
Abstract
Objectives:
This study was designed to assess the correlation between the grades of endolymphatic hydrops and the blood-labyrinth barrier permeability in the affected ear in Meniere’s disease, following the administration of intravenous gadolinium contrast.
Study Design:
Prospective study.
Methods:
The quantitative values of endolymphatic hydrops were determined after intravenous injection of a double-dose of gadobutrol in 39 patients with unilateral definite Meniere’s disease. Additionally, the signal intensity ratio of bilateral cochlear basal turns was evaluated and analyzed; The correlation between the grades of the endolymphatic hydrops and the signal intensity ratio of the cochlear basal turns in the affected ear was examined.
Results:
The grades of the endolymphatic hydrops can be quantitatively evaluated using magnetic resonance imaging (MRI). The signal intensity ratio of the cochlear basal turns in the affected ear was significantly higher than in the unaffected ear (P = .001); there was a positive correlation between the signal intensity ratio of the cochlear basal turn and the grades of cochlear (r = 0.634, P = 0.000) and vestibular(r = 0.559, P = .000) hydrops in the affected ear.
Conclusions:
The increased permeability of the blood-labyrinth barrier may play a role in the process of endolymphatic hydrops in Meniere’s disease.
Introduction
Meniere’s disease affects the inner ear, and presents with various recurrent symptoms, including tinnitus, fluctuating hearing loss and vertigo, 1 with endolymphatic hydrops as its pathological hallmark. 2 In recent years, there has been quite a few studies reporting the pathogenesis of endolymphatic hydrops in Meniere’s disease, however, the results have been considered somewhat controversial. Some researchers believed that the endolymphatic hydrops may be caused by changes in the electrophysiological environment of the inner ear, having been affected by excessive secretion or obstructed outflow, further influencing the signal transduction of vestibular and cochlear hair cells. 3 Other theories proposed that destruction of the blood-labyrinth barrier can lead to increased endolymphatic production, promoting endolymphatic hydrops. 4 In order to explore the relationship between the grades of endolymphatic hydrops and the blood-labyrinth barrier permeability, it may be helpful to elucidate the pathogenesis of Meniere’s disease.
Recently, extensive use of intravenous gadolinium contrast-enhanced MRI has been employed to depict the grades of the endolymphatic hydrops.5,6 Gadolinium agent enters the perilymph through the blood labyrinth barrier, rather than through the endolymph, resulting in a high signal intensity in the perilymph, but a low signal intensity in the endolymph. 7 Moreover, the contrast injection through the intravenous route may be an optimal approach to reveal the bilateral labyrinth simultaneously, due to its even distribution in virtually every compartment in the region of interest. This enables ascertaining bilateral blood-labyrinth barrier permeability. 8 Therefore, it is proposed that the ratio of signal intensity could provide a good estimator of the permeability of the barrier.
Recently, a semi-quantitative method has been utilized to assess endolymphatic hydrops by many researchers, and the grades of endolymphatic hydrops in the vestibule and cochlea were classified into 3 groups: none, mild, and significant9,10; Keller used a quantitative method to measure the grades of endolymphatic hydrops in the vestibule and cochlea. 11 In our study, we would like to assess the correlation between the degree of endolymphatic hydrops and the signal intensity ratio of the cochlear basal turn in the affected ear of Meniere’s disease, so as to explore the correlation between the grades of the endolymphatic hydrops and blood-labyrinth barrier permeability. Based on Keller’s method, we employed a new quantitative method to assess the degree of cochlear endolymphatic hydrops, which might make it easier to obtain a more accurate measure of endolymphatic hydrops. This method would indicate the degrees of endolymphatic hydrops more intuitively, and may assist in confirming our hypothesis.
Materials and Methods
Patients
Thirty-nine patients (17 males and 22 females), from March through December 2019, with unilateral definite Meniere’s disease, based on the diagnostic criteria of the Classification Committee of the Barany Society, 12 were included in our study. The cohort had an average age of 55 years (range, 10-77 years).
The study’s protocol was accepted by the medical ethics committee of our Hospital (2018-298-2), and all patients provided their informed consent.
Intravenous Gadobutrol (Gd) Injection and MRI
All patients underwent 3.0T MR imaging (GE Signa Pioneer 3.0T) using a 21-channel phased array receive-only coil. Regular scans consisted of T1 weighted images (TR 752 ms; TE 9.5 ms; 3 mm slice thickness; matrix 320 × 192; echo train length 3; acceleration factor 2; scanning time: 1 minute and 38 seconds) and T2 FLAIR sequence (TR 9000 ms; TE 95 ms; inversion time 2468 ms; 5 mm slice thickness; matrix 256 × 256; echo train length 22; acceleration factor 1; scanning time: 1 minute and 57 seconds).
A double-dose (0.2 mL/kg) of gadobutrol (Bayer pharmaceuticals, 7.5 ml/ unit, 1.0 mol/L) was injected intravenously; after 4 hours, a 3D-FLAIR sequence (TR 9000 ms; TE 163 ms; inversion time 2175 ms; 1 mm slice thickness; matrix 288 × 288; echo train length 180; acceleration factor 4; scanning time:12 minute and 4 second) was performed.
Imaging Analysis
Regular scans were used in order to rule out acoustic neuroma or other causes of vertigo and hearing loss. Four hours later, endolymphatic hydrops were observed on the 3D-FLAIR sequence, and endolymphatic hydrops were evaluated as following measuring method. The vestibular endolymphatic quantitative value was calculated by the ratio of the endolymphatic space inside the vestibulum to that of the cross-sectional area of the vestibulum, which was measured at the largest region of the utricle and saccule. The cochlear endolymphatic quantitative value was represented by the ratio of the transverse diameter of the cochlear duct to the sum of the perilymph (the sum of scala vestibule and scala tympani) of the second turn of the cochlea and the transverse diameters of the cochlear duct, which was evaluated at the optimal position of the cochlear basal 5 (Figure 1A).
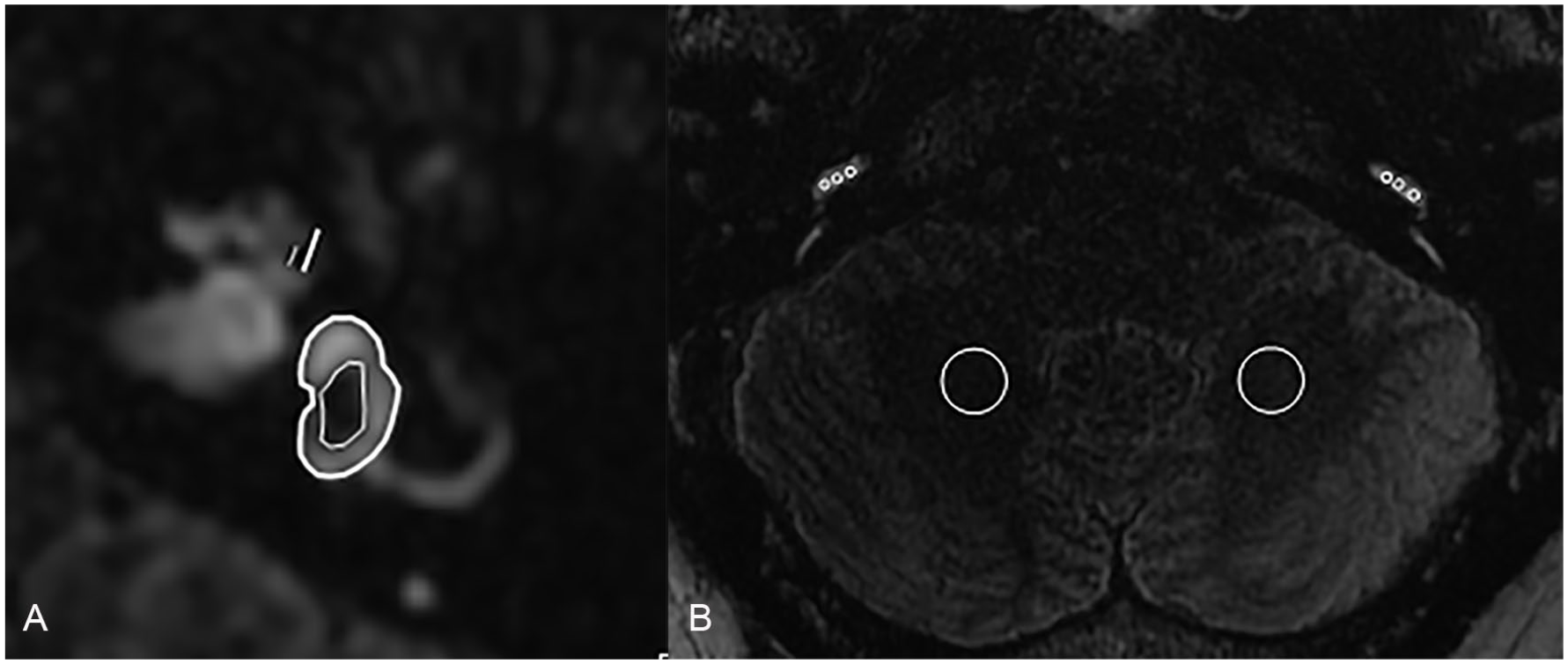
(A) Thin line: the transverse diameter of the cochlear duct; thick line: the sum of the perilymph (the sum of scala vestibule and scala tympani) of the second turn of the cochlea and the transverse diameters of the cochlear duct; thin circle: the endolymphatic space inside the vestibulum; thick circle: the cross-sectional area of the vestibulum. (B) A patient with left Meniere’s disease, a 3D-FLAIR image at the optimal position of the bilateral cochlear basal turns,3 1-mm2 regions of interest on perilymph of both cochlear basal turns and a coplanar circular 50-mm2 regions of interest of the cerebellum.
After a double-dose of gadobutrol was injected intravenously, the perilymph displayed a high signal while the endolymph showed a low signal. According to Shi’s method 13 mentioned above, at the optimal position of the bilateral cochlear basal turns, we randomly selected three 1-mm2 regions of interest on perilymph of both cochlear basal turns and a coplanar circular 50-mm2 regions of interest of the cerebellum on 3D FLAIR images (Figure 1B), and the signal intensity ratio of the cochlear perilymph to cerebellum was then calculated. In order to reduce the measurement error of signal intensity, we selected 3 regions of interest on each cochlear basal turn and utilized the average for our analysis. The signal intensity ratio for each patient was assessed by 2 experienced radiologists using the double blind method, and the mean value was calculated.
Statistical Analysis
The data were analyzed with the SPSS 20.0 software (IBM Corp., Armonk, NY), and data were presented as the mean ± SD.
A paired t-test was used to establish the differences in the signal intensity ratio between the affected and unaffected sides. Additionally, the relationship between the grades of endolymphatic hydrops and the signal intensity ratio of the cochlear basal turn in the affected ear was analyzed by the partial correlation analysis (Control Variables: age and gender). P < .05 was considered significant.
Results
All patients in our study had no history of any organic abnormalities in either the inner ear or brain. Perilympha displayed high signal, while the endolympha showed a low signal, and the boundaries of the perilymph and endolymph were clearly visible. The endolymphatic hydrops in the affected ear were observed by enhanced MRI (Figure 2A-C). Detailed quantitative values of endolymphatic hydrops and signal intensity ratio are listed in Table 1. The signal intensity ratio and the quantitative values of endolymphatic hydrops are summarized in Table 2.
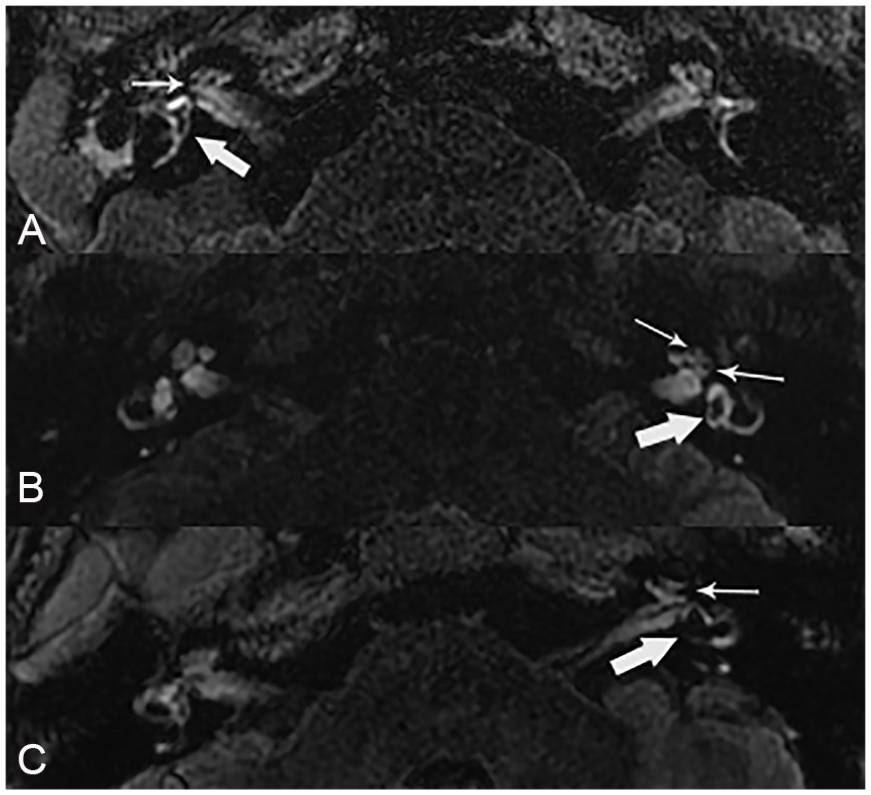
(A) A patient with endolymphatic hydrops in the right ear (cochlear hydrops: thin arrow; vestibular hydrops: thick arrow), the quantitative value of cochlear hydrops is 0.353 and the quantitative value of vestibular hydrops is 0.322, respectively. (B) A patient with endolymphatic hydrops in the left ear (cochlear hydrops: thin arrow; vestibular hydrops: thick arrow), the quantitative value of cochlear hydrops is 0.412 and the quantitative value of vestibular hydrops is 0.355, respectively. (C) A patient with the endolymphatic hydrops in the left ear (cochlear hydrops: thin arrow; vestibular hydrops: thick arrow), the quantitative value of cochlear hydrops is 0.5 and the quantitative value of vestibular hydrops is 0.62, respectively.
Detailed Quantitative Values of Endolymphatic Hydrops and Signal Intensity Ratio.
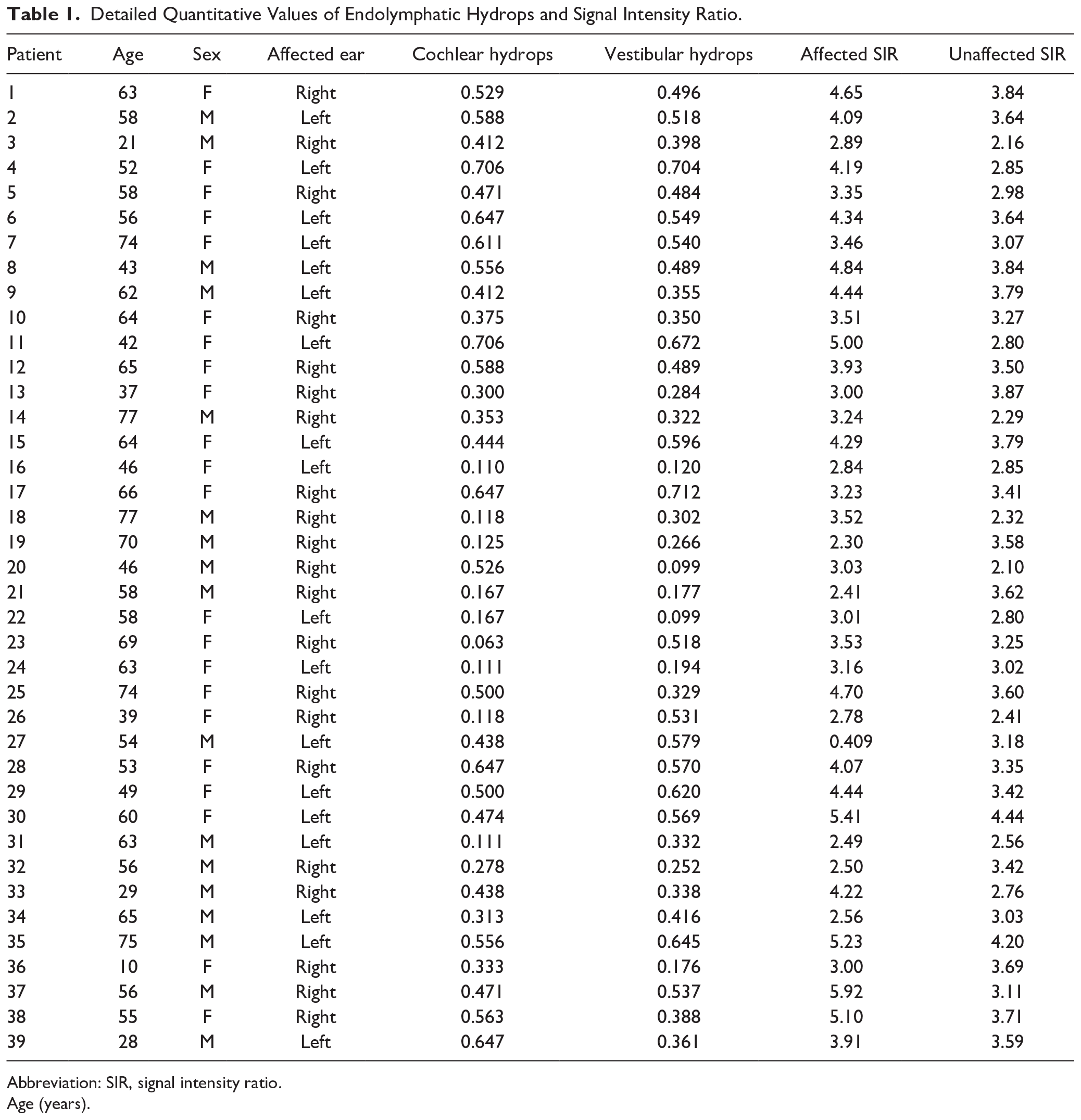
Abbreviation: SIR, signal intensity ratio.
Age (years).
The Results of Signal Intensity Ratio and the Quantitative Values of Endolymphatic Hydrops.

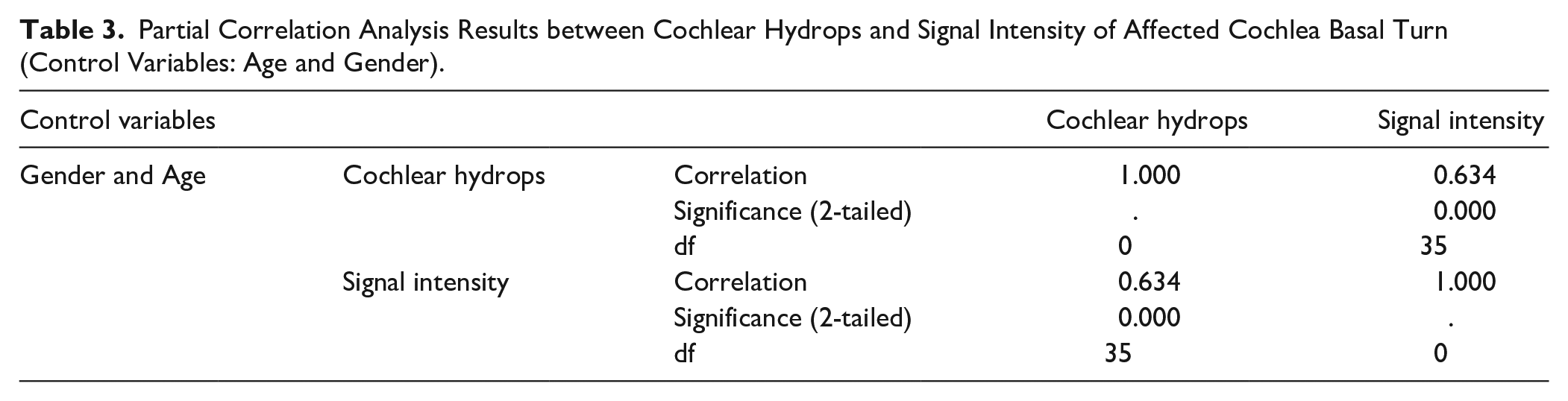
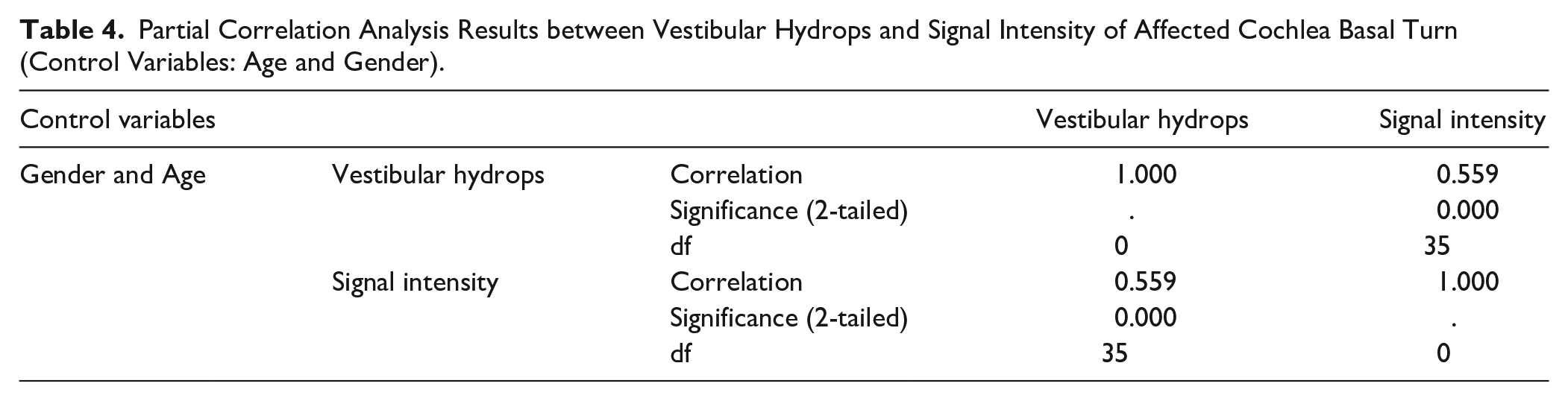
The signal intensity ratio of the cochlear basal turn in the affected ear(3.76±0.93) was significantly higher than that on the unaffected side (3.25 ± 0.56) (P = .001; Figures 3 and 4). By the partial correlation analysis, there was a positive correlation between the signal intensity ratio of the cochlear basal turn and the grades of hydrops in the affected ear, at both the cochlear level (Table 3) and the vestibular level (Table 4).
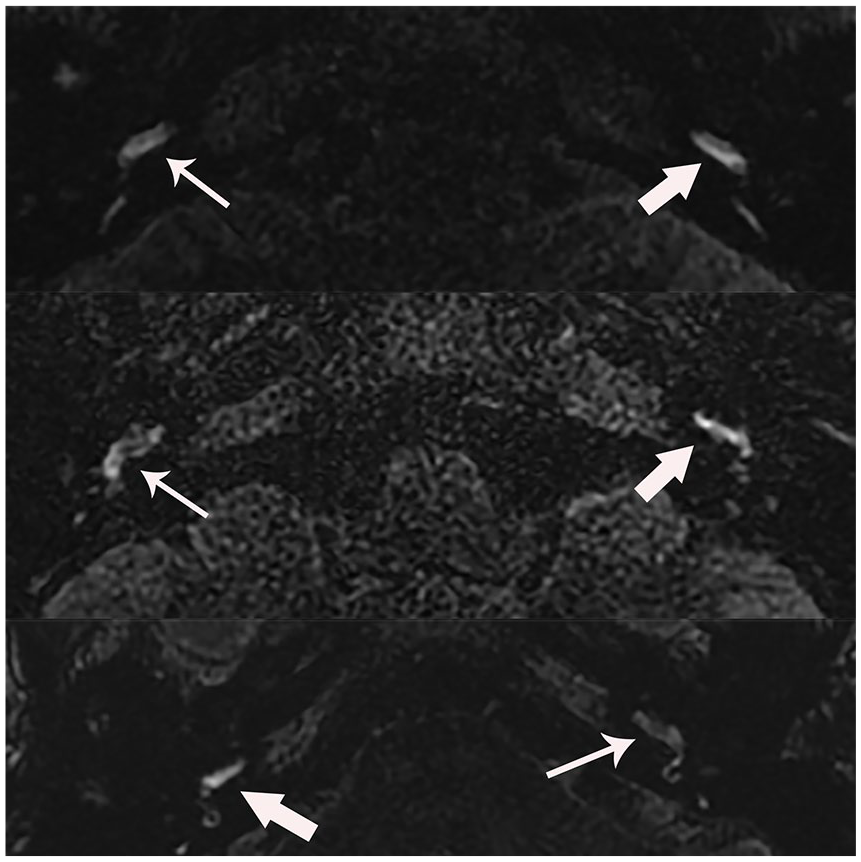
3D-FLAIR images collected at the optimal position of the bilateral cochlear basal turns in 3 patients with unilateral Meniere’s disease were shown. The signal intensity of the cochlear basal turn in the affected side (thin arrows) was significantly higher than that in the unaffected side (thick arrows).
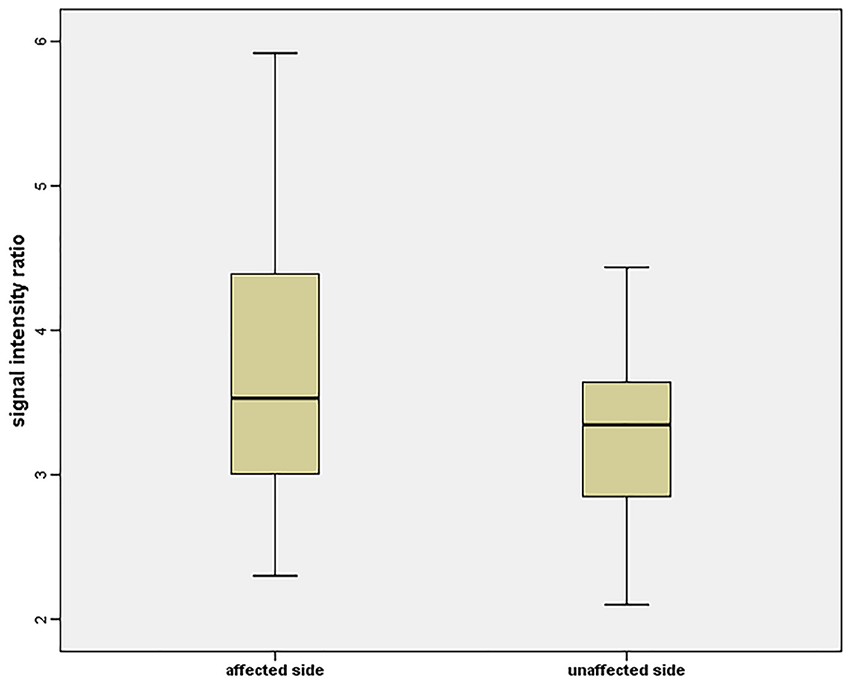
The signal intensity ratio in the affected side was significantly higher than that in the unaffected side of the cochlear basal turn (P = .001).
Partial Correlation Analysis Results between Cochlear Hydrops and Signal Intensity of Affected Cochlea Basal Turn (Control Variables: Age and Gender).
Partial Correlation Analysis Results between Vestibular Hydrops and Signal Intensity of Affected Cochlea Basal Turn (Control Variables: Age and Gender).
Discussion
Similar to the blood-brain barrier, the blood-labyrinth barrier allows for the penetration of low-molecular structures, including drugs, taurine, mannitol, steroid hormones and gadolinium contrast agents. 14 In animal models, the injection of lipopolysaccharide resulted in an increase in the permeability of the blood-labyrinth barrier, which can be measured by the enhancement of gadolinium in the perilymph. Moreover, some researchers have demonstrated that an increase in perilymph signal intensity on T2 FLAIR sequence is associated with an increase in the blood-labyrinth barrier permeability9,15; The signal intensity ratio is a good guage for assessing the damage to the blood-labyrinth barrier. 10 Following intravenous injection of gadolinium contrast agent, the contrast gadolinium agent enters the perilymph through the blood-labyrinth barrier; it cannot enter the endolymph, so that the perilymph presented with a high signal intensity at the cochlear basal turn after 4 hours, which could be detected more easily.8,16 Therefore, it is designated here as the measurement of signal intensity. In patients with Meniere’s disease, 16 the increased perilymph signal intensity of the cochlear basal turns has been confirmed to reflect the damage of the blood labyrinth barrier and the relative increase in permeability.
MRI is helpful for the detection of endolymphatic hydrops in Meniere’s disease. In this study, the various grades of cochlear or vestibular endolymphatic hydrops in the affected ear were found in all patients following the intravenous injection of gadobutrol; this is similar to findings reported in other studies.17,18 Our current results also showed that the signal intensity ratio of the cochlear basal turn in the affected ear was significantly higher than that of the unaffected ear, which was similar to previously reported studies,9,16 and animal studies of hydrops.19,20 The higher signal intensity ratio in the affected ear may reflect the increased permeability of the blood-labyrinth barrier.
Moreover, another interesting outcome was that the signal intensity ratio of the cochlear basal turn in the affected ear was significantly positively correlated with the grades of cochlear and vestibular hydrops, which was consistent with the results of Tagaya’s study. 9 The aggravation of the grades of endolymphatic hydrops with the signal intensity ratio of the cochlear basal turn increasing, indicated the increased blood labyrinth barrier permeability during the course of Meniere’s disease. Hence, we speculate that the increased permeability of the blood-labyrinth barrier may contribute to the formation of endolymphatic hydrops.
However, the breakdown of the blood-labyrinth barrier is likely to be an epiphenomenon and not specific to Meniere’s Disease. If an inner ear cannot maintain its endolymph/perilymph homeostasis, it is also unlikely to uphold an intact blood-labyrinth barrier. Some studies have demonstrated that the blood-labyrinth barrier permeability also increased in patients with sudden sensorineural hearing loss.21-23 Therefore, further studies are needed.
Limitation
The first limitation of this study was the absence of a control group of asymptomatic healthy patients. Systemic processes may affect the blood-labyrinth barrier permeability bilaterally 24 and may mask abnormalities in the symptomatic ear.
A second limitation was the lack of histological confirmation of the endolymphatic hydrops. It is virtually impossible to obtain histological evidence in living patients. Therefore, animal experiments would be necessary in order to validate the results of this study.
Conclusion
The increased permeability of the blood-labyrinth barrier may contribute to the process of endolymphatic hydrops in patients with Meniere’s disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.