
Abstract
Objective:
Identify knowledge deficits about alternate airways (AAs) (tracheostomy and laryngectomy) among physicians across multiple specialties a tertiary institution and to assess the impact of an educational lecture on improving deficits.
Methods:
Study Design: Cross-sectional assessment. Setting: Academic medical center. Subjects and Methods: An anonymous 10-item, multiple choice assessment was given to physicians at a tertiary care center in the departments of Otolaryngology, Emergency Medicine, Family Medicine, General Surgery, Internal Medicine, and Pediatrics. An educational lecture on AAs was presented. Scores between a pre-lecture and a 3-month post-lecture assessment were compared. Data was analyzed using ANOVA and chi-squared analysis.
Results:
Otolaryngology physicians scored an average of 97.8%, while non-otolaryngology physicians scored 58.3% (P < .05). Non-otolaryngology surgical physicians scored 68.4% while non-surgical physicians were lower at 55.1% (P < .0001). Comparing pre-lecture to post-lecture scores, all non-otolaryngology physicians improved their scores significantly from 58.3% to 86.5% (P < .005). Non-surgical physicians had significant improvement after the instructional lecture, closing the score gap with surgical physicians for the post-lecture assessment.
Discussion:
The care of patients with AAs requires an understanding of their basic principles. Our findings identify significant knowledge deficits among non-otolaryngologists. Through an instructional lecture, we demonstrated improvement in knowledge among non-otolaryngology physicians and durability of the knowledge after 3 months.
Conclusions:
Through an instructional lecture, we found tracheostomy and laryngectomy knowledge deficits can be identified and improved upon. Periodic reinforcement of basic principles for non-otolaryngology physicians may be a promising strategy to ensure the proper care of patients with AAs.
Introduction
Patients with alternate airways (AAs) such as tracheostomies or laryngectomies are often encountered in the hospital or clinic setting. Tracheostomy is one of the most common surgical procedures performed on critically-ill patients. 1 Nearly a 100 tracheostomies and approximately 10 laryngectomies are performed every year at the University of California, Davis. However, studies have shown that many non-otolaryngology physicians are unfamiliar or uncomfortable with the care and management of AAs.2-10 Questions regarding basic tracheostomy care and complications of tracheostomy are common consultations placed to the Otolaryngology service. Complications or emergencies involving surgical airways can be devastating and fatal. There appears to be a lack of knowledge regarding the key anatomical differences between different surgical airways such as tracheostomy and laryngectomy.2,3 For patient safety, it is vital that physicians, especially those who may regularly encounter these patients, have adequate knowledge regarding AAs. This study aims to quantify AA knowledge among non-otolaryngology physicians and to determine whether an educational lecture can improve identified knowledge deficits.
Material and Methods
An anonymous, 10-item, multiple choice assessment (Figure 1, answers provided in Supplement 1) was administered to residents, fellows, and attending physicians at the University of California, Davis. The control group consisted of voluntary participants from the otolaryngology department recruited and assessed during departmental grand rounds. The study group included physicians from the departments of Emergency Medicine, Family Medicine, General Surgery, Internal Medicine, Hospital Medicine, and Pediatrics. Participants were recruited from their respective departmental grand rounds. Attendees were asked to complete a pre-lecture assessment on AAs. A 1-hour educational lecture was then presented to the study group by the authors (Supplement 2). The lecture included a PowerPoint presentation reviewing alternate surgical airways during which the 10 assessment questions were covered and answers provided. The audience was also given an opportunity to ask questions. Additionally, tracheostomy tubes, obturators, and other surgical airway-related equipment were provided for familiarization. Three months following the lecture, the same assessment was sent to participants who had completed the initial assessment and attended the lecture via a secure online survey application, Research Electronic Data Capture. The institutional review board at the University of California, Davis approved this study.

Multiple choice assessment*.
Assessments were scored by the authors and the results compared between otolaryngology (control group) and non-otolaryngology (study group) physicians. The study group was further separated into a surgical specialty cohort and a non-surgical specialty cohort for sub-group analysis. Scores of the pre-lecture and post-lecture assessments were compared for the study group by surgical specialty and non-surgical specialty cohorts. Data was analyzed using ANOVA and chi-squared analysis using SPSS (include edition and OS).
Results
A total of 157 responses were received for the pre-lecture assessment with 25 responses from the otolaryngology department and 132 responses from non-otolaryngology departments (Figure 2). Otolaryngology physicians scored an average of 97.8% (SD = 4.22) on the pre-lecture assessment compared to an average score of 58.3% (SD = 20.2) by non-otolaryngology physicians (P < .05) (Figure 3). General surgery physicians scored the highest on average among the non-otolaryngology physicians (Figure 3). When the study group was divided into surgical versus non-surgical specialty cohorts, the surgical cohort scored on average 68.4% (SD = 18.7) compared with the non-surgical cohort which scored on average 55.1% (SD = 19.6) (P < .0001) (Figure 3). Among all non-otolaryngology physicians, lower scores were noted for laryngectomy questions compared to tracheostomy questions (Figure 4).
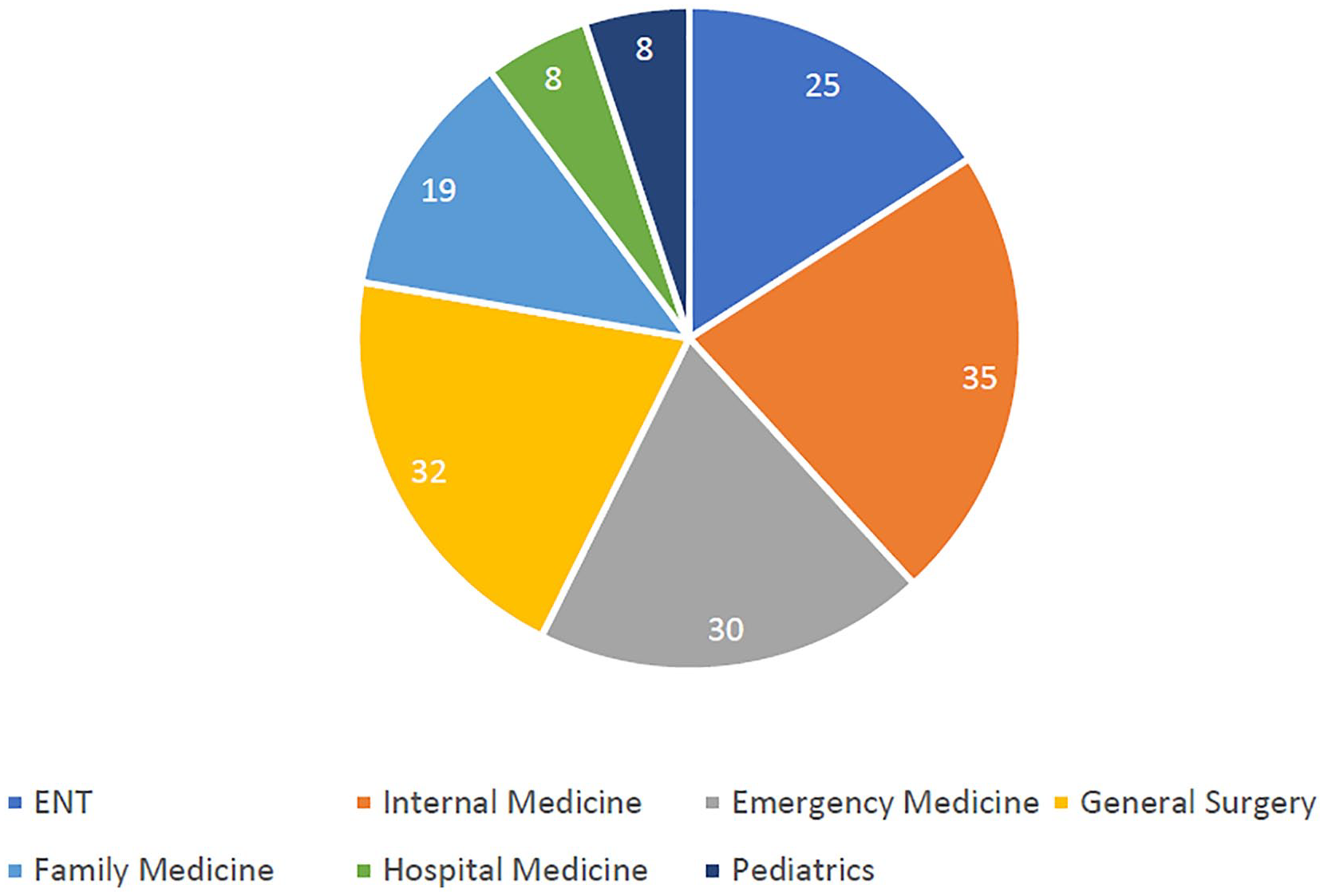
Number of pre-lecture assessment respondents by specialty.
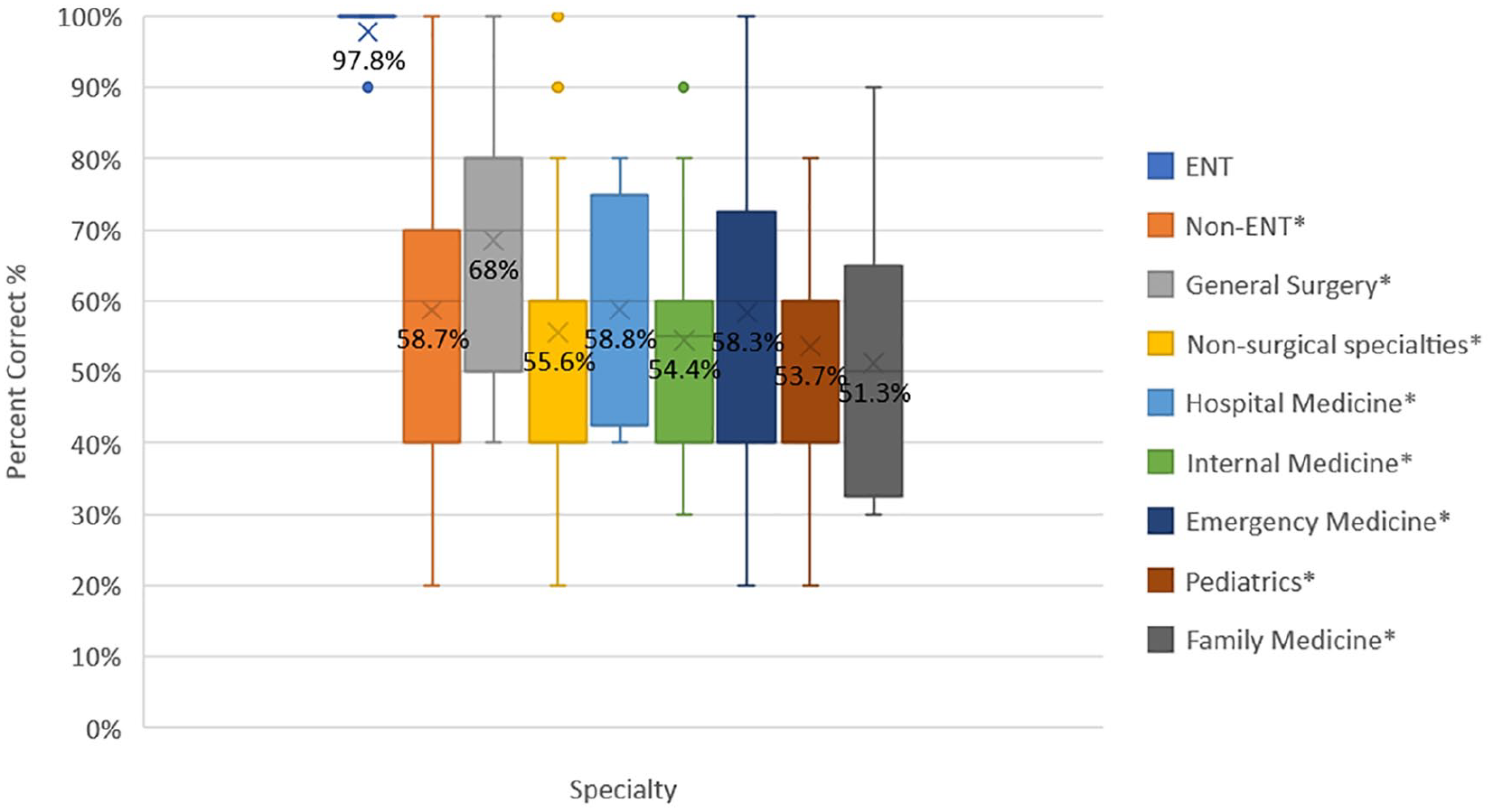
Pre-lecture assessment for control group (otolaryngology) versus study groups (non-otolaryngology) by specialty.
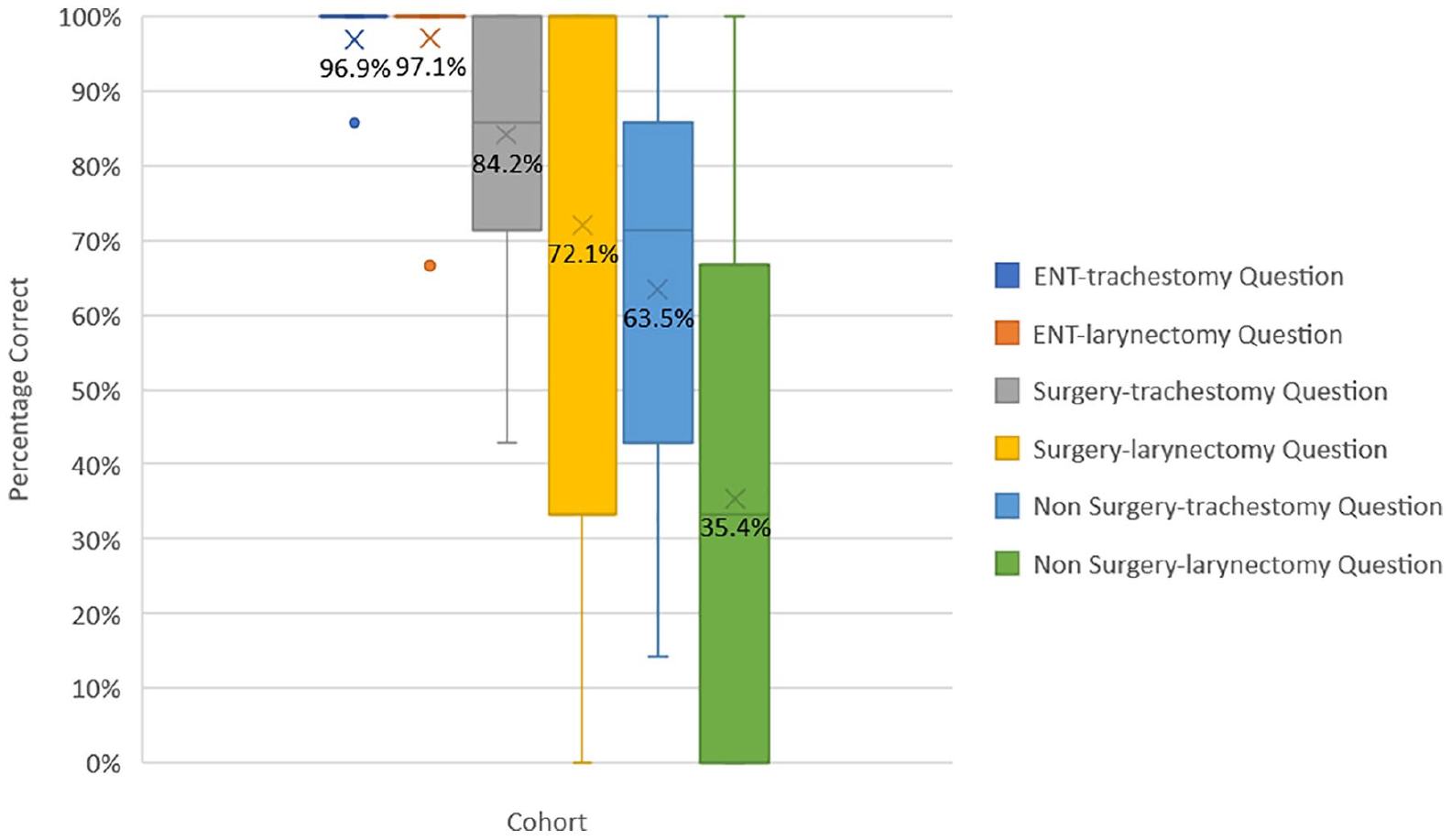
Pre-lecture assessment scores by cohorts and question-type.
A 3-month follow-up assessment was sent to 132 non-otolaryngology physicians who completed the initial assessment and attended the lecture. Thirty-seven responses were returned for a rate of 28%. Comparing pre-lecture scores to post-lecture scores, all non-otolaryngology physicians improved their scores significantly from 58.3% (SD = 20.2) to 86.5% (SD = 10.9) (P < .005). There was a statistically significant improvement (P < .05) on all laryngectomy questions and all but one tracheostomy questions (Figure 5). In addition, the non-surgical physicians had greater improvement after the instructional lecture, closing the score gap with surgical physicians for the post-lecture assessment (Figure 6). Statistical significance of the data was determined using ANOVA and chi-squared analysis.
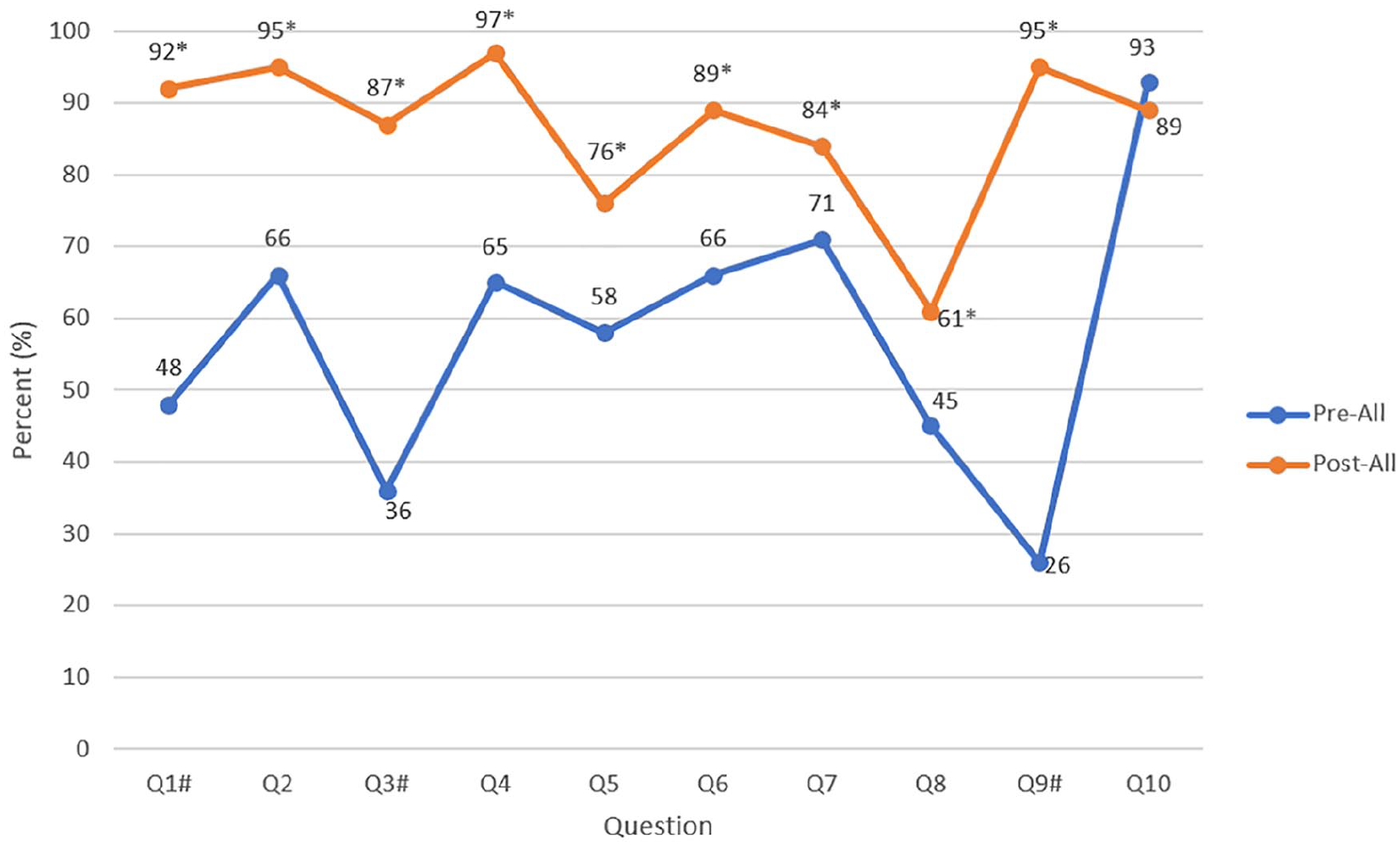
Pre-lecture post-lecture assessment scores for surgical and non-surgical physicians combined. Pound sign (#) indicates laryngectomy question.
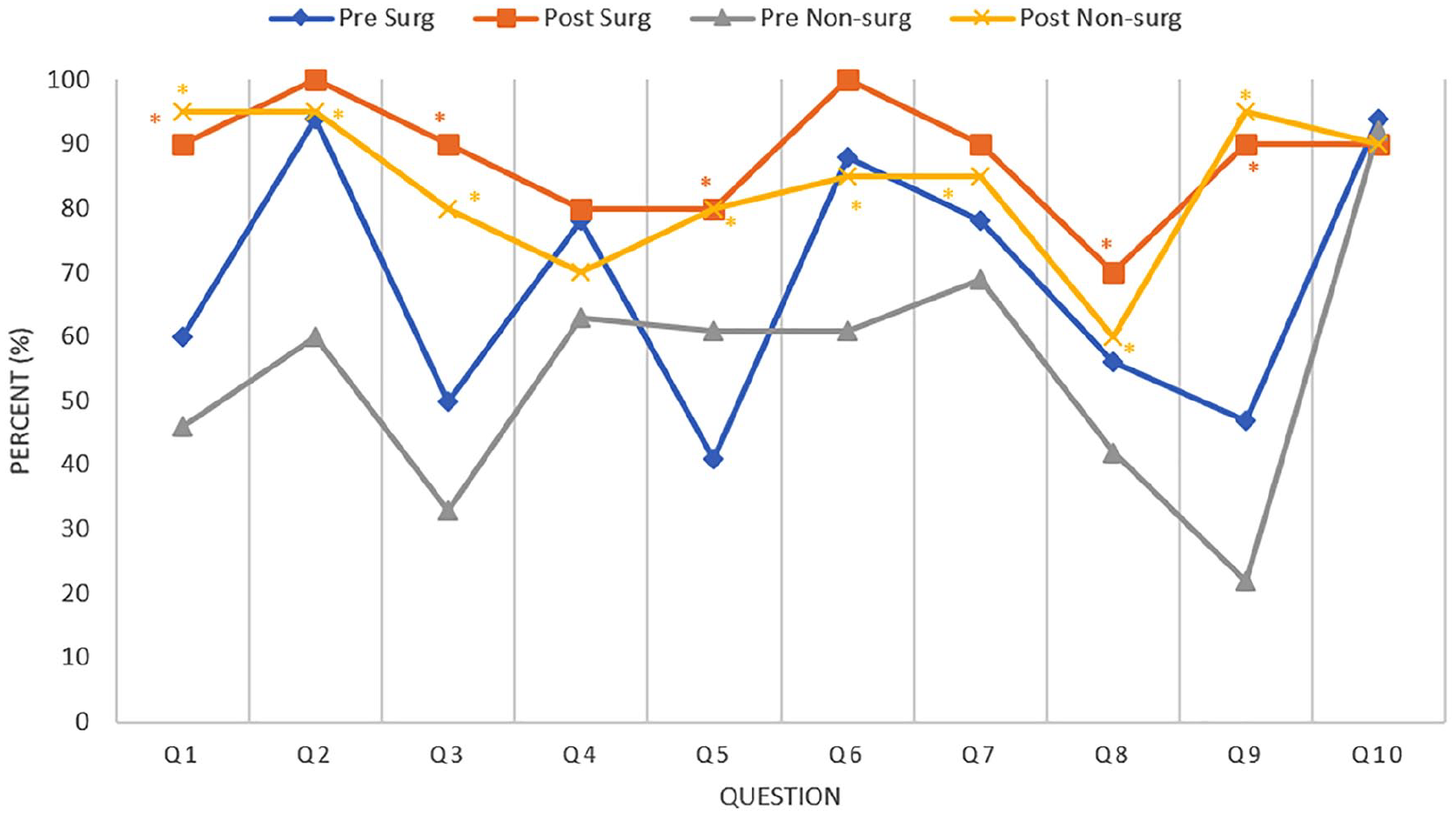
Pre-lecture versus post-lecture assessment scores for surgical versus non-surgical physicians.
Discussion
Our study identified considerable knowledge deficits in non-otolaryngology physicians regarding AAs. Non-otolaryngology physicians had significantly lower assessment scores compared to otolaryngology physicians in basic care and anatomy of tracheostomy and laryngectomy patients. We recruited physicians from multiple departments which allowed us to analyze our results in surgical versus non-surgical cohorts. Among non-otolaryngology physicians, non-surgical physicians were found to have the greatest knowledge deficits. Three months following a 1-hour educational lecture given during departmental grand rounds, all non-otolaryngology physicians improved their scores significantly. Non-surgical physicians were able to improve their assessment scores to match their surgical counterparts. In addition, despite overall poor performance on laryngectomy questions for all non-otolaryngology physicians, this deficit was significantly improved post-lecture. Our study also found there was durability of knowledge at 3 months following the lecture.
Previous studies indicate a need to develop a method to improve basic otolaryngology knowledge among non-otolaryngology physicians and healthcare staff. Casserly et al identified knowledge deficits among non-otolaryngology healthcare staff at two large teaching hospitals regarding tracheostomy-related emergencies. 4 Through a multidisciplinary physician survey, Garner et al found that 97% of internists received little or no residency training in tracheostomy care and this was associated with decreased comfort and willingness to care for these patients. 5 Error et al assessed basic otolaryngology knowledge in residents and medical students and demonstrated deficiencies in both clinical exposure and knowledge. 6 Studies by Whitcroft et al and Darr et al have also identified knowledge deficits in the emergency department setting regarding differences between tracheostomy versus laryngectomy management.2,3
Potential interventions to improve airway knowledge deficits have been studied with promising results. El-sayed et al administered pre-intervention and post-intervention surveys to demonstrate improvement in airway management understanding among physicians, nurses, and respiratory therapists using a bedside Emergency Airway Access form. 7 Dorton et al evaluated the competency of non-otolaryngology healthcare providers in tracheostomy management and incorporated an educational course with patient simulation that was shown to increase provider knowledge and comfort level. 8 In a pediatric study, Agarwal et al implemented a comprehensive simulation-based tracheostomy education program which was shown to improve confidence levels as well as knowledge and skills in healthcare staff at a tertiary care hospital. 9 Lastly, in an evaluating tracheostomy care, Yelverton et al gave an education module on tracheostomies to medical students, nurses, and physicians at an academic center and compared pre-education with post-education quiz scores. They administered their post-education quiz immediately following the module and then again 6 months later. The results of their study found increased knowledge on post-education quizzes both immediately and at 6 months follow-up. 10 Taken together with the results of our study, there is now growing evidence that the care of patients with AAs can be positively affected through simple educational interventions such an educational lecture or module. Our study demonstrated a greater deficit in laryngectomy knowledge as compared to tracheostomy knowledge. However, a statistically significant improvement in knowledge deficits in both these areas was found among non-otolaryngology physicians across specialties that are likely to encounter patients with AAs with retention of that knowledge after 3 months.
A low response rate for the follow-up assessment limits the interpretation of our findings. There is potential for biased responses as those who responded may have felt more comfortable with the topic. Similar to previous studies, our study was conducted at a single academic medical center. Future studies should be aimed at including multiple centers including both academic and private hospitals to determine the efficacy of educational interventions on improving AA knowledge in a larger population and across different clinical settings. In addition, patient-related outcomes should be examined including in-hospital tracheostomy or laryngectomy complications and loss-of-airway deaths.
Conclusion
Our findings identify significant knowledge gaps among non-otolaryngologists concerning the critical topic of AAs. These deficits underscore the importance of improving familiarity with AAs among non-otolaryngologists who will assuredly encounter such individuals in the clinical setting. Through a brief instructional lecture, we have shown that the deficits in knowledge can be identified and improved upon for both tracheostomy and laryngectomy. Future studies can aim to assess the educational efficacy of a lecture versus hands-on simulation. The timeframe for when to repeat an educational curriculum to reinforce important principles is another area that needs to be further elucidated. Periodic reinforcement of basic AA principles for non-otolaryngology physicians may be a promising strategy to ensure the proper care of patients with AAs.
Supplemental Material
Supplement_1_-_Multiple_Choice_Assessment_Answers – Supplemental material for Assessment of Tracheostomy and Laryngectomy Knowledge among Non-Otolaryngology Physicians
Supplemental material, Supplement_1_-_Multiple_Choice_Assessment_Answers for Assessment of Tracheostomy and Laryngectomy Knowledge among Non-Otolaryngology Physicians by Tsung-yen Hsieh, Leah Timbang, Maggie Kuhn, Hilary Brodie and Lane Squires in Annals of Otology, Rhinology & Laryngology
Supplemental Material
Supplement_2_-_Educational_Module_Key_Topics – Supplemental material for Assessment of Tracheostomy and Laryngectomy Knowledge among Non-Otolaryngology Physicians
Supplemental material, Supplement_2_-_Educational_Module_Key_Topics for Assessment of Tracheostomy and Laryngectomy Knowledge among Non-Otolaryngology Physicians by Tsung-yen Hsieh, Leah Timbang, Maggie Kuhn, Hilary Brodie and Lane Squires in Annals of Otology, Rhinology & Laryngology
Footnotes
Authors’ Note
Study previously presented as a poster presentation at AAO-HNS Annual Academy 2014.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.