
Abstract
Objective:
The incidence of occult metastasis (OM) in laryngeal squamous cell carcinoma (SCC) is still widely debated. In this systematic review, we aim to determine the rate of OM in laryngeal SCC, its impact on recurrence, and the role of elective neck dissection (END) in the management of the clinically negative neck.
Methods:
A systematic review of the English-language literature in Web of Science, PubMed, MEDLINE, and Cochrane Library databases on occult metastasis in laryngeal SCC from 1977 to 2018 was conducted. Studies evaluating occult metastasis (OM) in patients with laryngeal SCC with clinically negative necks undergoing surgery were included. Studies evaluating other head and neck subsites, clinically node positive, and salvage patients were excluded.
Results:
Twenty-one articles with a total of 5630 patients were included. The overall rate of OM was 20.5% and was 23% and 12.2% in supraglottic and glottic tumors, respectively. The OM rate in T1-T2 tumors was 13% and 25% in T3-T4 tumors. T3-T4 tumors had significantly greater odds of developing OM compared to T1-T2 tumors (Odds Ratio [OR] = 2.61, 95% Confidence Interval [CI] = 1.92-3.55, P < .00001). Patients with OM were more likely to develop distant metastasis (OR = 5.65, 95% CI = 3.36-9.51, P < .00001).
Conclusions:
Patients with advanced T-stage laryngeal SCC should undergo elective neck treatment. More aggressive treatment for patients with history of OM should be considered due to the risk of subsequent regional and distant metastasis.
Level of Evidence:
II
Keywords
Introduction
The presence of metastatic cervical lymph node disease in laryngeal SCC has a noteworthy negative impact on survival. 1 Despite the implementation of modern imaging modalities, clinical detection of metastatic disease in cervical lymph nodes remains challenging. It is now apparent that occult lymph node metastasis is not an uncommon occurrence in SCCs of the head and neck, particularly in supraglottic laryngeal carcinomas.2-4 This is believed to be due to the presence of robust lymphatic networks within this anatomical region, leading to cervical metastasis most frequently to level II and III lymph nodes. 2 Although early stage glottic carcinoma is established to have a low incidence of cervical metastasis (0-10%), the described incidence with more advanced stage carcinoma historically varies between 10% and 35%. 5
A classic approach to the treatment of supraglottic and advanced T-stage glottic laryngeal SCC with no clinical evidence of lymph node involvement on examination and radiological imaging is surgical intervention with bilateral elective neck dissection (END).6,7 In most institutions, occult metastasis rates exceeding 15% to 20% represents the threshold for proceeding with elective neck treatment due to the weighted risk of recurrence compared to the risks of overtreatment.8,9 Prior studies that provide quantitative data on the rates of occult cervical lymph node metastasis in laryngeal carcinomas report conflicting figures, and consequently make contradictory recommendations for the approach to elective neck treatment.3,10-12 To date, only one systematic review of the literature on occult metastasis in supraglottic laryngeal SCC has been published by Goudakos et al in 2009. 3 Unfortunately, due to the heterogeneity of their data, they were unable to perform a meta-analysis. In this study, we present an updated systematic review and meta-analysis of existing literature that reports on rate of occult metastasis in primary laryngeal SCC across subsites, its impact on recurrence, and the utility of END for the clinically negative neck.
Materials and Methods
A systematic review of the published literature on occult metastasis and elective neck dissection in laryngeal squamous cell carcinoma was performed. This study met criteria for nonhuman subject research, and approval by the Institutional Review Board of Augusta University was, therefore, not required.
Search Strategy
Review of the literature was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 13 A search of the Web of Science (WoS), PubMed, MEDLINE, and Cochrane databases was performed with the following search terms, “supraglottic,” “laryngeal cancer,” and the combination of terms “laryngeal cancer” AND “occult metastasis.” The search was completed in November 2018. Study results were limited to English-language articles that evaluated human subjects. All abstracts were evaluated, and full-text articles of those found to fulfill inclusion criteria were obtained. Reference sections of the included full-text articles were then reviewed for additional potential articles for inclusion.
Selection Criteria
Studies evaluating rates of OM in patients with clinically negative necks who underwent primary surgery for laryngeal SCC were included. Studies that evaluated salvage surgery, other head and neck subsites outside of the larynx, sentinel lymph node biopsy, and clinically node-positive patients were excluded. Foreign-language, review, or irrelevant studies and studies with insufficient data were excluded. Two investigators (D.S. and M.A.) independently performed the search review to determine that all appropriate articles were included in the analysis.
Data Extraction
Variables included author, publication year, study type, sample size, patient demographics, rate and location of occult metastases, surgical interventions performed, tumor staging and characteristics, follow-up time, recurrence, and overall survival (OS) were collected.
Assessment of Study Quality and Bias
The Newcastle-Ottawa Quality assessment scale for observational studies was used to grade studies included in the final review.14,15 Scales for selection (****), comparability (**), and outcomes (***) were used with a greater number of asterisks indicating higher quality. Two investigators (D.S. and M.A.) independently performed the quality assessment.
Statistical Analysis
Study results were combined into meta-analyses based upon similarity of reported outcomes. Aggregated results comparing patients by T-stage, tumor histopathologic grade, extralaryngeal spread, cartilage invasion, occult metastatic nodal status, and regional and distant recurrence events were reported using odds ratios (OR) and 95% confidence intervals (CI’s) with a significance level of P = .05 used for all analyses. A fixed-effects model was employed in the meta-analyses, and the I2 statistic was used to quantify analysis heterogeneity. When significant heterogeneity was present (P < .05, I2 ≥ 25%), a random effects model was used. Data analyses were performed with Cochrane Review Manager version 5.3 (Nordic Cochrane Center, Cochrane Collaboration, 2014).
Results
Study Selection
A total of 5970 studies were identified through database searching and identification of records through other sources (Figure 1), and 4333 titles and abstracts were screened for inclusion after duplicates were removed. Eighty-three articles were subsequently identified for screening. Nine articles were deemed to be irrelevant, and 72 full-text articles were then assessed for eligibility. Fifty-one articles were excluded due to failure to meet inclusion criteria. Twenty-one articles were included for qualitative synthesis, and 18 articles were able to be included for pooled data synthesis in evaluating prevalence and outcomes data.1,8,9,11,12,16-31 Notably, one large 1996 study by Gallo et al evaluating END versus observation in 1808 patients was specifically excluded due to the high likelihood of patient overlap with the same authors’ reported data in 2207 patients from 2006.9,32
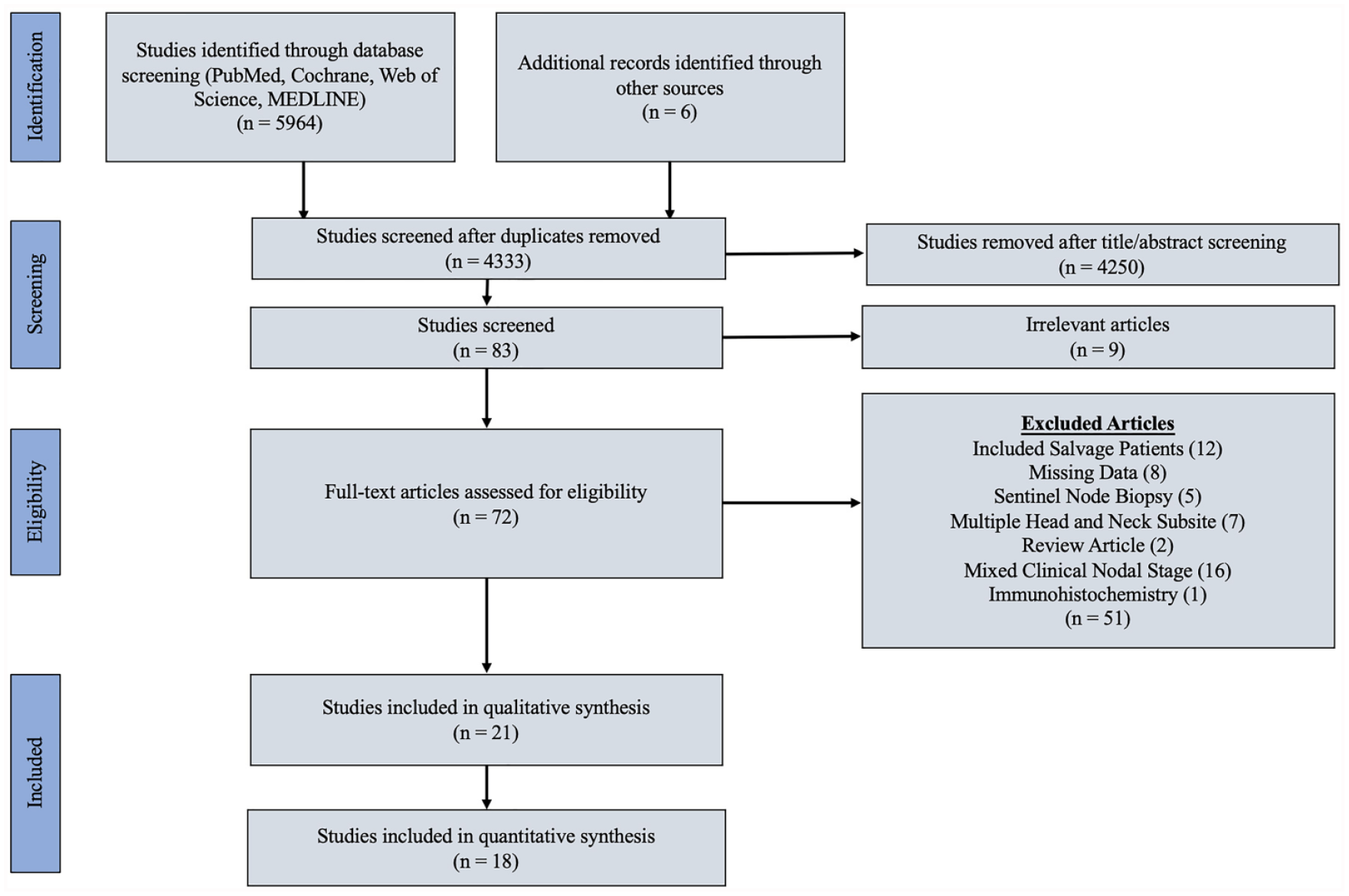
PRISMA compliant flow chart.
Study Characteristics and Patient Groups
Details regarding study characteristics can be found in Table 1. A total 5630 patients were included. Most studies evaluated cancers at multiple laryngeal subsites including the supraglottis/epilarynx, glottis, and subglottis as well as transglottic tumors. Eight studies evaluated patients undergoing only bilateral END and 13 evaluated patients undergoing both ipsilateral and bilateral END. Nine studies reported total lymph nodes removed, and five studies reported total number of positive lymph nodes.
Study Characteristics.
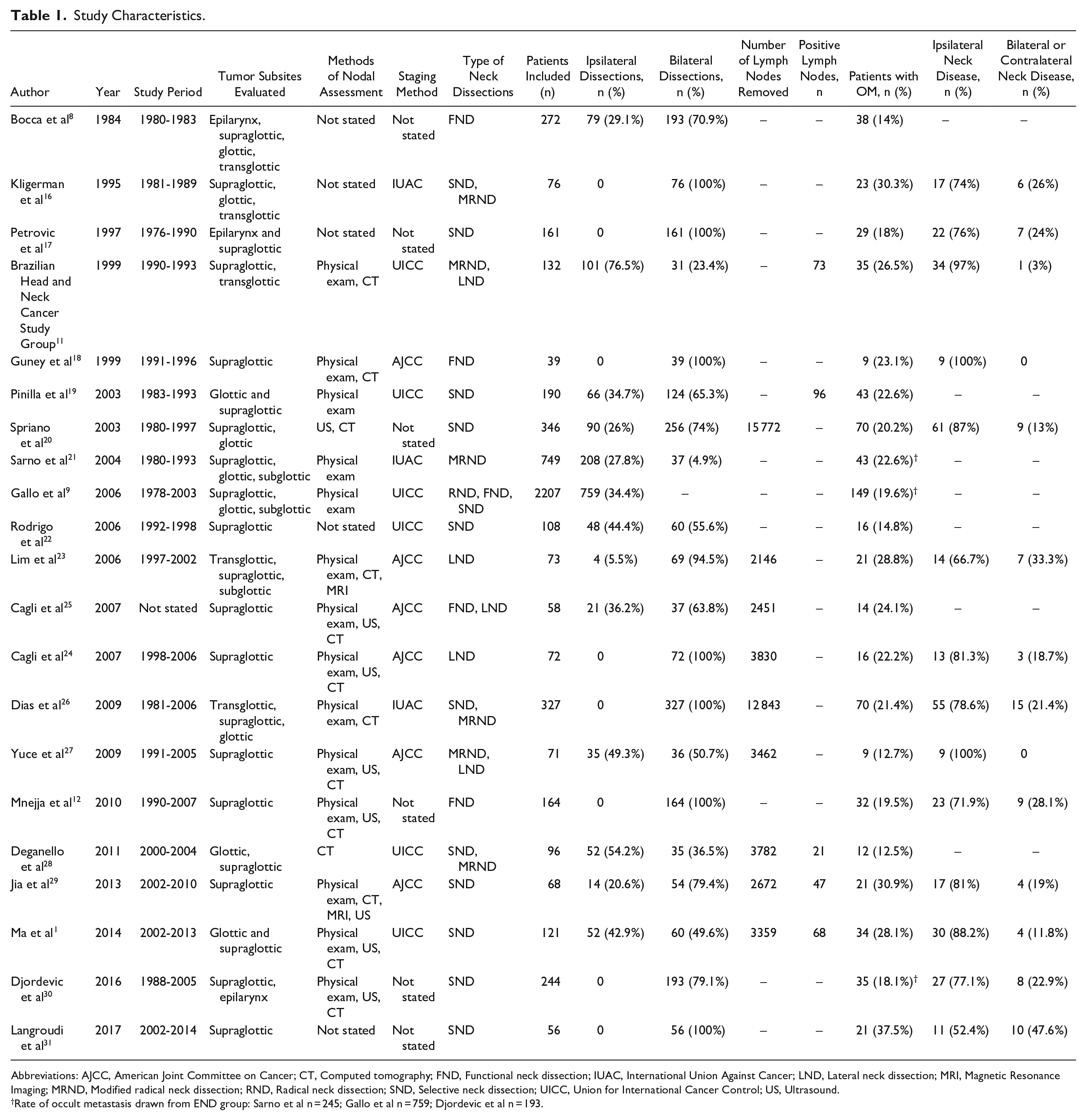
Abbreviations: AJCC, American Joint Committee on Cancer; CT, Computed tomography; FND, Functional neck dissection; IUAC, International Union Against Cancer; LND, Lateral neck dissection; MRI, Magnetic Resonance Imaging; MRND, Modified radical neck dissection; RND, Radical neck dissection; SND, Selective neck dissection; UICC, Union for International Cancer Control; US, Ultrasound.
Rate of occult metastasis drawn from END group: Sarno et al n = 245; Gallo et al n = 759; Djordevic et al n = 193.
Assessment of Study Quality and Bias
Assessment of the overall methodological quality of studies using the Newcastle-Ottawa Scale can be found in Table 2. The overall reported quality of the studies included was poor, as most were retrospective cohorts of patients who underwent elective neck treatment. Three studies comparing patients undergoing END versus observation with subsequent therapeutic neck dissection were of better quality.9,21,30 These three studies scored high on the selection subscale indicating appropriate representativeness of the exposed cohort, selection of the non-exposed cohort, ascertainment of exposure, and the demonstration that the outcome of interest was not present at the beginning of the study. Additionally, these studies controlled for tumor subsite, and two of them controlled for T-stage.
Risk of Bias Assessment.
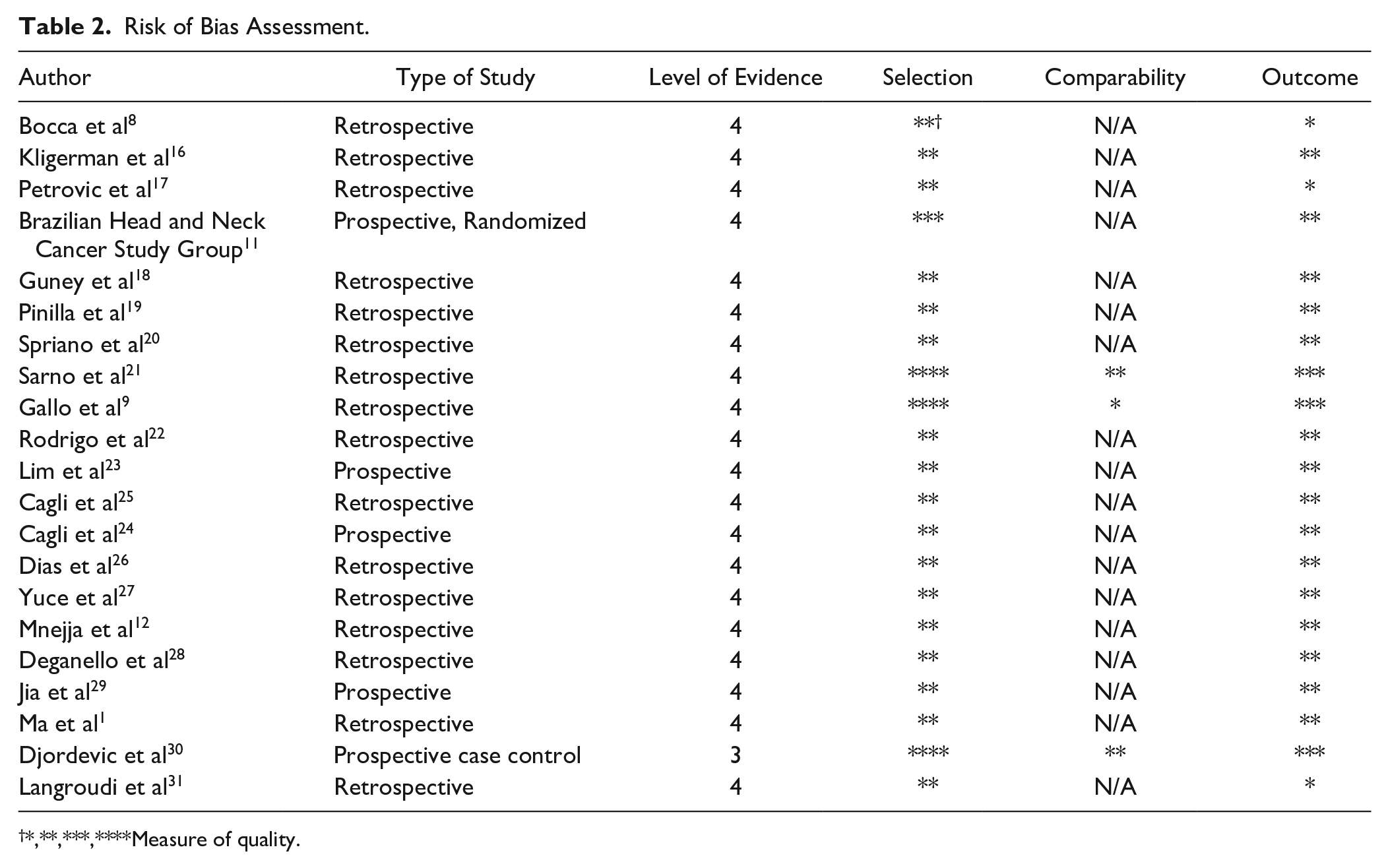
*,**,***,****Measure of quality.
Aggregate Rates of Occult Metastasis
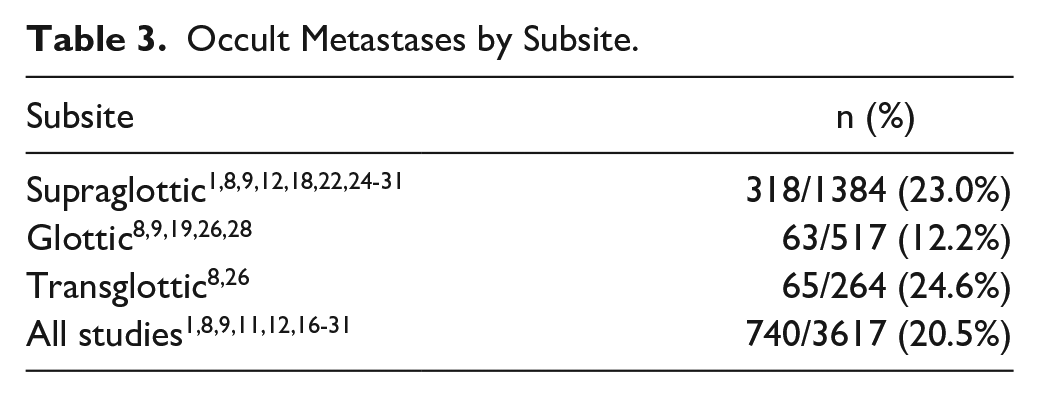
Table 3 demonstrates rates of OM by subsite. The overall rate of occult nodal metastasis was found to be 20.5%. The rate of occult metastasis by subsite was 23% in supraglottic tumors, 12.2% in glottic tumors, and 24.6% in transglottic tumors. Figure 2 demonstrates the location of neck metastases by level from 481 patients in 11 studies.1,9,11,12,20,23,24,27-30
Occult Metastases by Subsite.
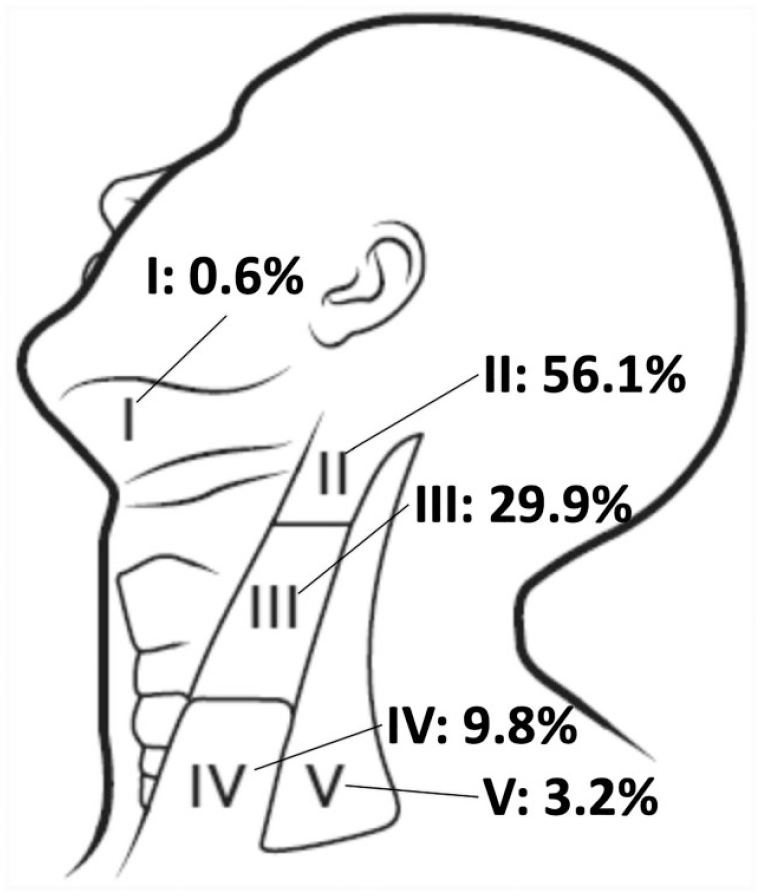
Distribution of occult metastases by neck level.
Meta-Analysis of Outcomes
Across thirteen studies covering all laryngeal subsites, 25% of patients with T3-T4 tumors demonstrated OM, while just 13% of T1-T2 patients demonstrated OM.1,8,11,12,17,19,24-29,31 Patients with T3-T4 tumors were found to have a significantly greater odds of developing OM compared to T1-T2 patients (OR = 2.61, 95% CI = 1.92-3.55, P < .00001, I2 = 0% Figure 3A). In the subgroup of seven studies evaluating odds of OM across T-stage in supraglottic tumors, 31.6% of patients with T3-T4 tumors also demonstrated a significantly greater odds of developing OM compared to 16% of patients with T1-T2 tumors who developed OM (OR = 2.28, 95% CI = 1.46-3.57, P = .0003, I2 = 0%, Figure 3B).1,17,24,25,27,31
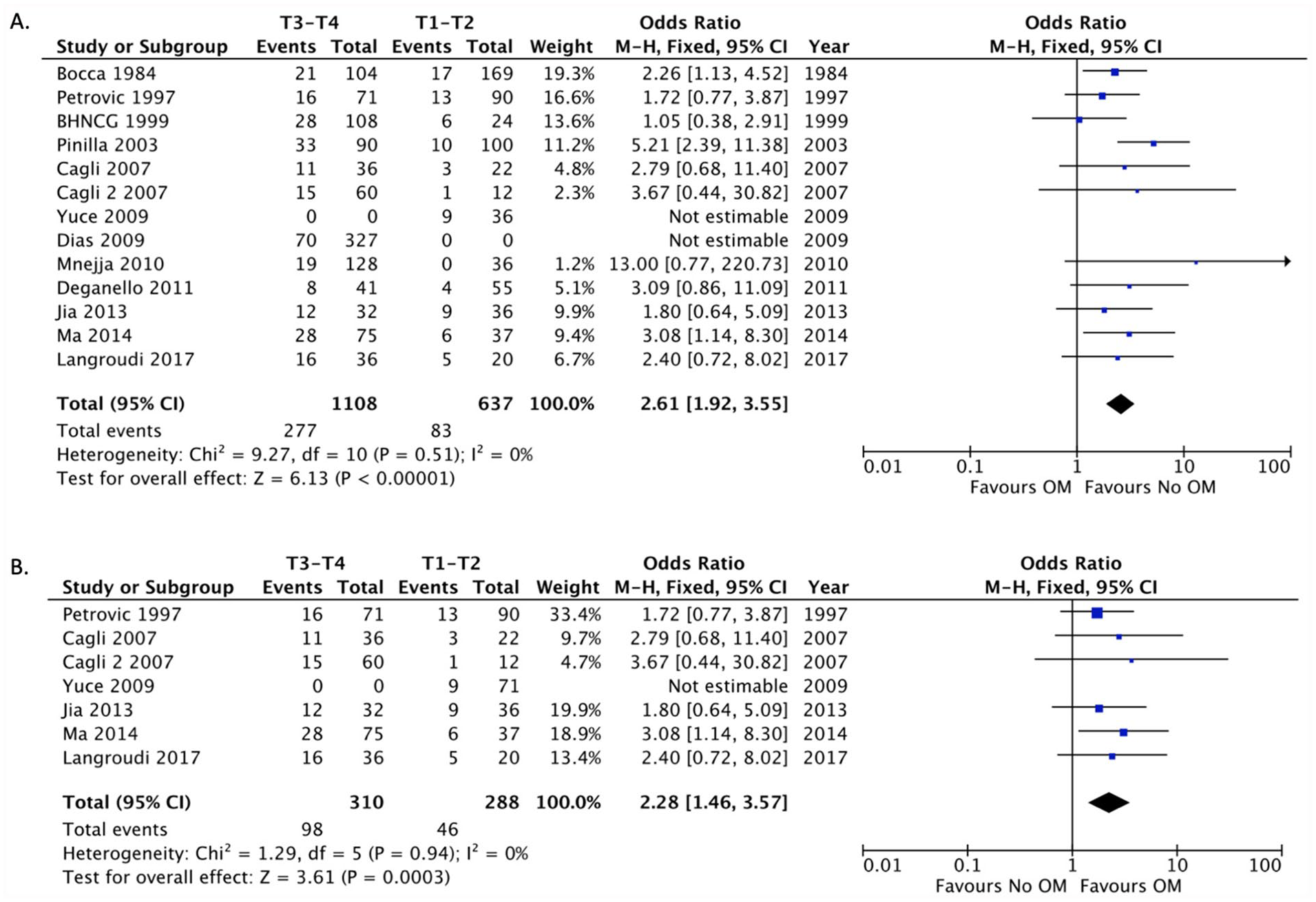
Forest plot of occult metastasis (OM) by T-stage (A) Across subsites and (B) In supraglottic tumors.
Patients with G2-G3 tumors from three included studies demonstrated significantly greater odds of developing OM compared to patients with G1 tumors (OR = 2.25, 95% CI = 1.18-4.27, P = .01, I2 = 63%, Figure 4A).1,12,26 In two studies, patients with extralaryngeal spread (ELS) demonstrated no significant difference in odds of developing OM compared to patients without ELS (OR = 1.49, 95% CI = 0.77-2.89, P = .24, I2 = 44%, Figure 4B).12,16 Meanwhile, tumors with cartilage invasion were significantly more likely to develop OM compared to tumors without OM (OR = 5.91, 95% CI = 1.67-20.89, P = .006, I2 = 83%, Figure 4C).12,16,26
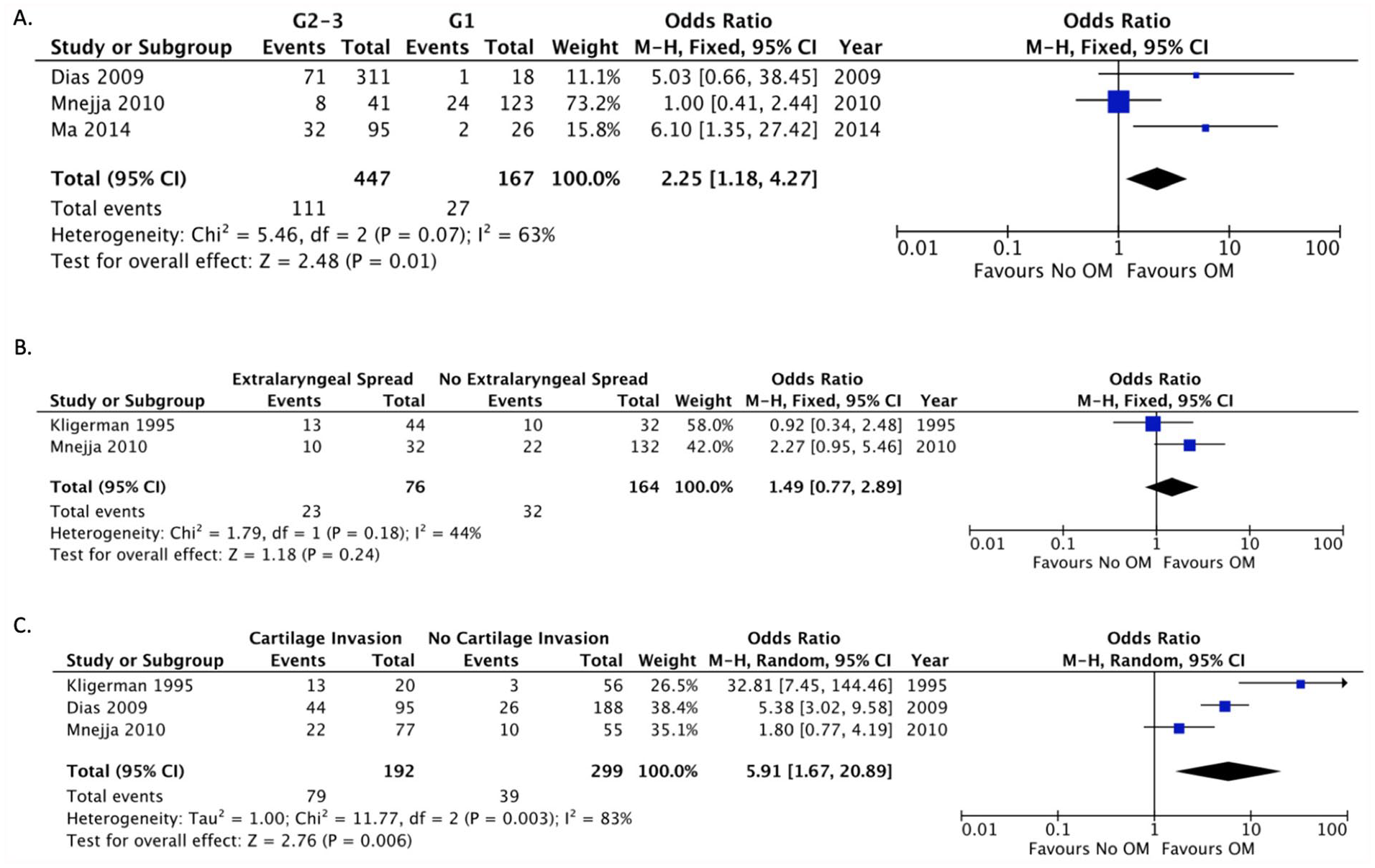
Forest plot of occult metastasis (OM) by (A) Tumor grade, (B) Extralaryngeal spread, and (C) Cartilage invasion.
Across 12 studies, patients with OM were found to have a significantly greater odds of developing regional failure compared to those without OM (OR = 1.46, 95% CI = 1.00-2.11, P = .05, I2 = 36%, Suppl. Figure 1A).1,9,11,12,18,20,22,24-26,28,29 In four studies that reported extranodal extension (ENE), 26% of patients with OM had ENE. Patients with OM with ENE also had significantly greater odds of regional failure (OR = 6.69, 95% CI = 2.07-21.6, P = .002, I2 = 21%, Suppl. Figure 1B) compared to patients with OM without ENE.20,26,27,29 Additionally, in five studies reporting rates of distant recurrence, patients with a history of OM had a significantly greater odds of metachronous distant metastasis (OR = 5.65, 95% CI = 3.36-9.51, P < .00001, I2 = 45%, Suppl. Figure 1C) compared to patients without a history of OM.12,16,17,19,26
Publication Bias
Funnel plots evaluating publication bias of the various studies included in the meta-analyses were generated. Overall, there appeared to be a moderate amount of asymmetry when evaluating odds of OM by T-stage across subsites (Suppl. Figure 2A) and less so in supraglottic tumors only (Suppl. Figure 2B). There was also moderate asymmetry in funnel plots for studies evaluating tumor grade, ELS, and cartilage invasion suggesting publication bias (Suppl. Figure 3A-3C). In the random effects funnel plot for risk of neck recurrence with OM, there appeared to be significant asymmetry (Suppl. Figure 4A), and there was asymmetry also found on the fixed effects plots for patients with OM with or without ENE (Suppl. Figure 4B) and for distant recurrence (Suppl. Figure 4C).
Discussion
Since the time of initial seminal studies describing patterns of nodal metastases, the role of END in laryngeal SCC has remained a topic of debate due to the potential for overtreatment, the morbidity of surgery, and heterogeneity of rates of OM by anatomic subsite.2,33-35,36 Historically, elective treatment of clinically node-negative necks is considered reasonable when primary tumor characteristics predict the likelihood of OM to be more than 15% to 20%. In this review, 20.4% of all patients with laryngeal SCC, 23.0% of patients with supraglottic SCC, and 12.2% of patients with glottic SCC who received END demonstrated OM. Rates of OM were found to be significantly higher in patients with more advanced T-stages across all subsites. The odds of developing OM increased from 13.0% in patients with T1-T2 tumors to 25.0% in patients with T3-T4 tumors (OR = 2.61, P < .00001). A subset of studies evaluated the rate of OM across T-stage in supraglottic tumors and this rate was also found to be increased in T3-T4 tumors compared to T1-T2 tumors (OR = 2.28, P = .0003). Taken together, our findings suggest that patients with T3-T4 tumors and should receive elective neck treatment despite having a clinically node-negative neck. Patients with supraglottic and transglottic tumors should be offered elective neck treatment across T-stages due to their increased odds of OM. While our analysis was not able to capture data specific to odds of OM and T-stage in purely glottic carcinomas, the overall rate of OM in glottic carcinoma and lower odds of OM in T1-T2 carcinomas across studies suggests that early stage glottic tumors can be observed.
Three of the included studies stratified rates of OM by cartilage invasion, and three also stratified rates of OM by tumor grade. In the presence of cartilage invasion, the rate of OM increased from 13.0% to 41.1% (P = .006). Advanced tumor grade was also found to significantly increase the rate of OM from 16.1% to 24.8% (P = .01). Our data are complementary to earlier literature by Ozdek et al, which determined tumor grade, lymphovascular invasion, and invasive tumor margins to be predictive of neck metastases in supraglottic SCC. 37 Unfortunately, the impact of other clinicopathologic tumor features such as perineural or lymphovascular invasion and margin status were unable to be evaluated as predictors in our study. However, in the included study by Dias et al, the rate of OM in patients with perineural invasion (PNI) was 32.4%, while the rate of OM in patients without PNI was 20.1%, but this difference was not statistically significant on our analysis (P = .10). 26
Subgroup analysis of recurrence outcomes suggested that OM significantly increased the odds of both regional and distant metastasis. Regional failure rates are also adversely affected by the presence of ENE with an increased rate of 20.0% versus 4.8% in the absence of ENE (P = .002). These findings are in keeping with historical data that demonstrate poorer regional and distant control for patients with OM and presence of ENE.35,38-43
While many centers have published useful outcomes data related to elective neck treatment in laryngeal SCC, there is a relative paucity of data directly comparing elective neck dissection to an observational protocol. In a 2009 systematic review of elective neck treatment of supraglottic SCC, Goudakos et al found there to be no overall, disease-specific, or neck disease-free survival benefit of elective neck dissection. 3 However, as the authors noted, there was significant clinical heterogeneity between the reported data of the included studies, thus preventing them from performing a formal meta-analysis. This is likely due to the heterogeneous population of cohorts included within each study, as most included node-positive patients in their analyses and inconsistently reported outcomes of interest.
Only two of the studies included in our analysis provided recurrence and survival data using an observational protocol.21,30 In the study by Sarno et al, 245 patients were subject to END, while 504 patients were observed with 83 (17%) receiving a subsequent therapeutic dissection due to clinically evident neck disease. They found no significant difference in both disease-free survival (DFS) or overall survival (OS) between the END or observational groups. Similarly, in the Djordevic et al study comparing 193 END patients to 51 observational patients, there was no significant difference in 5-year OS found between the two arms. Given the significant size discrepancy between these two groups and unavailability of subsequent recurrence data in the therapeutic dissection arms of these studies, a meta-analysis was unable to be performed between them. Nevertheless, these studies’ findings generally agree and are in keeping with historical data which have shown that END in head and neck SCC confers no overall survival benefit despite offering potentially improved regional control.2,35,38,40 Both of these studies are strengthened by their adequate control for laryngeal subsite and T-stage, but unfortunately, neither of the studies controlled for margin status or ENE. Only the Sarno et al study, reported impact of END on disease-free (DFS) survival. Not unexpectedly, however, Sarno et al found no significant difference in 5-year DFS between END and observation groups.
Our study carries some major shortcomings that must be reviewed. First, our study only reviews nodal metastasis to the nodal basins of neck levels I-V and completely excludes rates of occult metastasis to level VI. Unfortunately, none of the included studies reported this data point, likely for a few reasons. The retrospective cohort studies that report occult disease in this nodal basin include other head and neck primary subsites or clinically node positive patients in their data, thereby causing them to meet our exclusion criteria. As noted in a 2011 review of these studies by Medina et al, the published rate of occult metastasis to level VI ranges from 4.7% to 67%, with the highest rate reported in primary tumors occurring in the subglottis. 44 The vast majority of studies included in our analysis do not specifically evaluate occult metastasis from the subglottis due to its relative rarity compared to the glottic and supraglottic subsites. Despite these factors, it is unusual that none of the included studies reported data on occult nodal metastases to level VI. It is worth noting that patients who undergo en bloc total or open partial laryngectomy have a significant portion of level VI included as a part of the primary specimen. This may inject significant heterogeneity into the frequency and quality of formal pathologic reporting of level VI nodal dissection specimens.
Additionally, several of the studies included were either published in or included patients from the 1970’s and 1980’s.8,9,16,17,19,20,22,26 Some of these studies utilize only physical examination methods for clinical nodal staging, while some published more recently include CT, presumably in more recently staged patients. Given the greater sensitivity of radiologic imaging for evaluating nodal metastasis and the possibility that many patients included from the 1970’s and 1980’s would be staged as clinically node positive, we felt it pertinent to analyze our data after exclusion of these older studies. 45 Notably, the rates of overall OM and supraglottic tumors with OM were virtually unchanged. Though the rate of OM in glottic tumors was no longer able to be synthesized from multiple studies, this number from the Deganello et al study (13.2%) also remained consistent with the original analysis. 28 The percentage of T3-T4 and T1-T2 tumors with OM and odds of OM in advanced stage tumors compared to early stage tumors also remained consistent. Interestingly, through earlier study exclusion, there was found to be a much more robust impact of OM on regional failure (OR = 3.36, 95% CI = 1.66-6.82, P = .0008). This is likely due to exclusion of some earlier, larger cohorts and inclusion of more homogeneous cohorts investigating mostly supraglottic carcinomas. Given these findings, it is reasonable to conclude the validity of our overall analysis of the existing literature. Our data can ultimately provide both a historical and modern perspective on occult metastasis in laryngeal squamous cell carcinoma.
In addition to its potential therapeutic benefit, END may serve as a potential oncologic staging procedure for post-operative radiotherapy, particularly in clinically negative advanced stage primary tumors. For patients who are pathologically upstaged by documentation of occult metastases in their neck dissection specimens, this can help guide aggressiveness of adjuvant therapy and post-treatment surveillance. However, END does add significant morbidity to the surgical treatment of laryngeal SCC. Specifically, it has been demonstrated as a risk factor for development of post-operative pharyngocutaneous fistula.46-48
In the era of organ preservation therapy, the morbidity of surgery is usually too high to strongly consider it for primary therapy in many patients. Even for patients who are good surgical candidates, some consideration can be given to simply proceeding with organ sparing therapy if the need for post-operative radiation is strongly anticipated. While our data do not specifically evaluate the role of elective neck irradiation, the characteristics and patterns of occult disease reported in our analysis may be extrapolated for use in elective neck radiation therapy. Nevertheless, some laryngeal SCC patients are poor candidates for organ-sparing therapy due to a variety of potential biopsychosocial factors, and some patients may prefer to proceed with surgery as their primary modality of therapy. Elective neck treatment in these patients must have a clear indication with thorough explanation of the risks of surgery and added morbidity of neck dissection.
The overall quality of a systematic review and meta-analysis relies on the quality of the studies being analyzed. In this report, pooling of patient outcomes was limited by the heterogeneity of the data reported in the individual studies. In addition, the majority of the included studies are low-quality retrospective and observational, and, therefore lack the ability to control for specific confounders that were not measured and also introduce biases, such as selection bias and information bias. 49 In comparing the reported outcomes of a clinical trial versus an observational cohort study, a clinical trial can include any predefined endpoint, whereas the observational study is restricted by standard clinical care, which is not always comparable to standard endpoint assessment in clinical trials, such as OS or DFS. Observational studies can be more helpful moving research forward if they restrict focus to appropriate and valid endpoints. 50 Looking ahead, more high-quality, appropriately controlled prospective clinical trials are needed to replicate these results with a goal of achieving greater homogeneity in the reported outcomes.
Conclusion
Elective neck dissection is recommended for patients with advanced T-stage laryngeal SCC to help with achieving regional control. Patients with supraglottic and transglottic carcinomas are particularly at risk for developing OM. Tumors with OM carry increased odds of regional failure, particularly if ENE is present, as well as distant metastasis.
Supplemental Material
Annals_Sup_Fig_1 – Supplemental material for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis
Supplemental material, Annals_Sup_Fig_1 for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis by Daniel D. Sharbel, Mary Abkemeier, Michael W. Groves, William G. Albergotti, J. Kenneth Byrd and Camilo Reyes-Gelves in Annals of Otology, Rhinology & Laryngology
Supplemental Material
Annals_Sup_Fig_2 – Supplemental material for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis
Supplemental material, Annals_Sup_Fig_2 for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis by Daniel D. Sharbel, Mary Abkemeier, Michael W. Groves, William G. Albergotti, J. Kenneth Byrd and Camilo Reyes-Gelves in Annals of Otology, Rhinology & Laryngology
Supplemental Material
Annals_Sup_Fig_3 – Supplemental material for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis
Supplemental material, Annals_Sup_Fig_3 for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis by Daniel D. Sharbel, Mary Abkemeier, Michael W. Groves, William G. Albergotti, J. Kenneth Byrd and Camilo Reyes-Gelves in Annals of Otology, Rhinology & Laryngology
Supplemental Material
Annals_Sup_Fig_4 – Supplemental material for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis
Supplemental material, Annals_Sup_Fig_4 for Occult Metastasis in Laryngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis by Daniel D. Sharbel, Mary Abkemeier, Michael W. Groves, William G. Albergotti, J. Kenneth Byrd and Camilo Reyes-Gelves in Annals of Otology, Rhinology & Laryngology
Footnotes
Authors’ Note
This study was presented as a poster at the 2019 American Academy of Otolaryngology-Head and Neck Surgery Foundation Annual Meeting & OTO Experience in New Orleans, LA held on September 15-18, 2019
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.