
Abstract
Background:
Correction of caudal septal deviation is a challenging task that may require multiple surgical approaches.
Objective:
To introduce a novel technique – caudal septal division and interposition batten graft – and evaluate its surgical outcomes in patients undergoing correction of caudal septal deviation.
Method:
The surgical procedure includes a division of the deviated caudal L-strut preserved after resection of the deviated quadrangular septal cartilage at the central portion. A batten graft made of septal cartilage or bone is interposed between the cut ends of the caudal L-strut, the upper part of which mobilized toward the more concave side of the nasal cavity, and then sutured. The medical records of 29 patients with caudal septal deviation who underwent septoplasty using caudal L-strut division and interposition batten graft technique between January 2016 and March 2018 were retrospectively reviewed. Patient satisfaction and symptom improvement were evaluated by using the Nasal Obstruction Symptoms Evaluation scores. Endoscopic assessment of deviation correction was performed and postoperative complications were analyzed.
Results:
Of the 29 patients, 19 (65.5%) answered the telephonic interview. Mean Nasal Obstruction Symptoms Evaluation scores were 62.1 preoperatively and 9.2 postoperatively, exhibiting significant improvement (P < .001). Satisfaction was rated as much improved in 9 (32.0%) patients, improved in 16 (57.0%), unchanged in 2 (7%), and worse in 1 (4%). Records of endoscopic examinations showed that 26 (82.9%) patients had a straight septum, 4 (11.4%) had improved but persisting caudal deviation, and 2 (5.7%) had no available data. Four patients had postoperative complications: 2 had septal abscesses, 1 had wound dehiscence, and 1 had synechia. All of these complications were managed without persistent problems.
Conclusions:
Caudal septal division and interposition batten graft can serve as an alternative surgical approach with acceptable surgical outcomes for managing severely deviated caudal septum.
Level of evidence:
4
Keywords
Introduction
In the surgical correction of the deviated septum, correction of caudal septal deviation is a particularly difficult aspect. Using conventional techniques, which include batten grafting, scoring incisions, cutting and suture technique, and swing door technique, most caudal septal deviations can be corrected.1-4 However, in some cases, the use of conventional techniques is insufficient and may result in unsatisfactory outcomes. Because the shape and severity of the deviation vary along with the intrinsic physical characteristics of the caudal septum, corrective measures should vary accordingly. Hence, surgeons must be prepared with multiple surgical techniques for caudal septal correction.
Batten grafting is a good tactic for correcting deviated caudal septum; however, the batten graft itself may bend with the inherent caudal septal curvature, when the bending force of the native caudal septal cartilage overrides the stenting power of the batten graft. The swing door technique, in the same sense, may not be consistently effective when the strong native caudal septum exhibits severe curvature.
An essential element for the successful correction of curved septal cartilage is effective disruption of the intrinsic memory of the elastic recoil of the cartilage. Cartilage scoring is a popular method to disrupt the intrinsic memory of the cartilage; however, this technique carries the risk of weakening the caudal septum, thus causing an unpredictable result. 5 The cutting and suture technique is another powerful approach that can break the cartilage bending memory; however, it risks shortening the length of the caudal septum, which may result in tip deprojection or saddle nose deformity.
We have been treating caudal septal deviation primarily using cartilaginous or bony batten graft, with intermittent use of the cutting and suture technique. The ideal shape of the caudal septum that we sought to create is a straight structure, of which the base sits on the midline, strong enough to bear the weight of the nasal tip, thicker at the base, and smoothly gets thinner as it reaches to the top. However, in certain situations, when we conduct the cutting and suture technique, we have noticed that, rather than using the side-by-side placement of the batten graft, interposition of the batten graft in the mid-portion of the cut ends of the caudal septum can transform the caudal septum, such that it exhibits the desired shape and strength. Thus, this study was performed to evaluate the technique, feasibility, and surgical outcome of this new approach for caudal septal correction: caudal septal division and interposition batten graft.
Patients and Methods
Patients
This retrospective study was approved by the institutional review board of Asan Medical Center. The medical records of 29 patients with caudal septal deviation who underwent septoplasty using caudal septal division and interposition batten graft by the senior author (YJJ) between January 2016 and March 2018 were retrospectively reviewed. Patient satisfaction and symptom improvement were evaluated by using the Nasal Obstruction Symptoms Evaluation (NOSE) scores. 6 Postoperative 2-month symptom score was evaluated by telephone interview. The telephone interview was carefully performed not to make the interviewees feel pressured to respond to certain ways. Also, long-term symptom evaluation was done at 15 to 40 months postoperatively by web-based questionnaires to avoid possible bias that telephone interview may induce. The surgeon documented pre- and postoperative endoscopic findings of the nasal cavity; thus, assessment of deviation correction was performed in a retrospective manner. Two otolaryngology specialists individually assessed the endoscopic photos and categorized them into three categories: straight, improved but with residual deviation, and no change. When there was disagreement between the two specialists, it was resolved by discussion. Demographic data, concurrent procedures, grafting materials, postoperative complications, and revision surgeries were also assessed.
Surgical Procedures
All procedures were performed under general anesthesia. Hemitransfixion incision was performed at the caudal end of the septal cartilage and the bilateral septal mucosal flap was elevated. After elevation of the septal mucosa, deviated septal bone and cartilage were resected and harvested, preserving more than a 1-cm width of the L-strut. The remaining L-strut was cut at the most-bent portion of the caudal part; a batten graft comprising septal cartilage or bone was interposed between the cut ends of the caudal L-strut, mobilizing the upper part of the caudal septum toward the concave side of the nasal cavity (Figure 1). The position of the upper and lower parts of the caudal septal cartilage and interposed batten graft were adjusted with tooth forceps to generate the caudal septal length as desired. Then, the realigned caudal L-strut and batten graft with varying height were sutured 4 to 7 times until sufficient stability was reached, using 5-0 polydioxanone suture (PDS). In some cases, when the support of the caudal L-strut was insufficient with the use of the interposed batten graft, an additional batten graft was sutured to the previously concave side of the caudal septum to provide further support. The procedure was completed with suturing of the incision site, silastic sheet fixation to the septum, and nasal packing. Nasal packing was removed on postoperative day 1, and silastic sheets were removed at 4 to 6 days after the operation.
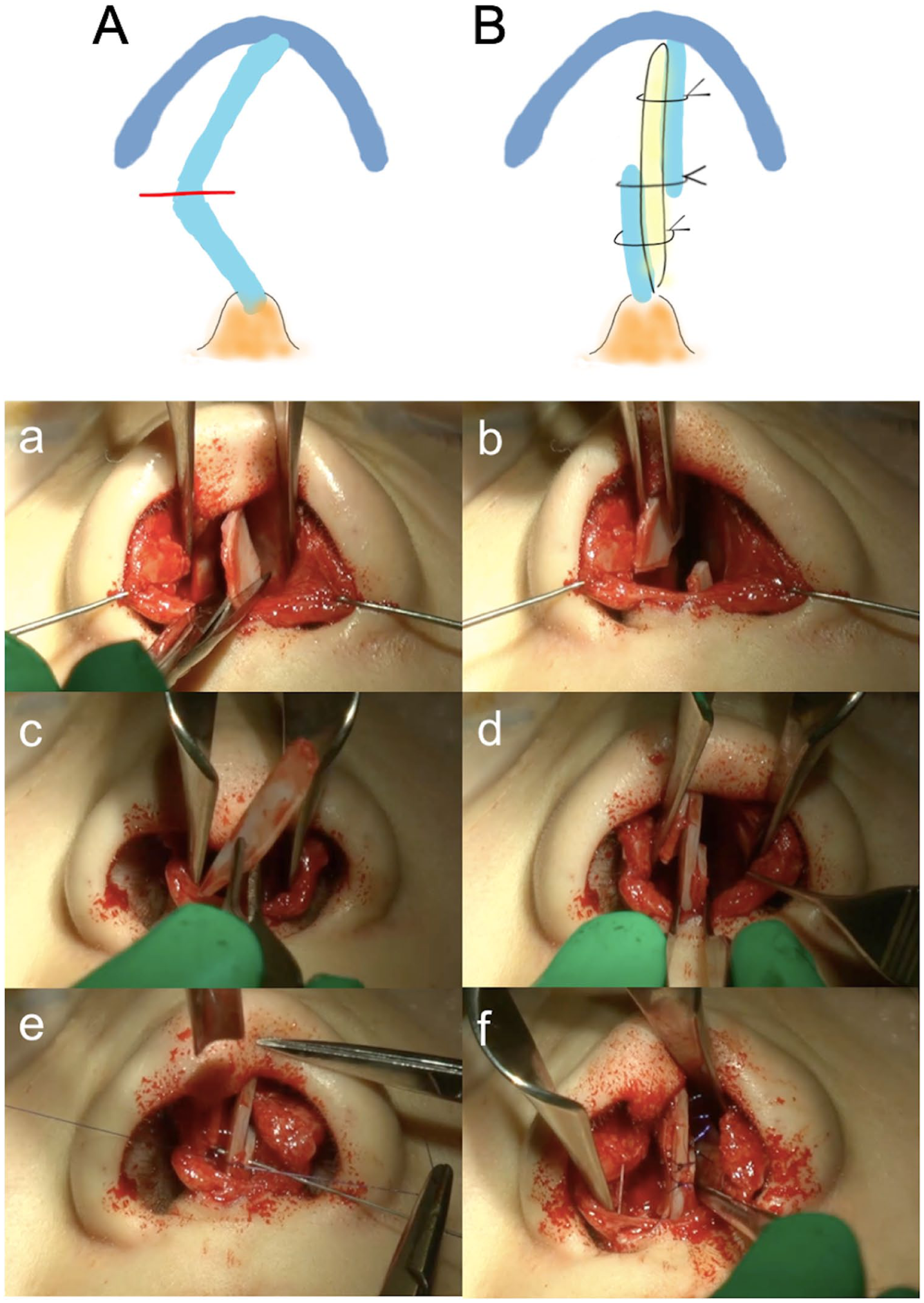
Illustration of the surgical procedure. (A, a-b) Cutting of caudal L-strut at the most-bent portion. (B, c-f) Interposition of a batten graft in between the cut ends of two septal cartilage flaps and fixation with PDS sutures.
Statistical Analysis
All statistical analysis was performed using SPSS version 23 (IBM, Armonk, New York, USA). Two-tailed paired t-tests were used to compare preoperative and postoperative NOSE scores. P values less than .05 were considered statistically significant.
Results
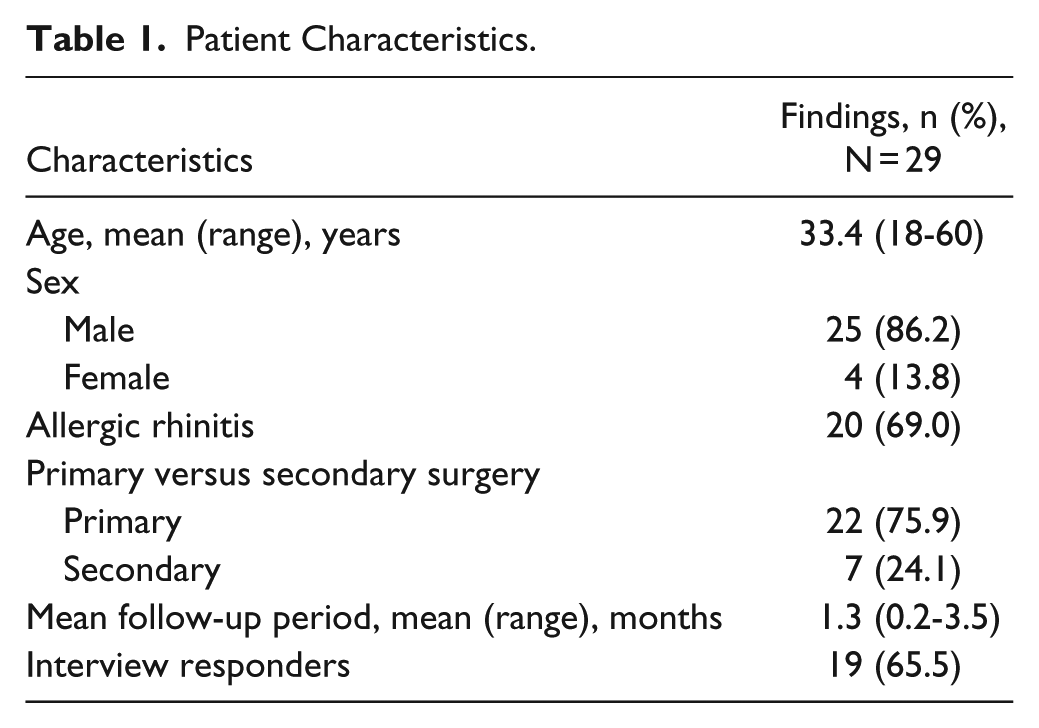
Of 29 patients, 25 (86.2%) were men and 4 (13.8%) were women; the mean age was 33.4 years (range, 18-60 years) (Table 1). Twenty patients (69.0%) had allergic rhinitis; 7 (24.1%) were undergoing revision surgery. The mean follow-up period was 2.1 months (range, 2.0-3.5 months) and 19 (65.5%) patients responded to the telephonic interview.
Patient Characteristics.
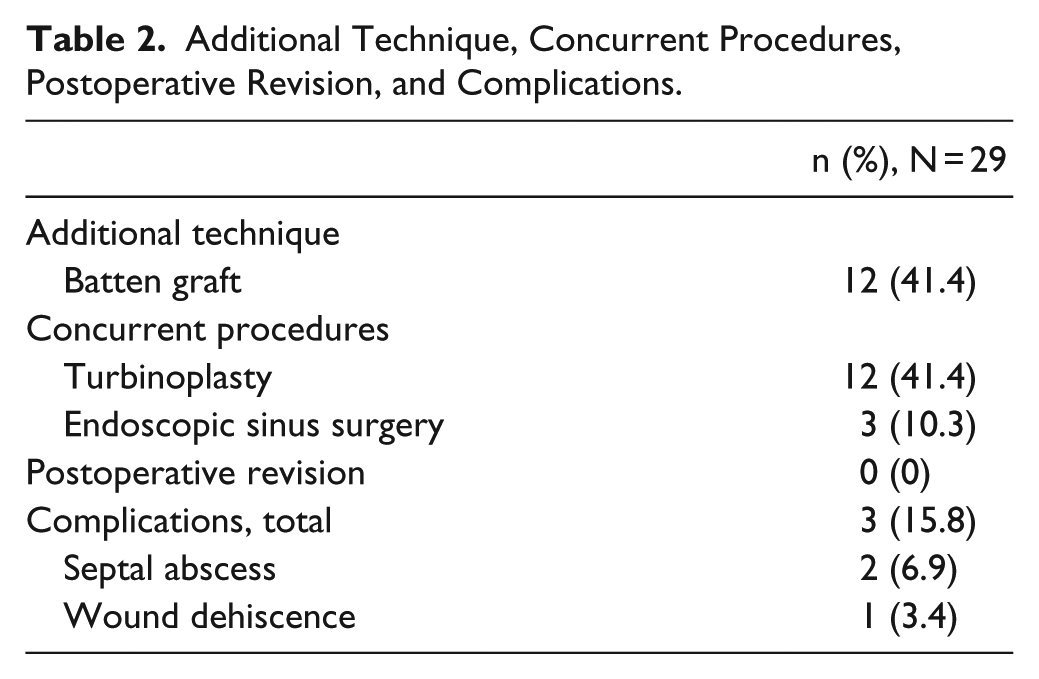
Additional batten grafting was performed after the caudal septal division and interposition batten graft in 12 (41.4%) cases. Concurrent surgical procedures were turbinoplasty in 12 (41.4%) patients and endoscopic sinus surgery in 3 (10.3%) patients (Table 2).
Additional Technique, Concurrent Procedures, Postoperative Revision, and Complications.
To evaluate surgical outcomes, pre- and postoperative endoscopic photographs, taken at the level of the external nasal valve area, were compared. Figure 2A shows examples of endoscopic photos of patients with either postoperatively straight septum or improved septal deviation without straight result. Twenty-six patients (89.7%) had a straight septum, while 3 (10.3%) patients had improvement with some residual deviation; no patient exhibited a lack of postoperative structural change of the caudal septum (Figure 2B).
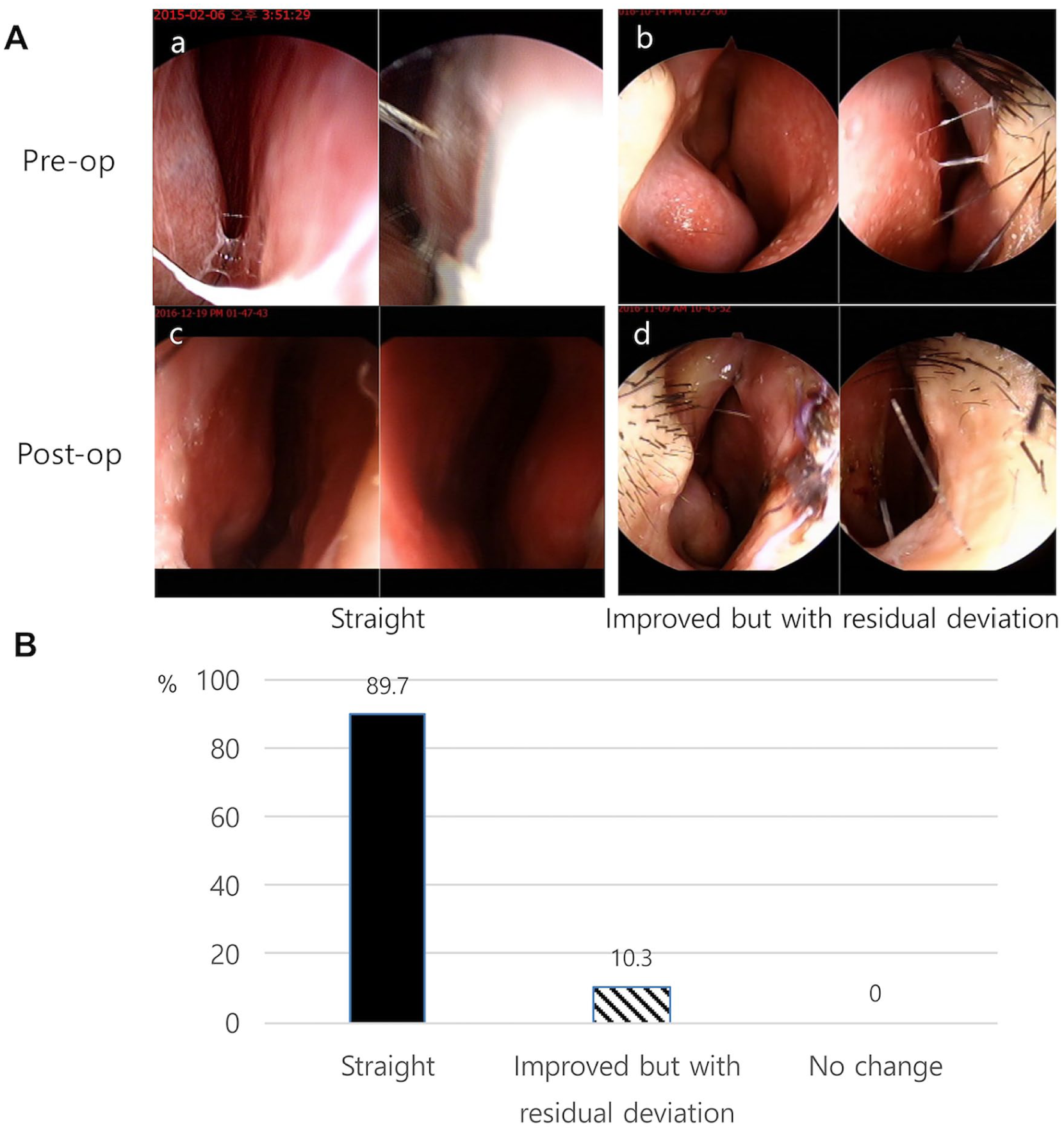
Evaluation of surgical outcomes via nasal endoscopic exam. (A) Examples of postoperatively straight septum and improvement with residual deviation. (B) Diagram of endoscopic measures of surgical outcomes.
The mean preoperative NOSE score was 62.1; it decreased to 9.2 at 2 months after the surgery and the difference was statistically significant (P < .001) (Figure 3A). Among the 19 telephonic interview responders, subjective patient satisfaction was “much improved” in 8 (42.1%) patients, “improved” in 9 (47.4%), “no change” in 1 (5.3%), and “worse” in 1 (5.3%) (Figure 3B). The patient who responded that the nasal obstructive symptom was worse after the surgery experienced difficulty in self-removal of the nasal crust, due to the increased thickness of the caudal septum from grafting. Twelve out of 29 patients responded to the long-term symptom survey, at 29.1 (mean) months (range,15.1-40.6) after surgery (Figure 3A). Mean long-term NOSE score was 32.1; subjective satisfaction was “much improved” in 3 (25.0%) patients, “improved” in 7 (58.3%) patients, 1 (8.3%) “no change,” and 1 (8.3%) “worse” (Figure 3B).
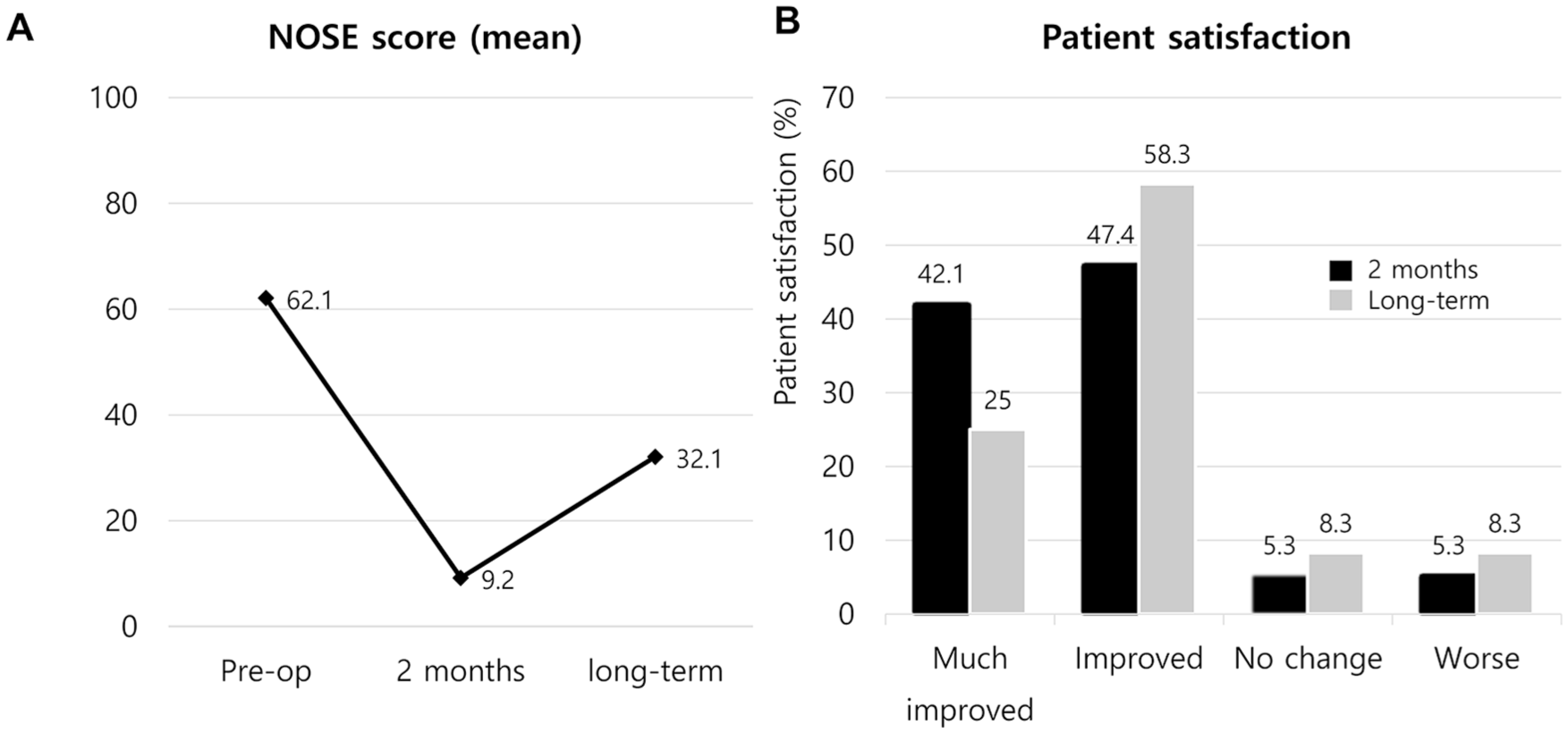
Preoperative, postoperative at 2 months, and long-term mean Nasal Obstruction Symptoms Evaluation (NOSE) score (A) and subjective patient satisfaction (B).
Complications occurred in 3 (3.4%) study patients. Two patients (6.9%) developed septal abscess, which was resolved with incision and drainage of the abscess pocket and irrigation with betadine solution; 1 (3.4%) patient had wound dehiscence at the hemitransfixion incision site, which was resutured. All complications were resolved without long-term consequences; no patient required postoperative revision surgery.
Discussion
Correcting caudal septal deviation is one of the most difficult tasks in septoplasty, particularly when the surgeon aims to correct severe caudal septal deviation, which is skewed more than 50% of the length between midline and lateral border of the internal nasal valve, without jeopardizing caudal septal stability. We found this new technique, caudal septal division and interposition batten graft, useful for correcting caudal septal deviation in selected cases.
Caudal septal division and interposition batten graft was an effective surgical approach, because postoperative caudal septal position showed an improved state of deviation in all observed cases; the postoperative NOSE score was significantly reduced, from 62.1 preoperatively to 9.2 postoperatively, and 89.5% of study patients reported improved nasal obstruction. The long-term follow-up data are not as dramatic though, with mean NOSE score of 32.1 and 83.3% of overall satisfaction. From this, we can assume that improved state of nasal obstruction persists in the long-term manner as well, although it is not as good as postoperative 2-month result. This result is comparable with the outcome reports from other studies: the cutting and suture technique resulted in 83% subjective satisfaction and 98% improvement in caudal septal deviation from endoscopic examination; 4 batten grafting resulted in reduction of the NOSE score from 70.5 preoperatively to 28.7 postoperatively, 100% improvement in the endoscopic examination, and improvement of symptoms in 91% of patients;7,8 anterior septal reconstruction resulted in reduction of the NOSE score from 68.2 preoperatively to 21.1 postoperatively. 9
Our caudal septal division and interposition batten graft technique might seem similar to pre-existing cutting and suture technique, but there are some distinctive differences between the two. Cutting and suture technique is a technique that involves cutting of the caudal septum and realigning them by suturing, which can be used with additional batten grafting optionally. On the other hand, caudal septal division and interposition batten graft essentially involves batten grafting at all times. Also, we positioned batten graft not on one side, but in between two cut ends of caudal septal cartilage. In this manner, the caudal septal height can be more easily adjusted.
There are a few notable merits of this technique, compared with existing methods for caudal septal correction. First, it is an effective method for correcting very severe deviation, which narrows the width of nasal valve area by half or even narrower. Although most caudal septal deviation can be corrected by suture techniques or batten grafting, some patients exhibit severe deviation such that these techniques alone cannot provide satisfactory results. When caudal septal deviation is sufficiently severe that it is necessary to cut the cartilage to eliminate the force of cartilage recoil while maintaining its original shape, caudal septal division and interposition batten graft can serve as a good approach. Moreover, the new technique provides benefits that include destruction of cartilage bending force; no harm to keystone area stability, compared with the extracorporeal or modified extracorporeal technique; 10 and preservation of the strong native connection between the nasal spine and caudal septum, impairment of which can weaken caudal septal stability.
Second, caudal septal height can be easily adjusted with caudal septal division and interposition batten graft. The cutting and suture technique typically does not shorten the caudal septal height, because excessive cartilage is interposed and sutured; however, when there is a notable reduction of septal height after overlapping the upper and lower ends of the cut septal cartilage, placement of the interposed batten grafting is a good alternate approach. A surgeon can easily control the caudal septal height by adjusting the suture fixation points of the upper and lower portions of the caudal septum, centered by the interposed batten graft.
Third, this technique can be useful when the position of the anterior nasal spine itself is skewed toward a narrower side of the nasal cavity. Frequently, in patients with facial asymmetry, the position of the anterior nasal spine is not at the midline of the nasal base. With caudal septal division and interposition batten graft, the interposed batten graft – positioned lateral to the nasal spine and lower part of the caudal septum – can add some volume to the concave nasal cavity and equalize the nostril base width, which is caused by the tilted anterior nasal spine.
There also are some disadvantages to this technique. First, this technique will increase the thickness of the caudal septum. A single interposed batten graft typically increases caudal septal thickness, and the degree of thickness gained with the procedure often has no clinical significance. However, one patient complained of step formation at the caudal septum, which interfered with crusting from the nostrils, care should be taken not to excessively enlarge the caudal septum. Second, the interposed graft can be tilted. No patient complained of this problem in our study; however, because the interposed graft is sutured with cartilage flap from either side, there remains a possibility of tilted graft. Graft tilting, however, could be complemented by the use of another batten graft. Third, there are some morbidities associated with this technique. Bilateral elevation of septal mucosa involves a greater risk of septal hematoma formation than unilateral opening of the septum. Furthermore, we noted that the use of multiple PDS sutures predisposed patients to postoperative inflammation. In our case series, the complications of septal abscess formation in two patients could have arisen from these factors.
This study has a few limitations. First, there were a limited number of study patients; long-term follow-up results are collected in less than a half of the total cohort. Future large-scale studies with long-term follow-up data are needed for more accurate evaluation of the efficacy of this new technique. Second, many of the study patients underwent concurrent procedures, such as turbinoplasty or batten grafting; thus, it is difficult to conclude that the surgical outcomes of our study are solely the result of caudal septal division and interposition batten graft. However, we suspect that in patients with severe caudal septal deviations, most nasal obstruction symptoms are not relieved until the caudal deviation is corrected; thus, our new technique is likely to have contributed to the good functional result. Third, as NOSE score is retrospectively collected by telephone interview, there are higher chances that the result could be swayed to certain direction. Considering that problem, we made an effort to make our survey reliable by making a standard script for before asking, and did a long-term survey in the written form. Fourth, there are time differences between the symptom interview and postoperative endoscopic exam, which could be a confounding factor in the interpretation of the surgical outcomes. For that reason, we have checked the time difference and, luckily, there was no patient with a large gap; it was within 1 month in all patients.
Conclusion
Caudal septal division and interposition batten graft can serve as a useful surgical approach for managing deviated caudal septum.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.