
Abstract
Objective:
Septal Perforations may be asymptomatic or can cause significant problems including nasal obstruction, crusting, bleeding, whistling and in severe cases a change in nasal shape and even pain.
Method:
The author would like to present a single surgeon case series of septal perforation repairs, managed using an endo-nasal technique, with no external scars. There were 54 consecutive cases between 2011 and 2017. The repair was carried out using mucosal rotation flaps with an interposition graft of porcine collagen matrix. Patients were grouped according to the size of the perforation as measured at the time of the surgery. The patients were then clinically followed up for 1 year, and the recorded outcome measures were: the success of the surgical repair and the patient reported symptoms.
Results:
Surgical success was 70% up to 1 cm diameter, 77% from 1 to 2 cm and 82% in perforations from 2 to 3 cm in diameter. No perforation over 3 cm in diameter was successfully closed. Patients were rendered asymptomatic even if the perforation was not closed in between 81% and 91% of patients up to perforations 3 cm in size. Over 3 cm in size 50% of patients reported being asymptomatic.
Conclusions:
This technique is an effective and low morbidity option for patients with small to medium sized septal perforations. For perforations over 3 cm in diameter other options may be more suitable.
Introduction
Nasal septal perforations are a well-recognized problem that can occur for a variety of reasons. 1 Septal perforations can also be caused by trauma, including digital trauma or may be a manifestation of a systemic disease such as vasculitis. The commonest cause of a septal perforation is iatrogenic, as a result of nasal septal surgery one of the commonest of all ear-nose and throat operations. 1 The commonest cause in public perception is a perforation secondary to nasal drug use.
Although the nasal blood supply is excellent, damage to the septal muco-perichondrium leading to its permanent loss, rapidly leads to the necrosis of the septal cartilage beneath it. Unilateral septal mucosal injuries may well heal spontaneously, however, bilateral injuries need to be repaired to prevent the development of a septal perforation. The natural healing process leads to rapid re-epithelialization of the mucosal edges of the perforation and this process prevents the defect from healing over.2,3
The symptoms caused by septal perforations can also be varied. Some patients with a septal perforation may be entirely unaware that they have one, or they may be very symptomatic and troubled. The commonest symptoms described are nasal obstruction, crusting, bleeding and whistling. 4 The formation of crusting at the posterior edge of the septal perforation due to a low-grade perichondritis, can lead to bleeding when the crust comes away. Less commonly, patients may describe pain, or even report a change in nasal shape such as a “saddle nose”.
There is some discussion as to whether only symptomatic perforations should be repaired. Clearly, a quiescent asymptomatic perforation that does not change over time does not require surgical intervention. However, it is not clear if even an indolent process of crusting and removal, gradually wears the edges of the perforation, thus enlarging it over time.
Anterior septal perforations through the cartilaginous septum are much more frequently symptomatic than more posterior perforations through the bony septum, which tend not to be. 1 The symptoms may also relate to the size of the perforation, as smaller perforations are more likely to whistle, while large ones are more likely to cause functional symptoms. However, patients often complain of noisy nasal breathing even if the perforation does not actually whistle.
The management of septal perforations varies, as they have commonly been considered a difficult surgical challenge with a significant risk of failure if a surgical repair is attempted. The management has therefore traditionally been very varied. The commonest approach is conservative 5 with management based on nasal care with rinses and nasal lubricants to minimize bleeding and crusting. Septal buttons made of silicon and inserted into the perforation to obturate the perforation and ameliorate the symptoms have also been a method of management. 6 They are, however, poorly tolerated by patients and over time, may enlarge the perforation and can even cause complications such as fistulas through the hard palate, as seen by the author first hand.
Many different surgical methods have been described for the closure of septal perforations. Enlarging small perforations has been described as a method of stopping patients troubled by whistling or noisy breathing, 7 although this may ultimately reduce the chance of success of any subsequent attempt at surgical repair.
Surgical techniques described range from the use of free grafts 8 or local flaps and have variously been described9-13 via both open 14 and closed approaches to the septum, or via an endoscopic approach. 15 It has been documented that unilateral repairs are more likely to re-perforate than a technique using bilateral flaps in the nose. 16
The various methods have been described with and without interposition grafts. A variety of graft materials have been described, ranging from autologous grafts such as temporalis fascia, cartilage or bone,17,18 to extraneous materials including polydioxanone sheeting, 19 titanium membrane 20 or acellular dermal matrix.21,22 All have been shown to have varying success rates, with varying sizes of studies.
Some newer techniques avoid the use of mucosal flaps at all and involve obturating the perforation by under-laying one of the muco-perichondrial flaps with a graft to allow it to act as a bio-scaffold for re-epithelialization. The materials described are acellular dermis 23 or a polydioxanone sheet wrapped in temporalis fascia. 24 Again the results have been divergent in the studies.
The current accepted standard of care as practiced by the majority of surgeons treating this condition, are techniques involving an interposition graft with bilateral mucosal flaps to cover the implant.25,26 The exact designs of the flaps vary and the interposition grafts used include, PDS sheets, titanium, bone and cartilage or even more novel materials such as porcine intestinal mucosa have been used. 27
The technique described here involves the use of bilateral non-opposing rotation flaps 20 and a porcine collagen matrix (PermacolTM) that has been shown to provide a long-term tissue layer when used in the nose. 28 There has only been one other description of the use of PermacolTM in the repair of septal perforations. 29 The advantage of this method, is that there is no need for any autologous tissue harvesting and is therefore a cartilage sparing technique.
Materials and Methods
A series of 54 patients with septal perforations who underwent a surgical closure is presented. These patients were managed using a closed endo-nasal approach using local mucosal rotation flaps with a porcine collagen matrix (PermacolTM) underlay. PermacolTM comes in sheets with the consistency of soft leather. It is very tough and cannot be torn, but can easily be cut to the desired size and shape. The product is made from Porcine skin that has been treated so that all that is left is a pliable collagen matrix, that is highly versatile. The material is inexpensive and readily available, thus avoiding the need to harvest material from the patient and therefore avoiding a donor wound which could lead to donor wound morbidity and scar formation. The series is from a single surgeon and was collected prospectively and a 1-year post-operative follow up was attempted in all cases. The cases were grouped by the maximum diameter of the septal perforation as measured at the time of surgery. The perforation was measured carefully using a small measuring strip and the size of the perforation recorded was the largest dimension of the perforation. Often perforations were oval and in these situations the greatest dimension was used. The primary outcome measure was an intact nasal septum 1 year post-operatively. A secondary outcome that was recorded was any change in patient reported symptoms after the procedure. All patients were screened for signs of autoimmune disease and underwent blood tests to exclude a vasculitis or autoimmune condition.
Active intranasal drug use was an exclusion criteria for septal perforation repair. 30 Patients were followed up and managed conservatively until they had successfully managed to withdraw from drug use for a minimum of 1 year. If patients had stopped using cocaine, there was nothing in this data to suggest that having a perforation caused by drug use lead to a lower success rate of surgery.
Smokers were encouraged to stop smoking prior to surgery to optimize the success rate. 31 Delayed healing was observed in patients who smoked, although there was insufficient evidence to show that smokers had a higher failure rate of septal perforation repair overall.
Surgical Technique
The surgical technique used in this series is a closed endo-nasal technique raising the muco-perichondrial flaps on both sides of the nasal septum. The superior flap was based upon the anterior ethmoid artery for its blood supply. The inferior flap was fed posteriorly from the lateral nasal wall and the nasal floor and was therefore based on the inferior and septal branches of the spheno-palatine artery. 32 The flaps are designed asymmetrically to avoid opposing suture lines. The surgery was carried out under general anesthetic and usually as a day case procedure. The nose was prepared with a modified Moffats solution topically containing Cocaine Solution, Adrenaline and Normal Saline. The nasal lining was then injected with 2% lignocaine containing adrenaline 1:200 000.
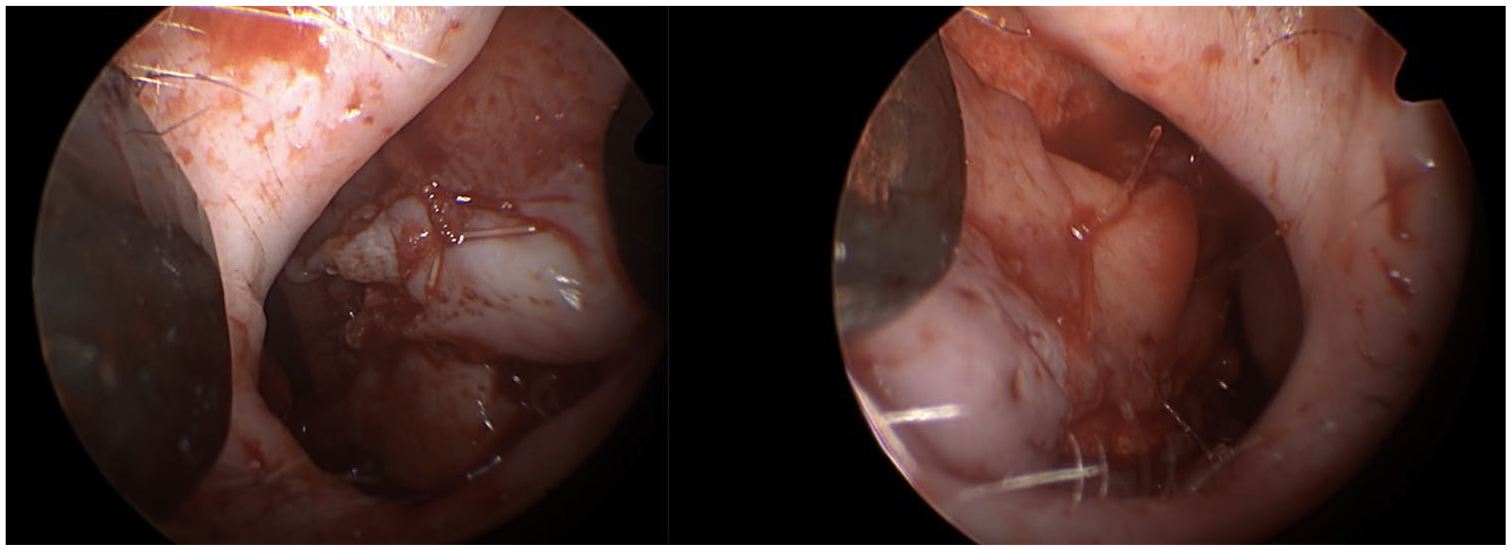
An incision was placed in the nasal vestibule and a standard endo-nasal septoplasty approach was used to lift both nasoseptal flaps. The cartilaginous septal perforation was dissected free by raising the muco-perichondrial flaps on both sides (Figure 1). A superior muco-perichondrial flap was then fashioned by making a releasing incision high up on the septum on this side. This allowed the flap to be mobilized and rotated downwards to cover the perforation on one side (Figure 2). Once the flap had been dissected, the perforation was sutured closed, by approximating the mucosal edges of the perforation and securing them with an absorbable monofilament mattress suture (Figure 2). An inferior mucosal flap on the other side of the septum was then dissected by freeing up the inferior part of the septum below the perforation. The dissection extended laterally along the floor of the nose and up the lateral nasal wall up to the attachment of the inferior turbinate. A releasing incision was then made under the inferior turbinate on the lateral nasal wall to allow the inferior flap to be mobilized medially to cover the septal perforation (Figure 3). The flap frequently needed to be released anteriorly from the skin of the nasal vestibule to allow the flap to be fully rotated over the septal perforation. This flap was then rotated upwards to cover the septal perforation from below. The bare septal cartilage left by fashioning the superior flap and the bare bone of the nasal floor left by the inferiorly based flap were left to re-epithelialize by secondary intention.
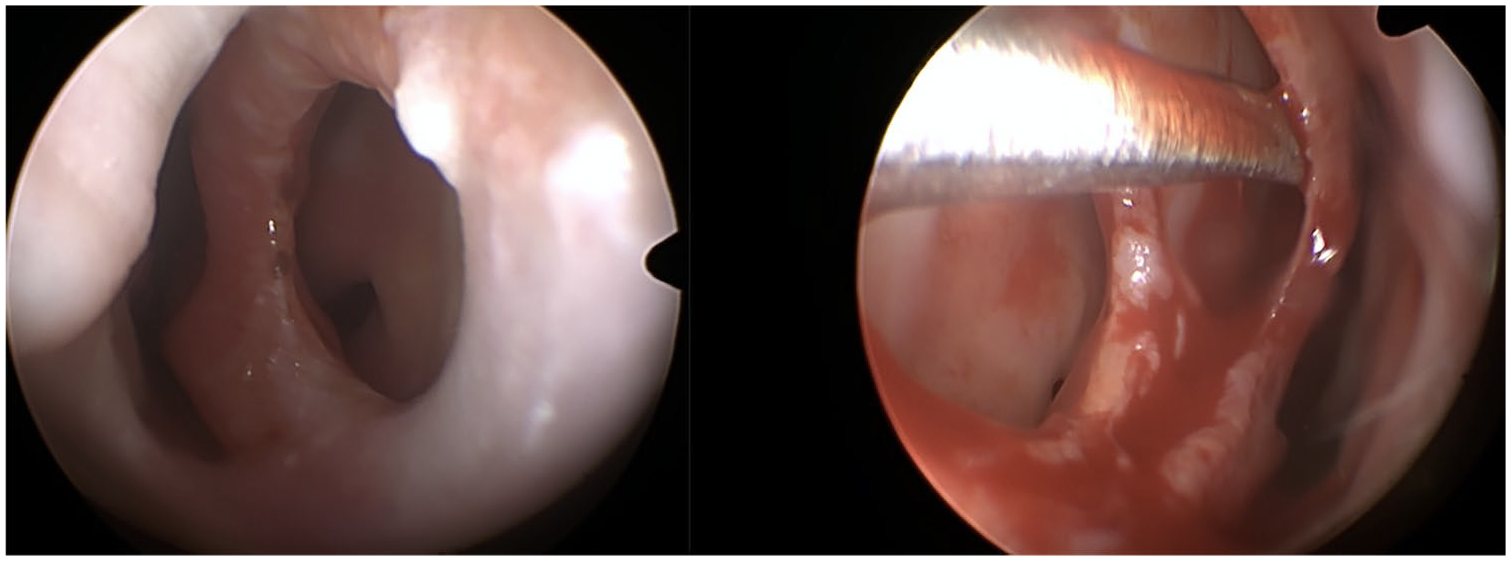
Showing septal perforation and raising muco-perichondrial flaps.
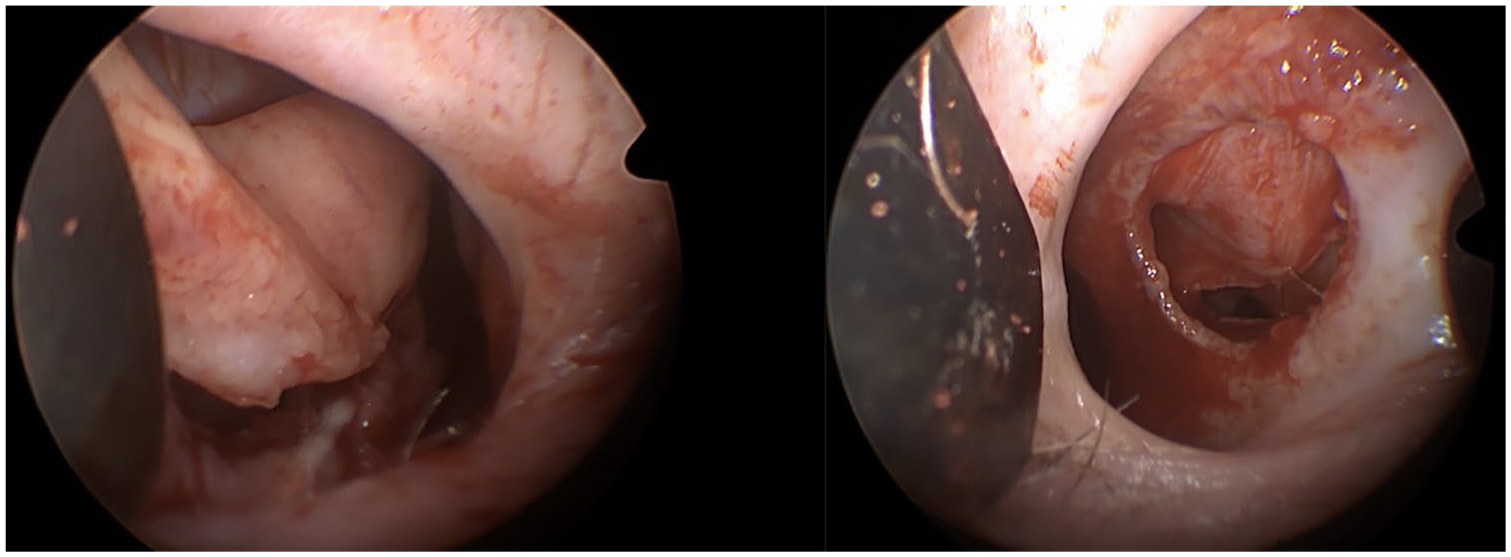
Showing release of the superior flap (left sided) and seen again with tacking suture in place holding the flap over the septal perforation seen from the contralateral side.

Inferiorly based flap pulled up over perforation on right side of septum. Showing Permacol interposition graft being positioned in the nose.
Once the mucosal flaps had been dissected, mobilized and prepared in this way, the porcine collagen matrix (PermacolTM) implant was prepared (Figure 3). The porcine collagen is available in different thicknesses and the author preferred the structural integrity of the 1 mm thickness collagen sheets, which did not unduly broaden the septum. The sheet of collagen was cut to generously overlap the edges of the cartilaginous perforation. If there was a slight deviation of the septum, then the porcine collagen implant was placed on the concave side, to minimize the chance of any subsequent nasal obstruction due to any increased bulk in the septum.
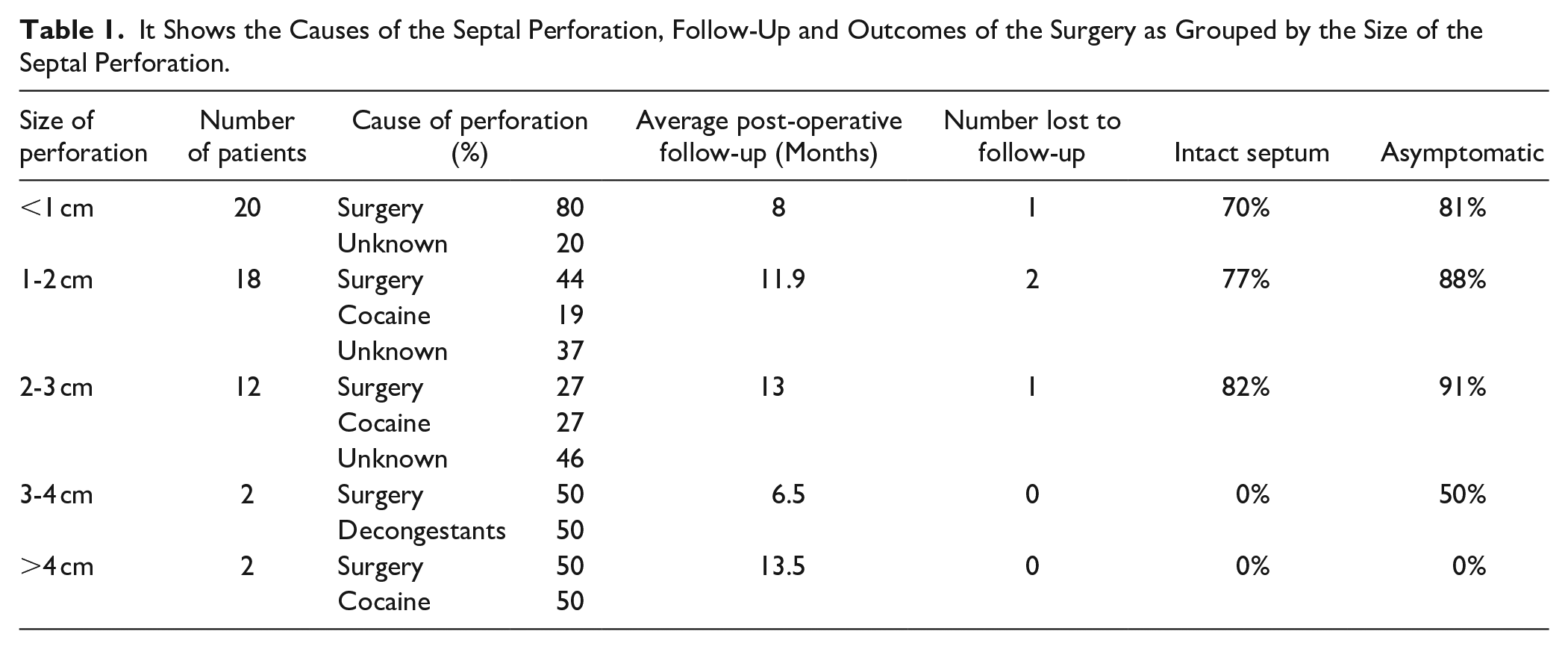
The porcine collagen was placed between the septal cartilage and the muco-perichondrial flap on one side. The implant and the rotation flaps were fixed in position with 5/0 polydioxanone mattress sutures. The incisions were closed with rapidly resorbing 5/0 monofilament sutures and the mucosal flaps secured in position with further mattress sutures (Figure 4). No splints, packing or dressings were placed in the nose.
Showing completed septal perforation repair with both muco-perichondrial flaps secured in place with absorbable mattress sutures.
Post-operative aftercare included analgesia, nasal douches and a week of oral antibiotics to minimize the risk of implant infection and therefore repair failure. Patients were then followed up at 6 to 8 weeks post-operatively and kept under review for 1 year.
Results
Overall 54 successive cases managed surgically between 2011 and 2017 are presented. The ages of the patients ranged from 14 to 63 years old. The results were grouped into 5 groups according to the maximum diameter of the septal perforation as measured at the time of surgery. The causes of the perforations were recorded according to each group. The smallest perforations were the ones most likely to have been caused by surgery (Table 1).
It Shows the Causes of the Septal Perforation, Follow-Up and Outcomes of the Surgery as Grouped by the Size of the Septal Perforation.
Three patients needed a revision procedure to achieve the result. One year post-operative Follow up was attempted in all cases, however, this was not achieved in all patients. Four patients were lost to follow up completely (Table 1).
All patients were treated with the above surgical technique. Three patients needed a revision procedure to achieve successful closure of the nasal septum. Asymptomatic, recurrent pinhole perforations were also recorded as a failure to close the septal perforation. Some of the patients without an intact septum were rendered asymptomatic and were therefore satisfied with their surgery. The smallest perforations were only closed in 70% of patients and no perforation over 3 cm in diameter was successfully closed. Perforations between 1 and 2 cm in diameter were successfully closed in 77% of cases and perforations between 2 and 3 cm were closed in 82% of cases. Rates of symptom relief were about 10% higher than the closure rate across the groups (Table 1).
Statistical analysis of the results using Fischer’s Exact Test did not show any significant difference in the outcome between the small and medium sized perforations. It did show a significant link between size and outcome when including perforations over 3 cm in diameter. The frequency of success in the different groups with confidence intervals was: <1 cm 70% (CI 43.5-87.4%), 1 to 2 cm 75% (CI 47.6-92.7%), 2 to 3 cm 81.8% (CI 48.2-97.7%) >3 cm 0% (CI 0-60%).
Due to the small numbers in each group, it was not possible to show a significant link between cause of perforation and outcome of repair. What was statistically highly significant was the difference in the cause of the perforations between the <1 cm perforation group and those with medium sized perforations. The high number of post-surgical perforations in this group was highly significant with a P-value of .0003.
In the 54 patients treated there were very few complications following the surgery. Infection was seen in 2 cases, which responded to a course of oral antibiotics. There was 1 case of post-operative hemorrhage, which required nasal packing to control. There was no adverse outcome in any of these cases.
Failure of repair was considered the main negative outcome of the surgery and is discussed separately. One patient developed a saddle nose post-operatively, which was subsequently corrected after the successful repair of a 3 cm septal perforation. The patient was very satisfied with the outcome. This was an unusual complication, and the cause of the saddle nose was due to the size and position of the perforation in a small female nose. The weakness in the remaining dorsal septal cartilage and some scar contraction following the repair, lead to the minor saddling of the nose that was subsequently corrected by surgical augmentation.
Nasal obstruction was usually a transient symptom post-operatively due to the bulk of the flaps narrowing the nasal airway. This usually settled within a few weeks of surgery as the healing process progressed and endo-nasal swelling settled down. Pain was rarely reported, and was perceived as similar to undergoing a septoplasty.
No patient reported a worsening of their symptoms or situation when compared to their pre-operative state. As such, this is a low risk and low morbidity intervention. There were also no cases of nasal stenosis or adhesions.
Revision surgery was carried out in 3 patients to achieve a successful outcome after an initially incomplete repair of the septal perforation. As the intervention was very acceptable to patients, this was an option patients were willing to undergo.
Discussion
This is one of the largest reported series of septal perforation repairs using this technique. The technique described is a closed approach with no external scars with a low rate of morbidity and complications. As the porcine collagen is a proprietary implant, there was no need for donor site incisions and as no autologous tissue was harvested or prepared, there was also a significant time saving.
The results suggest that this method appears to be particularly suitable for middle sized septal perforations between 1 and 3 cm where the success rate was highest.
What was of interest was the relatively lower success rate for the closure of small perforations, under 1 cm in diameter. There was no clear difference between these patients and the patients with larger septal perforations, other than the fact that most of the small perforations were caused by surgery. The <1 cm group had far and away the highest rate of post-operative septal perforations. This may suggest that perhaps there was a predisposing factor to the formation of the septal perforation. This may in turn suggest that attempting the surgical repair in patients with scarred tissue also may have predisposed to a higher failure rate. 32 This effect has previously been reported and previous septal surgery does correlate negatively with the success of septal perforation repair.
The described method is a relatively simple technique with a low morbidity and good success rate in medium sized perforations. Over 3 cm, other techniques may be more suitable. It is unclear why the failure rate for very small perforations was relatively high. Perhaps the relatively higher rate of post-surgical septal perforations in this group may offer an explanation. Although exactly how the post-surgical change leads to a higher tendency for the repair to fail, is unclear. 5
The dramatic drop in success rate in perforations over 3 cm may relate to the fact that a suitably wide mucosal flap is required to cover the perforation. If there is insufficient tissue above or below the perforation, then it becomes increasingly challenging to get the available tissue to cover the defect. Despite obturating the perforation with the porcine collagen implant, re-epithelialization alone does not seem to lead to a reliable closure. Sufficient mucosal cover appears to be important in achieving a successful closure. Therefore the height of the septal perforation is the true limiting factor in a repair using mucosal flaps.
Revision or staged surgery was used in the largest perforation, with the result, that a 4 cm perforation was reduced in size to only a pinhole perforation, after 2 procedures. The patient was asymptomatic although the septum was not fully closed. As the donor mucosa in the nose re-epithelializes after each intervention, these is always a new source of tissue to re-attempt the closure once the first procedure has been allowed to heal. The regenerated nasal mucosa is never quite as robust as the original nasal lining and the revision procedure can be a little more challenging in terms of achieving a good dissection and an intact muco-perichondrial flap to rotate into the defect.
A further limitation to this technique relates to the position of the septal perforation. If the perforation is very anterior, then the inferior flap can be difficult to mobilize forwards sufficiently to cover the most anterior extent of the perforation. The superior flap is much easier to move in an anterior direction, as it can be “bucket-handled” down once it has been released superiorly. The superior flap is generally far easier to dissect and is easier to move to cover the full extent of the septal perforation, regardless of the position of the defect.
The larger the septal defect, the harder it becomes to get a tension free closure within the mucosa of the nose. In order to close a perforation there needed to be a sufficient width of tissue between the edge of the perforation and the roof of the nose or attachment of the inferior turbinate. As these are the anatomical limits of dissection, a perforation that is larger than this distance, cannot be covered using these muco-perichondrial or muco-periosteal flaps.
Concurrent septoplasty or endoscopic sinus surgery was carried out in several cases, all of whome healed well and had a successful closure of their septal perforation. Carrying out other procedures with the septal perforation repair did not appear to compromise the success of the procedure.
The technique was very effective at ameliorating patient symptoms, even if the septum was not fully closed. This relates to the fact that the perforation was often moved and made significantly smaller, which has previously been shown to effectively improve symptoms. 33
Conclusion
The use of endo-nasal rotation flaps and interposition of porcine collagen matrix is a reliable method of septal perforation closure and yields comparable long term results to other published techniques. 34 As it is an entirely endo-nasal procedure with no external scars, acceptance from patients is high. Results are consistent, with the highest levels of success being achieved in septal perforations between 1 and 3 cm in diameter. Over 3 cm in diameter no perforation was successfully closed using this method, although patients reported that symptoms had improved and the numbers treated were only small.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.