
Abstract
Objectives:
Examine outcomes of patients 1 month of age or less who received supraglottoplasty. Demonstrate the feasibility and safety of supraglottoplasty in neonates <1 month of age.
Methods:
Charts were reviewed from 2015-2017. Patients with previously identified laryngomalacia requiring surgical intervention and age 1 month or less were identified. We collected data on age, gender, surgical technique, other airway lesions, time to extubation and discharge, and comorbidities.
Results:
Six patients met the inclusion criteria of which four were male and two were female. Average age at time of surgery was 19.5 days. All patients had diagnosis of laryngomalacia made on flexible or direct laryngoscopy with increased work of breathing, reports of cyanotic episodes, or oxygen desaturations. All had feeding difficulties, and three had signs and history consistent with gastroesophageal reflux. Two patients underwent supraglottoplasty by CO2 laser treatment alone, one patient received cold steel treatment alone, and the remaining three patients received cold steel with supplemental microdebrider treatment. Out of six patients, five were extubated within 5 days of their procedure. The average time to extubation was 1.8 days. The average time to discharge was 24.25 days following surgery. Two patients required revisions.
Conclusions:
Supraglottoplasty in children younger than 1 month of age is rare. Despite the rare occurrence, it appears to be feasible early in life in treating laryngomalacia. Neonates with respiratory failure, apneas, and cyanosis, or difficulty feeding due to laryngomalacia should be evaluated and treated with supraglottoplasty.
Keywords
Introduction
Laryngomalacia is the most common cause of stridor in the neonate. 1 Patients typically present with symptom severity ranging from occasional or positional stridor and mild feeding symptoms to constant stridor, failure to thrive, cyanotic spells/hypoxia, and obstructive sleep apnea with serious sequelae such as cor pulmonale and pectus deformities. Symptoms worsen until age 4 to 6 months, after which they decrease and resolve by age 18 to 24 months. 2 The majority of patients diagnosed with laryngomalacia can be treated conservatively. However, approximately 10%-15% of patients present with symptoms severe enough to require surgery. Supraglottoplasty is the current surgery of choice. Although the average age at surgery ranges from 3.8 to 5.5 months, 1 in some cases, symptom severity requires surgery in patients <1 month of age. Patient factors that influence disease severity include Apgar scores, resting oxygen saturation level at time of presentation, and the presence of a synchronous airway lesion. 3 While age at the time of surgery and gestational age have not been shown to be a statistically significant factors for post-supraglottoplasty outcomes, there is scant information on outcomes of laryngomalacia in neonates 1 month of age requiring supraglottoplasty.4,5 The goal of this study is to examine outcomes of patients 1 month of age or less who received supraglottoplasty and to demonstrate the surgical feasibility in this age group.
Methods
A single institution, tertiary care center retrospective review was performed to compare indications for surgery, surgical techniques, and postoperative outcomes. Internal review board (IRB) approval was obtained for a retrospective chart review. Charts were reviewed from 2015 to 2017. Inclusion criteria included patients with previously identified laryngomalacia requiring surgical intervention and age 1 month or less. Exclusion criteria included age >1 month and laryngomalacia that was medically managed at home. Relevant data points included age at the time of surgery, gender, surgical technique, synchronous airway lesions, time to extubation, time to discharge, and gestational age.
Results
Six patients met the inclusion criteria of which four were male and two were female. Average age at time of surgery was 19.5 days. All patients had diagnosis of laryngomalacia made on flexible or direct laryngoscopy with increased work of breathing with hypoxia and reports of cyanotic episodes or oxygen desaturations. Two of the six were intubated and failed attempts at extubation—one of these two was the only patient with a synchronous airway lesion—grade 1 subglottic stenosis. All had reported feeding difficulties. One had dysphagia that persisted after supraglottoplasty; he eventually required placement of gastrostomy tube. Additionally, three patients had erythema and edema of arytenoids and post-cricoid space on airway evaluation, along with history consistent with gastro esophageal reflux (GER); one of these patients had a pH probe to confirm the diagnosis.
Two patients underwent CO2 laser treatment alone, one patient received cold steel treatment alone, and the remaining three patients received cold steel with supplemental microdebrider treatment. Out of six patients, five were extubated within 5 days of their procedure. The average time to extubation was 1.8 days. The average time to discharge was 24.25 days following surgery. Two patients required revisions and one ultimately required tracheostomy. The patient who remained intubated had multiple comorbidities, including maternal methamphetamine abuse, neonatal encephalopathy, and grade 2 intraventricular hemorrhage (IVH). Throughout his admission, he demonstrated no neurologic progress and had poor neurologic prognosis, which lead to eventual withdrawal of care 3 months following surgery. Our results are depicted in Table 1. Figure 1 shows photos of a larynx before and after supraglottoplasty.
Patient data. Six patients underwent supraglottoplasty at age less than one month.
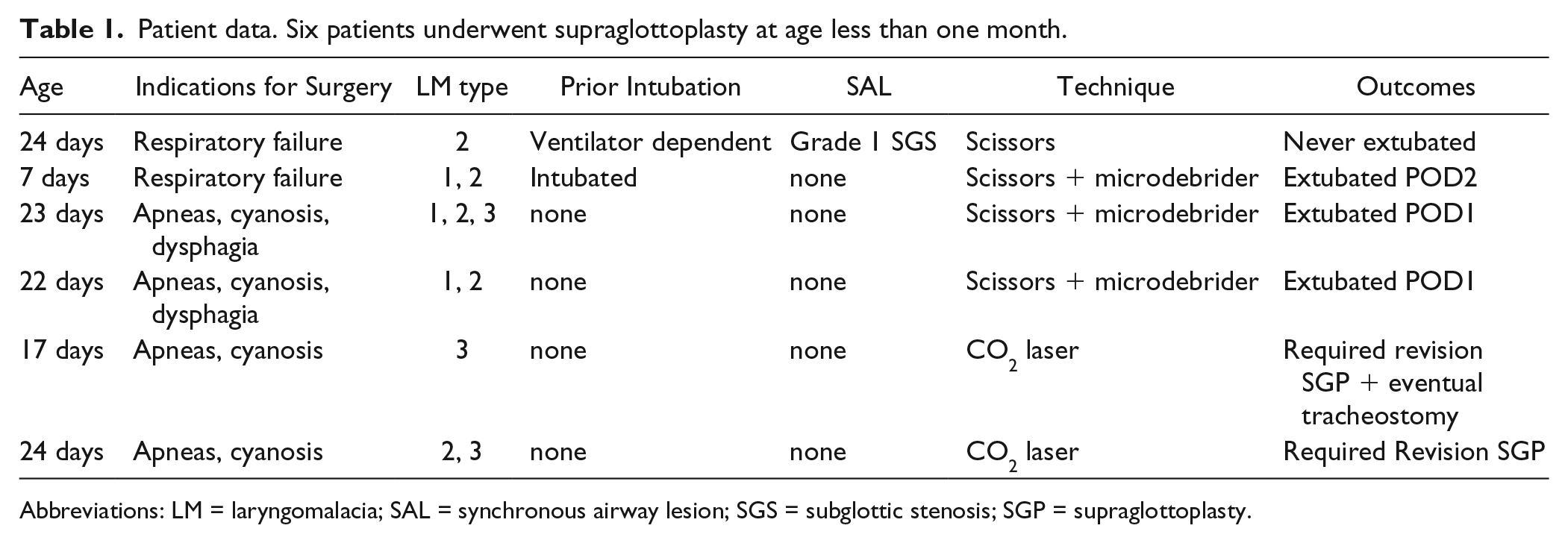
Abbreviations: LM = laryngomalacia; SAL = synchronous airway lesion; SGS = subglottic stenosis; SGP = supraglottoplasty.
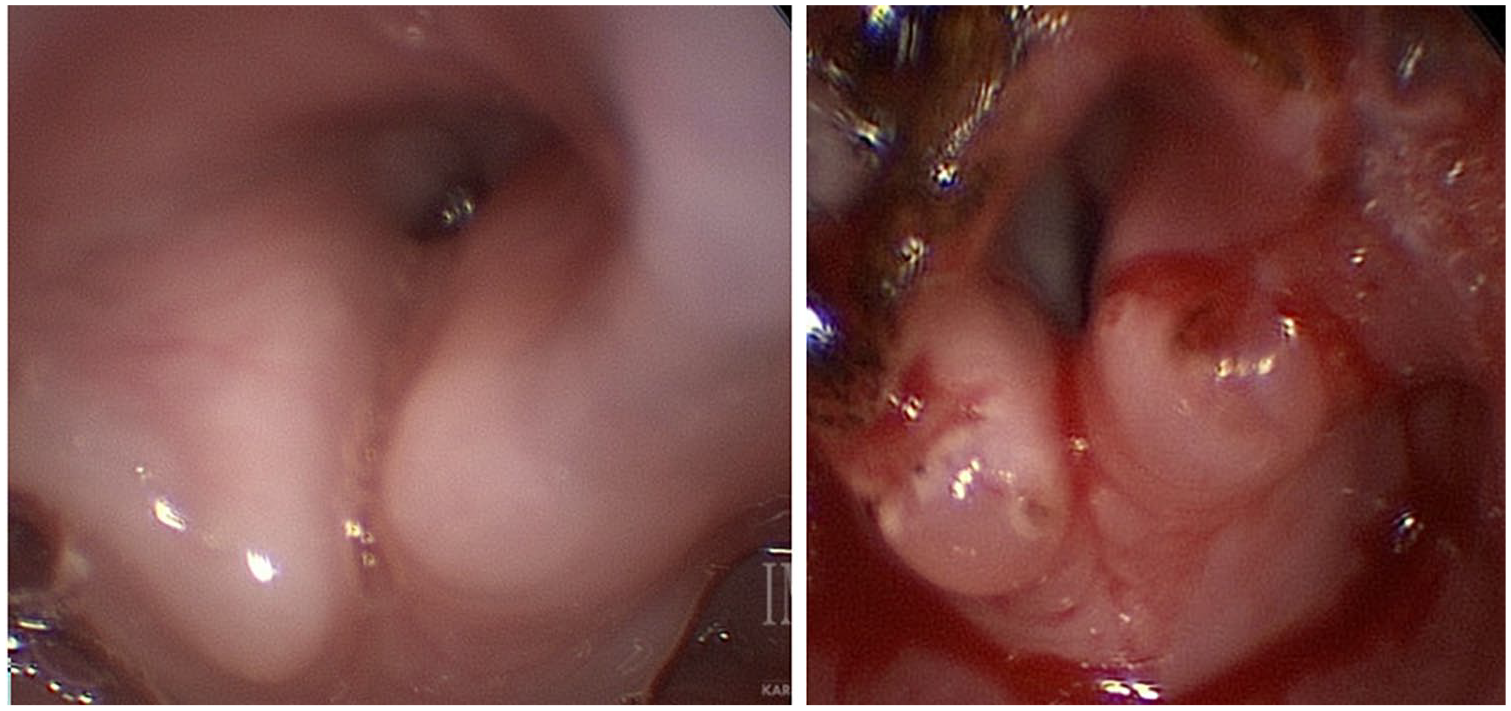
Photos of larynx before and after supraglottoplasty.
Discussion
Supraglottoplasty continues to be the surgery of choice for laryngomalacia that does not respond to medical management or with severe sequela. The average age at surgery for supraglottoplasty is reported to be between 3.8 to 5.5 months. Patients who require supraglottoplasty at age <1 month either have severe laryngomalacia causing respiratory distress, or have significant apnea and cyanosis often with feeds, causing alarm among caretakers. Two of our patients required intubation prior to surgery with laryngomalacia as the principle airway lesion seen on exam (one of these also had grade 1 subglottic stenosis).
While it has been shown that earlier presentation of laryngomalacia and subsequent need for supraglottoplasty suggests a more severe disease process, the effect of age at date of procedure on neonatal outcomes has not been fully elucidated. One study reported that among non-comorbid patients <2 months of age at the time of surgery, there was a significantly increased rate of revision when compared with infants between 2 and 10 months of age. 6 Others have found no significant difference in outcome of supraglottoplasty when comparing patients grouped either <2 months old or greater. 7 The possibility and practicality of supraglottoplasty at an early age needs more data to develop clear guidelines.
Most laryngomalacia types are isolated, but 15% are combined. Type I is due to prolapsed arytenoids, Type II includes foreshortened aryepiglottic folds, and Type III consists of prolapsed or overhanging epiglottis. 8 Only two out of our six patients had an isolated type of laryngomalacia reported. The combination of laryngeal anomalies in our remaining neonatal patients may correlate with increased severity of symptoms. Synchronous airway lesions (SAL) have been shown to be present in a high number of laryngomalacia cases. These may include hypoplastic mandible, subglottic stenosis (SGS) >35%, laryngeal edema, and others. 9 One patient in our study was found to have a SAL—grade 1 SGS—but no other patients did, suggesting that SALs may not play a significant part in early presentation and subsequent need for treatment of laryngomalacia.
Surgical techniques include cold steel and radiofrequency ablation. Our supraglottoplasty surgeries were safely performed in neonates with steel, CO2 laser, and microdebrider. Recent studies suggest no difference in outcome between laser versus cold steel techniques. 10 In this study, the surgery was safely performed in neonates with all techniques without complication. However, the two patients in our study who were treated with CO2 laser needed revision supraglottoplasty, and one required tracheostomy. Due to our small sample size and overwhelming research in the literature that suggests no difference between cold steel and laser technique, we do not feel this is a significant finding. While CO2 laser is feasible, family counseling should include discussion of possible revisions and surgery should be approached with caution.
In general, success rates for supraglottoplasty range from 53% to 95%, with success defined as improvement in respiratory status and feeding problems. In our cohort of neonates, three out of six patient experienced improvement after extubation without requiring further airway surgery—slightly below the above reported success rate. This lower success rate is possibly the result of increased comorbid conditions.
Conclusion
Supraglottoplasty in children younger than 1 month of age is rare. Patients who present early with laryngomalacia appear to have more severe symptoms associated with feeding difficulties and prolonged hospital stays. Although it is rarely indicated, supraglottoplasty for laryngomalacia within 1 month of life appears to be feasible, and current instrumentation is able to accomplish this with end results comparable to that in older infants. Similar techniques used in older infants are safely used in neonates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.