
Abstract
Background:
In this paper, the author describes a novel step-by-step setback procedure for correcting protruding lobules; the success of correcting protruding lobules depends on the nature and severity of the auricular lobule deformity. Although the auricular lobules occupy small areas on either side of the head, protruding or misshapen lobules exert a significant and sometimes exaggerated disfiguring influence on the otherwise aesthetically pleasing appearance of the ears. Because the lobule is a soft structure without a cartilage skeleton, the correction of a protruding ear and lobule is always a challenge.
Methods:
Protruding lobule abnormalities stem from deformities of the cauda helicis (cartilaginous helical tail) of the auricular lobule, soft tissue, and/or a shortage of anterior skin; however, the abnormalities are usually a combination of all of the above. Therefore, surgical procedures should address all of the causes of lobule deformity and preserve as much tissue and blood supply as possible. Achieving a successful intervention depends on reducing the tension that affects the entire lobule.
Results:
This is a retrospective analysis of 660 patients who had otoplasty performed by the first author between January 2010 and December 2017. Correction of the ear lobule was needed in 398 (60.3%) patients. Of these, 44.6% patients were male, 55.4% female and the average age was 9 years (range 4-18 years). In this patient cohort, 356 (89.4%) required bilateral and 42 (10.5%) unilateral ear lobule correction. Standardized pre- and postoperative images were recorded for each patient.
Conclusion:
The goal of a setback procedure is a natural and harmonious auricular lobule appearance that is achieved through simple, optimal surgery that addresses all of the features of the auricular anatomy.
Introduction
Protruded lobules cause prominence of the lower third of the pinna. This paper describes a novel step-by-step setback procedure for correcting protruding lobules. The success of correcting protruding lobules depends on the nature and severity of the auricular lobule deformity. Although the auricular lobules occupy small areas on either side of the head, protruding or misshapen lobules exert a significant and sometimes exaggerated disfiguring influence on the otherwise aesthetically pleasing appearance of the ears. Because the lobule is a soft structure without a cartilage skeleton, the correction of a protruding ear and lobule is always a challenge. 1
There are four primary causes of auricular protruding lobule deformities:
A protruding helical tail.
Misshapen soft tissue.
Asymmetry of the skin envelope.
A combination of the above.
There are two options for correcting protruding lobules. The simplest is the nonsurgical technique of taping the lobule to the mastoid during the first week of life. If taped for 3 weeks, the results are typically permanent (Figure 1). 2
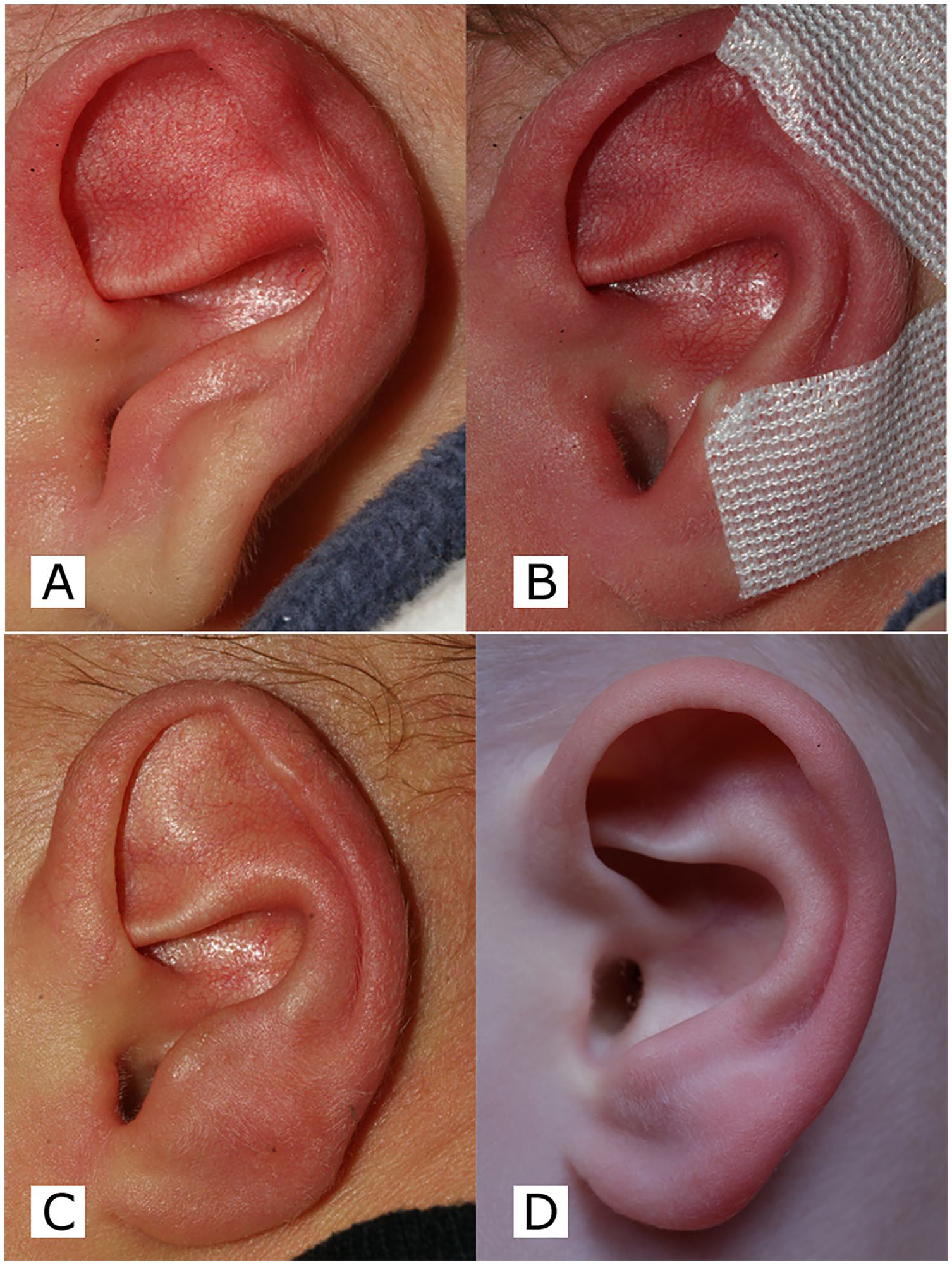
(A) Protruding lobules after birth. (B) Lobules after a standard taping procedure for 3 weeks. (C) Lobule result after 3 weeks of taping. (D) Lobule result after 3 years.
Surgical Techniques
The current techniques summarized by Sadick and Gosain are the most prevalent; however, they are expanded upon herein.3,4
Methods
Patients with protruding lobules who underwent surgery by Dr. Raunig in the General Hospital of Spittal/Drau (Austria) between January 2010 and December 2017 were included. The records for this case series (671 patients) were analyzed retrospectively. Standardized pre- and postoperative images were recorded for each patient. The study was approved by the local ethics committee of Carinthia and meets the requirements of ICH-GCP as well as the requirements of the Declaration of Helsinki.
Intervention – Surgical Procedure
Before commencing surgery, it is important to determine whether the helical tail or soft tissue caused the protrusion. Often, the protrusion is caused by a combination of factors, as mentioned above. One should address the cartilage and the soft tissue to a greater or lesser extent (depending on the degree of the deformity), use separate accesses to address all of the causes of lobule deformities, and preserve as much tissue and blood supply as possible. Achieving a successful intervention depends on reducing the tension that affects the entire lobule. Strategies for addressing the different types of deformities and their varying severity are described below.
Helical Tail
Mild deformity
If the helical tail points forward and can be easily palpated, modify its shape with a 20-gage needle (Figure 2A-D). 5 Score the concave helical tail in rectangles through the skin. If tension persists, perform multiple perforations through the cartilage. Because the needle acts as a mini scalpel, consider the direction of the cutting edge.
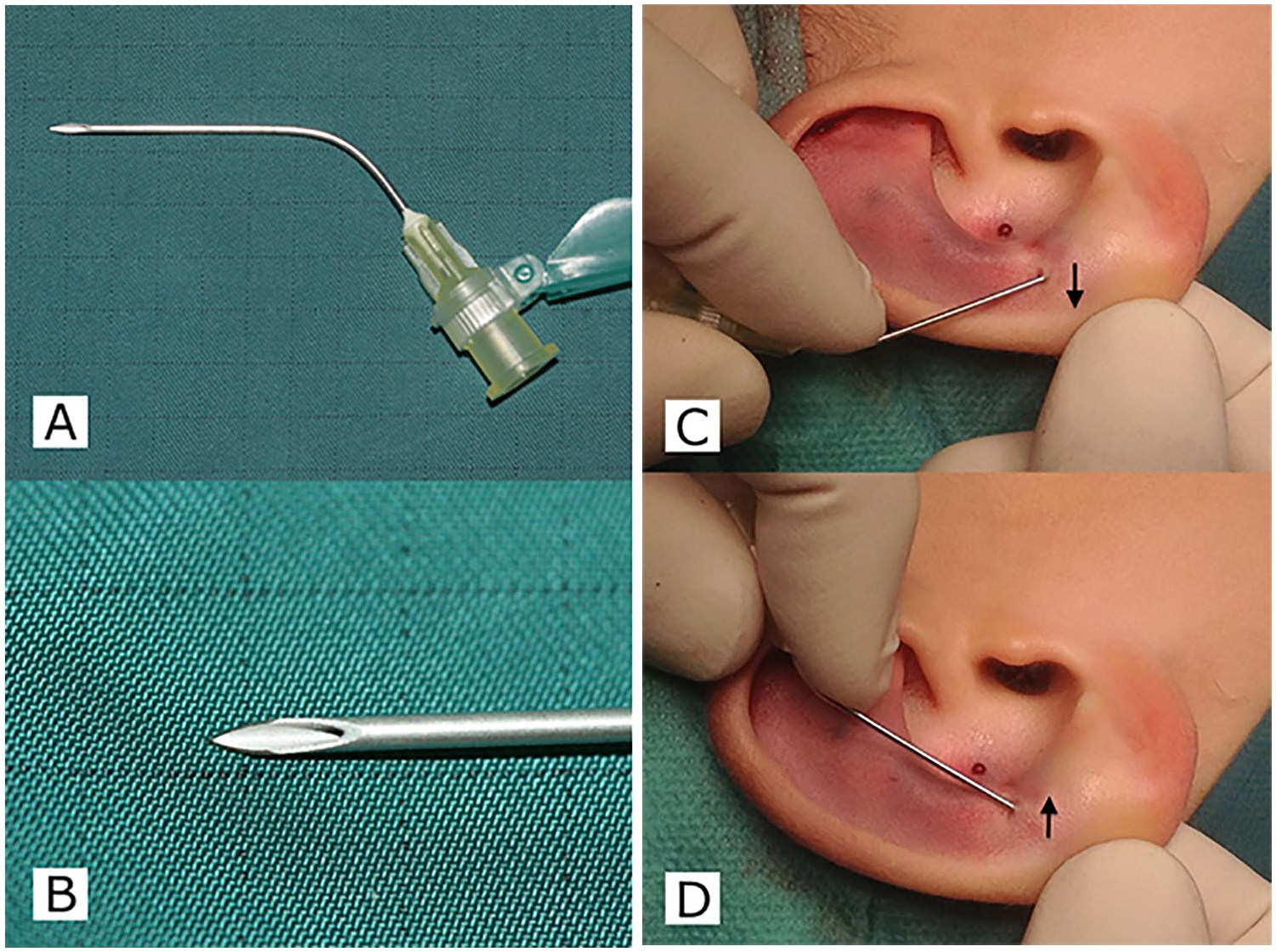
(A) 20-gage needle bent to use as mini scalpel. (B) Close-up of the needle tip to demonstrate the sharp edges. (C, D) Subcutaneous scoring of the helical tail.
Severe deformity
A strong protruding helical tail always occurs in conjunction with a hypoplastic antihelix. Palpate the helical tail posteriorly along the elongation of the sulcus as it emerges from the groove opposite the curvature of the antihelix. Then, perform an oval-shaped skin incision that correlates with the intended degree of posterior skin shortening (Figure 3A, B). Thick helical cartilage does not respond to needling. 5 It will, however, respond to radial stab incisions until there is a significant palpable change in the resilience of the cartilage (Figure 3D). Finally, palpate to ensure the softening of the lobule.
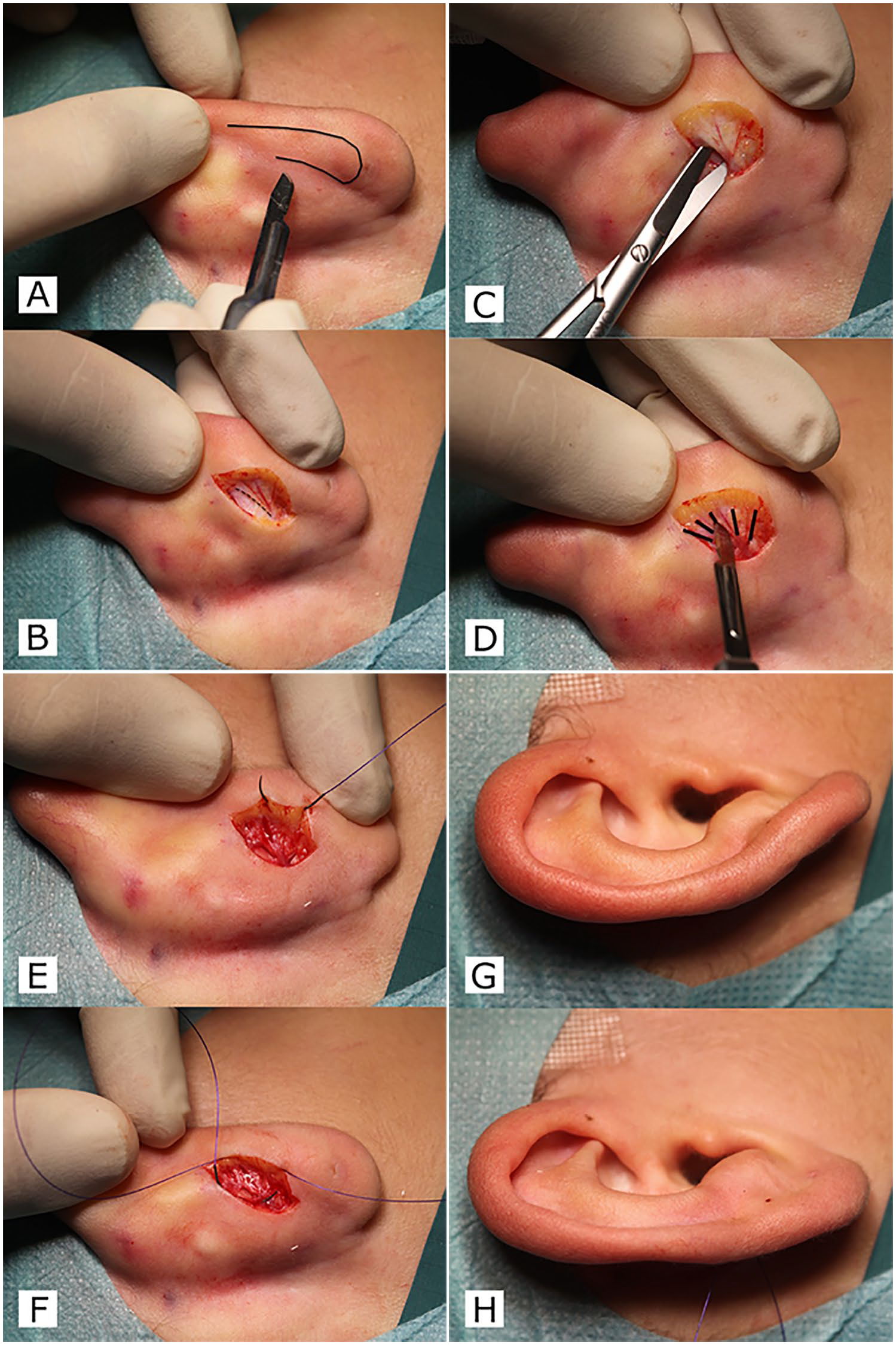
(A) Outline of the helical tail. (B) Oval skin excision in the antihelical-lobule groove. The medial rim of the helical tail is marked in black. (C) Sub-tunneling between the medial rim and conchal cartilage to mobilize the anterior skin. (D) Multiple stab incisions (marked in black) go through the medial rim but preserve the lateral rim. (E) To correct the weakened lobule, the lateral bite goes subcutaneously. (F) The medial bite goes through conchal cartilage. Before (G) and after (H) the procedure.
Soft Tissue
The anterior skin of a normal flat lobule approximates the area of the posterior side. Relatively smaller anterior skin areas cause anterior concavities and protrusions. These concavities can manifest on the horizontal or vertical plane. However, most concavities display a combination of planes. Loosen and stretch the anterior skin to set back and obtain the desired lobule shape. The fat tissue of the lobule is characterized by good blood supply.
Mild deformity
Mild deformities should be addressed with an oval-shaped skin excision followed by subcutaneous long-term absorbable sutures and proper skin closure (Figure 3B, E, F).
Severe deformity
Expose the medial edge of the helical tail. Use blunt-tipped scissors underneath the medial edge of the helical tail to subcutaneously dissect the anterior skin of the lobule as necessary (Figure 3C). This will allow a shift of the shortened anterior skin to all of the affected planes when setting back the lobule. Further resection of the posterior skin can be helpful if the desired shape is not yet acquired.
Preserving the Shape
Preserve the shape of the setback with long-term absorbable subcutaneous sutures (eg, 4-0 Polydioxanone). Insert the lateral bite of the suture subcutaneously, close to the skin and place the second bite in the conchal cartilage to pull the soft tissue in the desired direction (Figure 3E, F). The challenge lies in placing the sutures in the correct direction to compensate for the anterior concavity. Two sutures pulling in different directions are rarely needed to address both the vertical and horizontal planes. After achieving the desired result, close the skin with a short-term absorbable 5-0 Polyglactin 910 suture. Postauricular skin, especially of the lobule, is sensitive to the development of a hypertrophic scar or keloid formations when closed under tension. The subcutaneous Polydioxanone suture is therefore essential to obtain a good result.
Bandage
On completion of the procedure, taping of the lobule in overcorrection to the mastoid for 2 weeks is essential (Figure 4A, B).
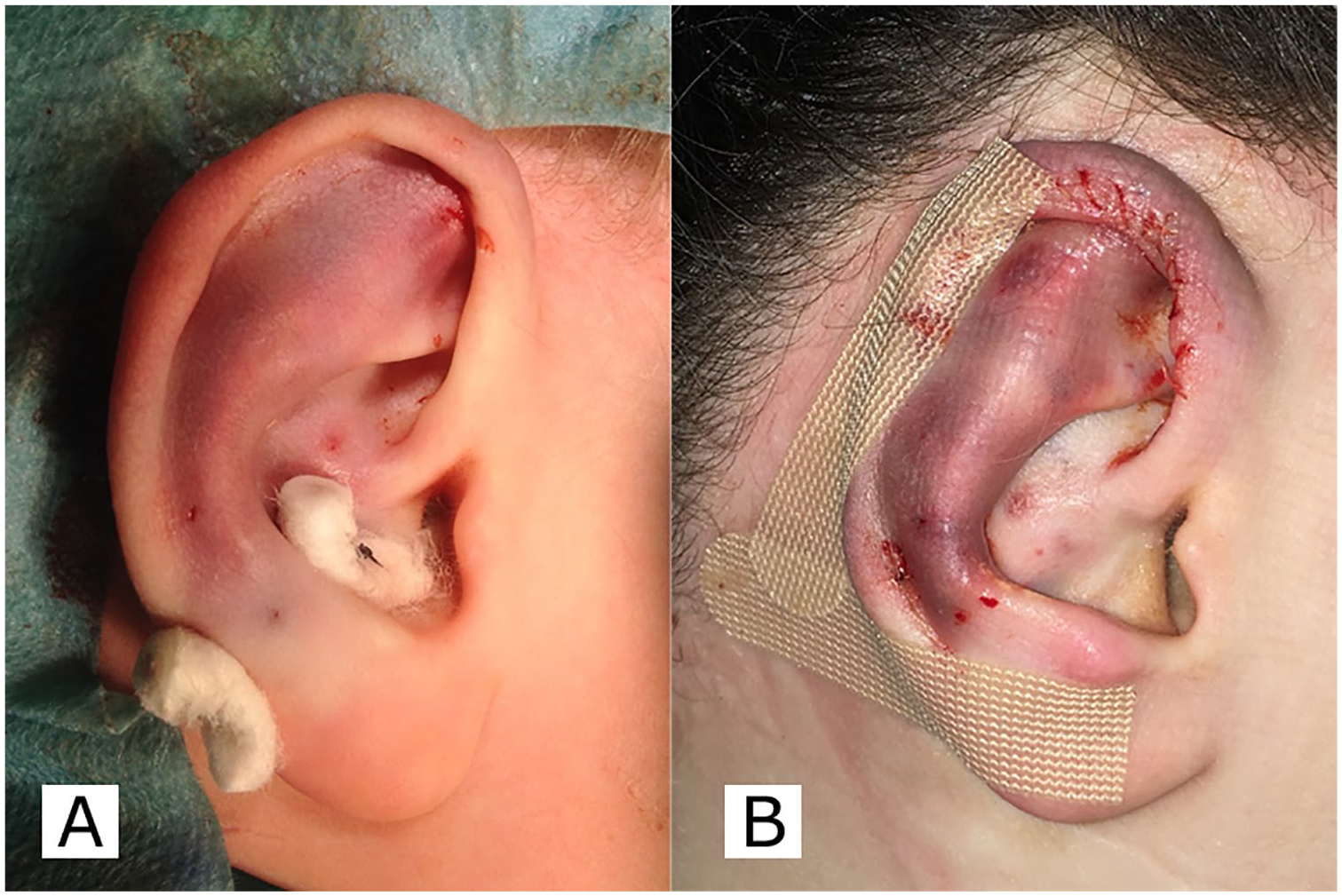
(A) Percutaneous mattress suture supported by cotton wool pads to keep the lobule overcorrected for 1 week (different patient). (B) Taping the lobule in overcorrection to the post auricular skin.
The Aging Lobule
The aging lobule loses fat and soft tissue. It consequently becomes thin, flabby, and unable to support earring studs. To replace the missing tissue and restore a natural look, inject the lobule with hyaluronic acid or lipofilling. Injections close to the anterior skin tighten the lobule and promote a convex shape.
Results
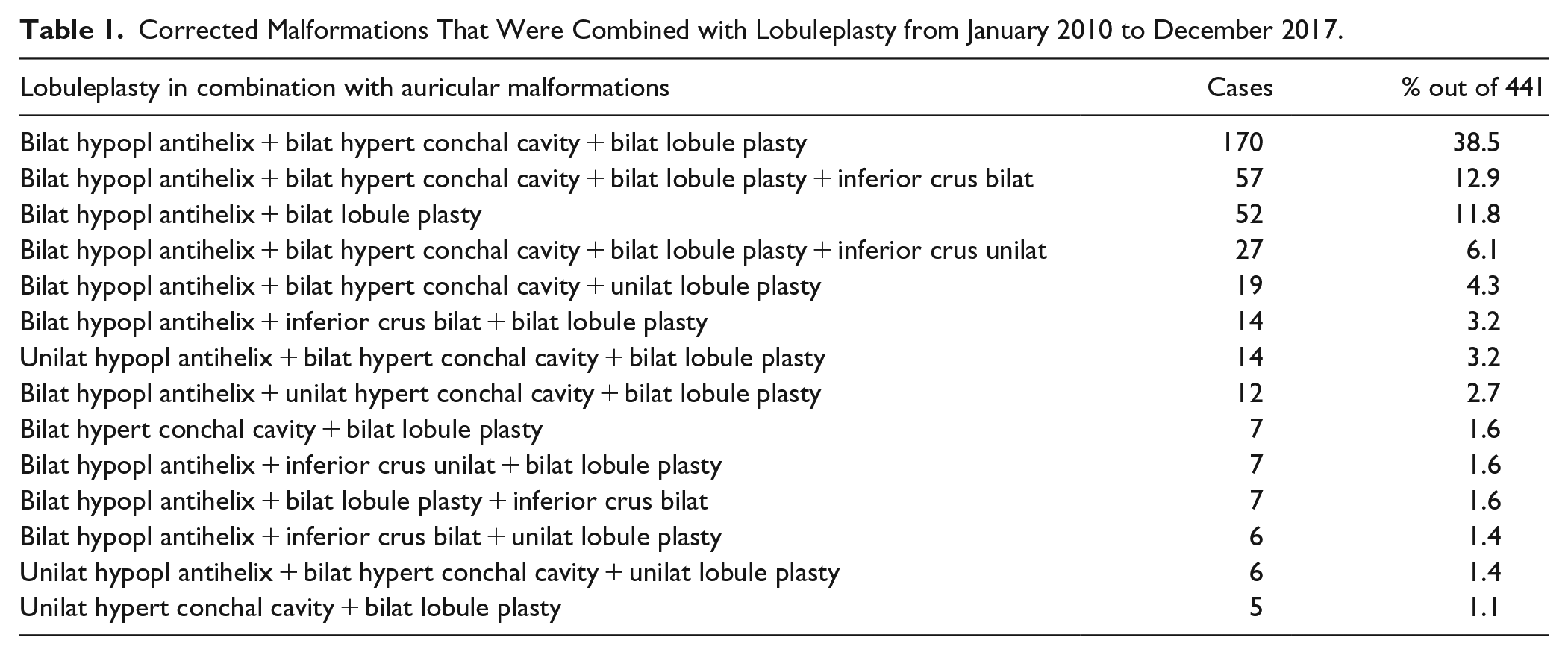
The follow-up period for the 398 patients ranged from 1 month to 8 years. In three cases, the ears, including the lobule, required bilateral revision. One case required a unilateral revision. In most cases, the protruding lobule deformity presented as a combination of hypoplastic antihelix and hypertrophic, conchal cavity abnormalities (Figure 5A-D and Table 1).6,7
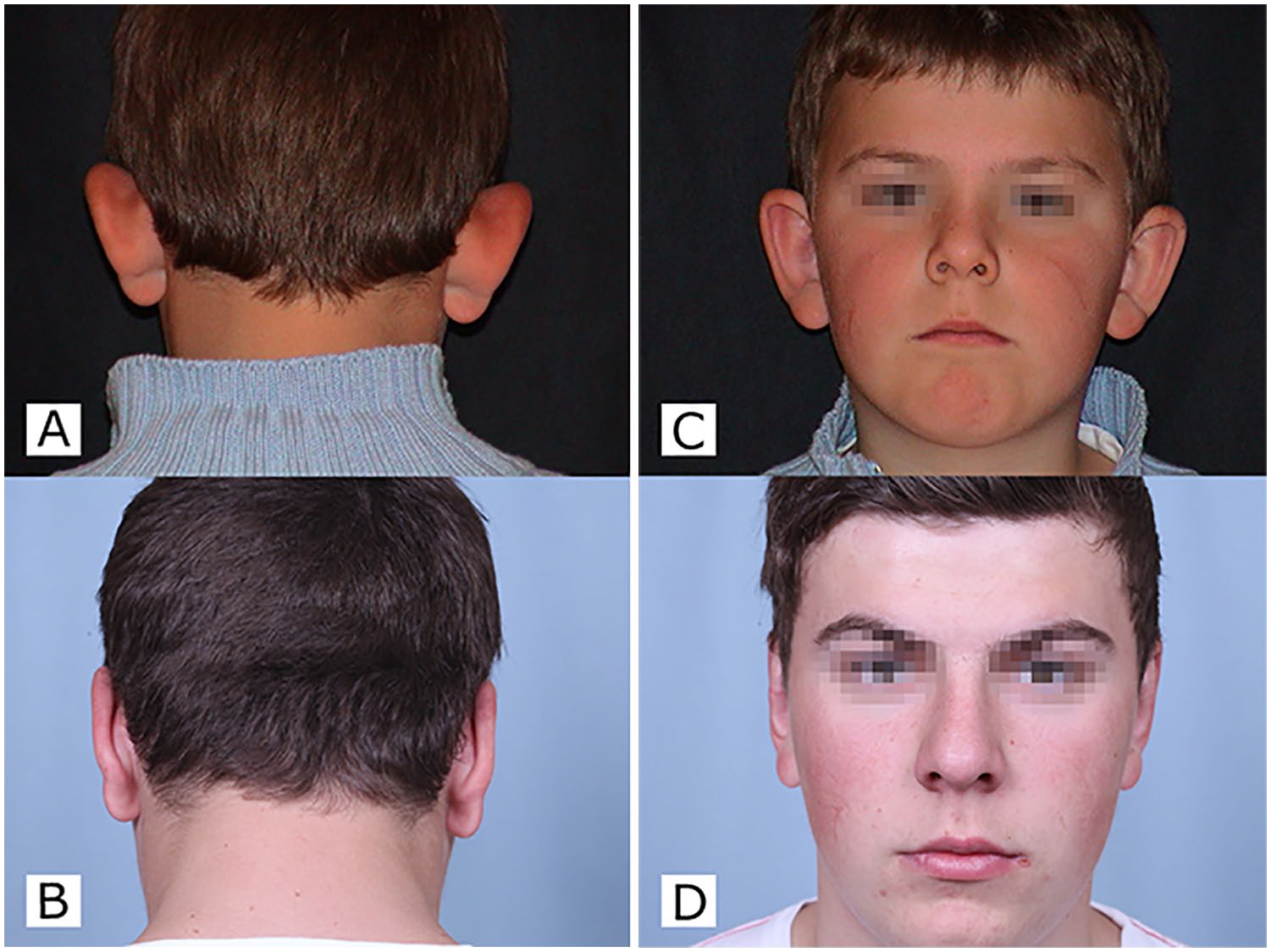
(A, C) Preoperative and (B, D) 8 years postoperative pictures presenting a slightly overcorrected helical tail on the right lobule.
Corrected Malformations That Were Combined with Lobuleplasty from January 2010 to December 2017.
Conclusion
The techniques described in this paper were performed in 398 patients with a very low complication rate. The most important concepts to remember when using this technique are as follows. When analyzing protruding auricles for a setback procedure, understand and respect the degree to which protruding lobules influence the facial appearance. Protruding lobules usually manifest with related deformities, such as a hypoplastic antihelix and hypertrophic conchal cavity (Table 1). To avoid the recurrence of lobule protrusion, release the tension in the soft tissue and the helical tail. Absorbable sutures prevent potential complications associated with permanent sutures.3,5,8
Footnotes
Author Contribution
Conception and design of the study, acquisition of data, analysis and interpretation of data, drafting, and final approval of the paper: Hermann Raunig, Grant Hamilton.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.