrane Central Register of Controlled Trials, Scopus, and Google Scholar in an attempt to cover all possible indexed publications. The search strategy used was a combination of keywords indexed in Medical Subject Headings (MeSH) and keywords related to the population, intervention, and treatment outcomes, which were inserted to assist the literature survey in the databases to increase the specificity of the search. The key terms included: head and neck, cancer, carcinoma, malignancy, radiation/radiotherapy, chemoradiation, cricopharyngeus muscle, CP, upper esophageal sphincter, pharyngoesophageal, UES, cricopharyngeal dysfunction, bar, narrowing, stricture, stenosis, dysphagia, swallowing problems, dilation, Botox, botulinum toxin, and endoscopic myotomy. All of these terms were used in varying combinations for the search. The following filters were used: publication in English language, year of publication between January 1980 and December 2017, and full available article. Inclusion criteria according to the study design were any randomized controlled trial, prospective and retrospective cohorts, case-control study designs, and case series. All studies included reported the success rate and safety profile of endoscopic surgical options for UES stenosis/stricture in adult HNC patients with primary RT/CCRT-induced dysphagia, including: esophageal dilation, CP myotomy, and CP intramuscular Botox injection. Two authors (S.A.G., A.J.) reviewed the titles and the abstracts from the studies that met the selection criteria, applying the inclusion criteria. Duplicates were removed. The reference list of each article obtained was checked for further potentially relevant studies. The exclusion criteria consisted of articles that reported pediatric patients, small series (≤5 patients), foreign language articles, series with Zenker’s diverticulum, or following primary surgical treatment including laryngectomy and open UES/CP surgery. Data from the eligible studies were independently assessed and extracted by 2 authors (S.A.G., A.J.) using standardized data forms. Information about study design, primary tumor treatment (RT/CCRT), sample size, preoperative swallowing evaluation workup, surgical endoscopic intervention including the number of procedures, and duration of follow-up were assessed. Reported success and complication rates related to endoscopic surgical treatment of CP/UES dysfunction were defined as the primary outcomes.
Results
An initial search identified 539 articles. All titles and abstracts were reviewed. One hundred and sixteen potentially relevant articles were inspected in more detail, as shown in Figure 1. Eleven review articles were excluded, and 91 articles were excluded due to (1) inability to isolate outcomes in HNC patient subset following primary RT/CCRT therapy, (2) an insufficient sample size (N < 5), or (3) an inadequate description of the outcomes. A final total of 14 observational retrospective studies (N = 264 patients) met eligibility criteria and were included in the current systematic review as summarized with the surgical procedure characteristics in Table 1.11-24 Table 2 shows the preoperative swallowing assesment and success and complication rates of CP myotomy (N = 3 studies; overall 36 patients), UES dilation (N = 10 studies; overall 208 patients), and Botox injection to the CP muscle (N =1 study; 20 patients) in adult HNC patients with dysphagia following organ preservation therapy.
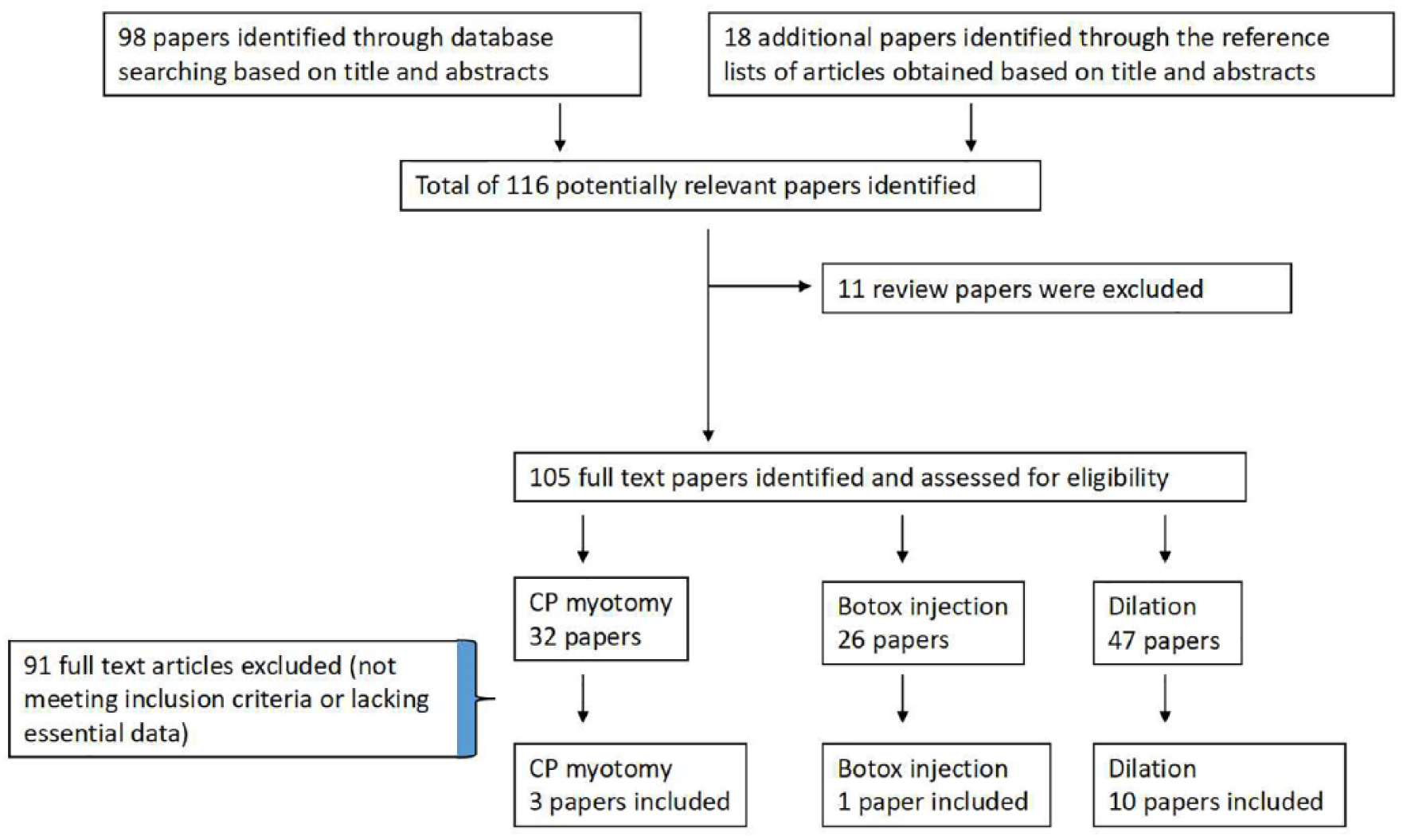
Flowchart showing the process of study selection.
Characteristics of the Studies Included in the Current Systematic Review.
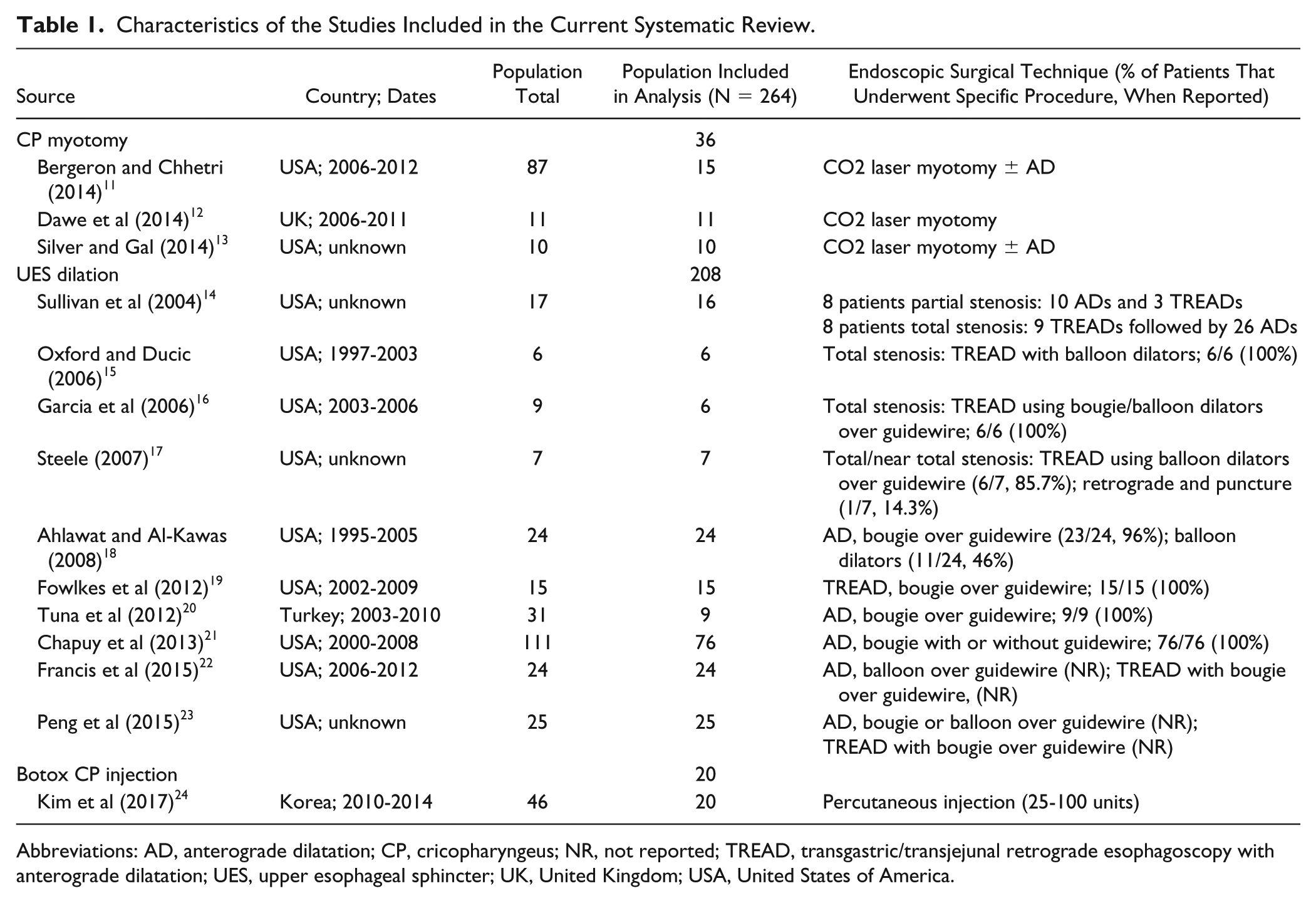
Abbreviations: AD, anterograde dilatation; CP, cricopharyngeus; NR, not reported; TREAD, transgastric/transjejunal retrograde esophagoscopy with anterograde dilatation; UES, upper esophageal sphincter; UK, United Kingdom; USA, United States of America.
Preoperative Swallowing Evaluation and Success and Complication Rates of Endoscopic UES/CP Surgery for Radiation-Induced Dysphagia in Head and Neck Cancer Patients.
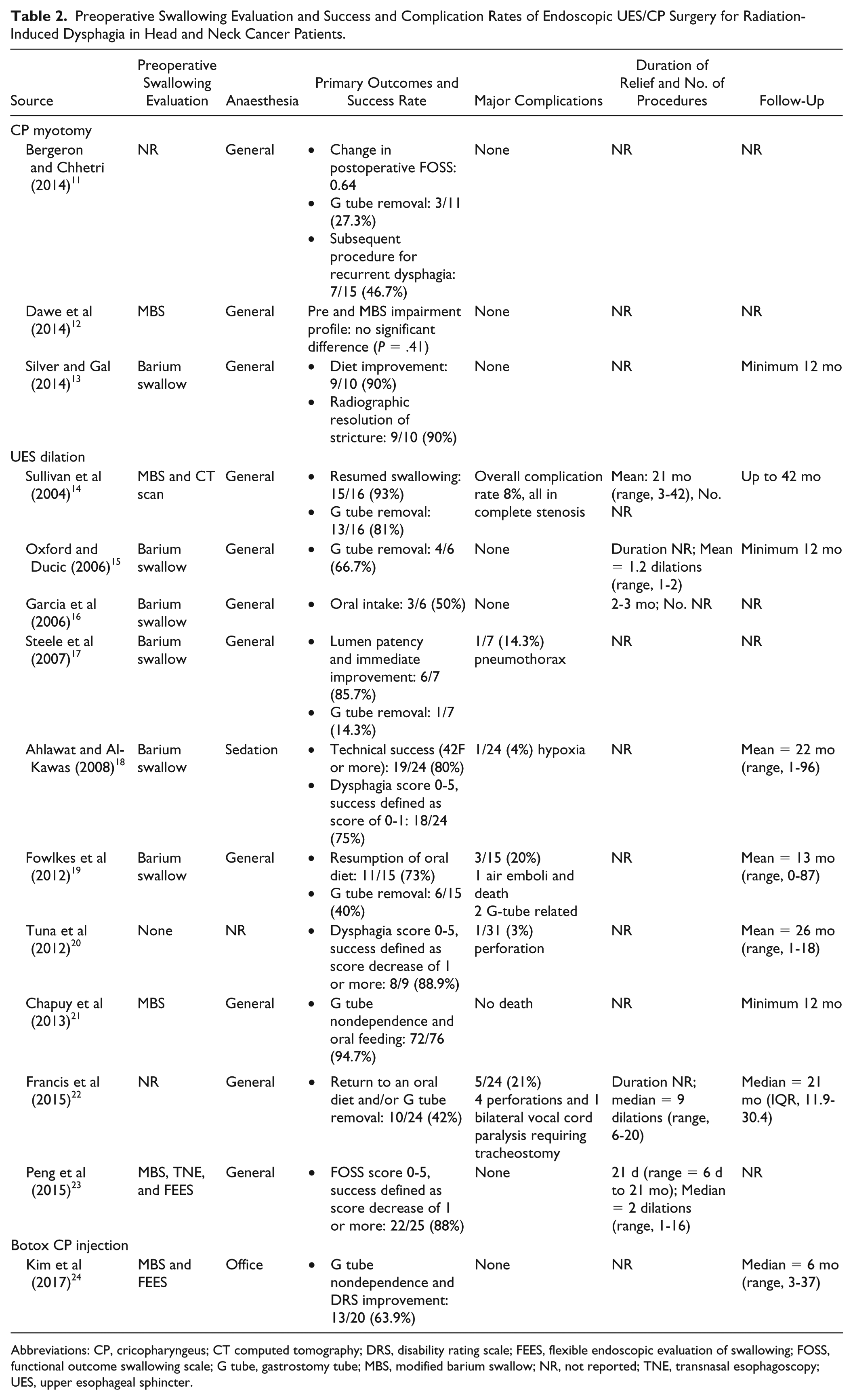
Abbreviations: CP, cricopharyngeus; CT computed tomography; DRS, disability rating scale; FEES, flexible endoscopic evaluation of swallowing; FOSS, functional outcome swallowing scale; G tube, gastrostomy tube; MBS, modified barium swallow; NR, not reported; TNE, transnasal esophagoscopy; UES, upper esophageal sphincter.
The majority of articles reported barium swallow study or modified barium swallow study for preoperative evaluation of RT/CCRT-induced dysphagia (N = 11). Reported primary postoperative outcomes were inconsistent and differed between studies. These included return to oral diet or postoperative diet advancement, precutaneous feeding tube removal, surgical success as lumen patency, and improvement of dysphagia score or scale (Table 2). Reported success rate ranged from 42% to 100% in the UES dilation group, 27% to 90% in the CP myotomy group, and 65% success rate in the CP Botox injection group.
Discussion
Radiotherapy with or without concurrent chemotherapy is the workhorse for organ preservation treatment of many oral, pharyngea,l and laryngeal cancers, with higher potential of speech and swallowing function. 25 Unfortunately, organ preservation does not always translate into good functional result in terms of swallowing. Radiation-induced dysphagia has complex multifactorial pathogenesis stemming from damage to skin, connective tissue, salivary glands, nerves, and muscles.4,26 Acute injuries of edema and mucositis are often temporary and resolve within a few months after treatment; however, some persist, producing chronic changes manifest as fibrosis. 4 This may develop or persist long after RT/CCRT treatment completion, leading to pharyngoesophageal stricture or stenosis and impaired strength, timing, and coordination of motion of the tongue base, hyolaryngeal complex, pharyngeal constrictors, and upper esophagus. 27
The severity of radiation-induced dysphagia is dependent on total radiation dose, dose per fraction and schedule, target volumes, treatment delivery and organ sparing techniques, concurrent chemotherapy, percutaneous tube feeding use, genetic factors, smoking status, concurrent swallowing exercises/therapy, and psychological coping strategies as reviewed by Platteaux et al. 28 Radiation-induced dysphagia is a challenging clinical problem that must be systematically treated. This group of patients has a notable decrease in quality of life secondary to post-RT/CCRT dysphagia. Moreover, they are often psychologically devastated as they have undergone what was described as “organ sparing” treatment yet still suffer from the debilitating long-term sequelae of radiation treatment to the head and neck.
A multidisciplinary team approach is optimal for the management of post-RT/CCRT–induced swallowing disorders, consisting of the treating radiation oncologist, an otolaryngologist, a speech-language pathologist, and a dietician. Nonsurgical treatment options consist of pain management, dietary alterations, oral nutritional supplementation, and exercise-based swallowing preservation protocols. 29 These include compensatory and rehabilitation strategies designed to reduce aspiration and improve bolus flow, range of motion of oral and pharyngeal structures, and sensory-motor integration.28,29 Surgical intervention is reserved for structural or functional swallowing dysfunction that cannot be relieved by rehabilitation therapy alone. These include endoscopic procedures; open reconstructive surgery, including functional laryngectomy; and/or placement of gastrostomy tube for feeding.29,30 Although the RT/CCRT-induced injury is multilevel and complex, the CP muscle and UES segment are typically the main surgical targets in the treatment of oropharyngoesophageal dysphagia following organ preservation oncological treatment. There are several retrospective series and systematic reviews reporting the outcomes of endoscopic management of CP dysfunction and UES stenosis or stricture for different etiologies. However, there is surprisingly a limited literature specifically for the HNC population following primary RT/CCRT.31,32
For centuries, the mainstay of therapy for proximal esophageal stenosis has been anterograde dilation.31,33 Retrograde dilation refers to the passage of a dilator into a stenotic/stricture segment as approached from the gastroesophageal junction and into the esophagus, in a cephalad direction. A rendezvous procedure, which incorporates simultaneous anterograde and retrograde approach, is utilized when a lumen cannot be clearly identified.31,33 Dilation can be accomplished using a variety of dilating devices (ie, bougie, balloon, olive-tip dilators) and adjunctive techniques.
In addition, this can be done with or without fluoroscopic guidance. 33 Strictures that require continued multiple dilation sessions after the achievement of an adequate luminal diameter (ie, 12 mm or larger) to relieve dysphagia are considered refractory. 33 Post-RT/CCRT patients constitute a special group as their stenosis/stricture is often remarkably fibrotic and resistant to dilation. 34 Based on the results presented here, UES dilation was found to be the most commonly reported endoscopic approach for the treatment of postradiation UES benign stenosis or stricture, with success rate reported to range between 42% and 100%.14-23 Unfortunately, most publications lacked data on the duration of symptomatic relief and number of procedures that were needed to alleviate dysphagia symptoms in this group of patients. Moreover, the studies were lacking data on postoperative subjective and objective swallowing assessment.
A subset of post-RT/CCRT dysphagia patients was found to benefit from enlargement of the UES opening and lower resistance to transsphincter flow, achievable by endoscopic sectioning of the CP fibers (myotomy) or by CP Botox injection.35-37 Endoscopic CPM was first described in 1994 38 and was reported as a safe treatment for CP dysfunction of various causes.37,11 Our extensive literature review yielded only 3 studies on the effectiveness of CPM for postradiation CP dysfunction or lack of relaxation.11-13 Overall, only 36 patients were included with mixed success rates. Bergeron and Chhetri 11 compared CPM outcomes based on etiology and indication and found the least improvement for those with prior radiation. There are numerous methods for delivering Botox to the CP: Rigid and flexible endoscopes, fluoroscopy, and EMG guidance have been used as well as direct injections in the muscle during surgery.35,36 The mechanism of action of Botox in creating a temporary blockade of neural stimulation to muscle would suggest that Botox injection will only be effective in functional muscle tissue and not in fibrotic muscle. It follows that the success rate will be lower following radiotherapy, in the setting of a fibrotic CP. Literature review presented here cannot demonstrate a clear relation between success rate and radiotherapy based on the single paper identified. 24
The current study reviewed the 3 main endoscopic options, as reported in the literature, to treat post-RT/CCRT–induced pharyngoesophageal segment narrowing. Preliminary studies for the treatment of pharyngeal stenosis or non-retroflexing epiglottis were not included.39,40 The limitations of the current study include the retrospective nature of studies and their relatively small sample sizes. The majority of reports had either mixed group of patients (total vs. partial stenosis) or lacked data on previous operative history, number of procedures, duration of symptomatic relief, and details on operative and postoperative minor and major complications. Moreover, the reported postoperative swallowing outcomes were inconsistent and lacked objective and subjective measures. A wide range of rates indicates variability in the data. For these reasons, we could not compare the surgical outcomes between the different endoscopic approaches. Due to heterogeneity of the data, a meta-analysis was not conducted. Yet, to the best of our knowledge, this is the only systematic review to discuss and summarize the current literature on the surgical endoscopic management of dysphagia following organ preservation therapy.
Conclusions
In conclusion, this systematic review demonstrates the endoscopic options for treatment of HNC dysphagic patients following organ preservation therapy, including: UES dilation, CPM, and Botox injection. More importantly, this study emphasizes the need for greater standardization of postoperative outcome assessments. The lack of consistency across trials indicates insufficient evidence for guiding clinical practice. Future prospective evaluation should use validated patient-rated and clinician-rated assessment tools to optimally measure postoperative swallowing outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.