
Abstract
Objectives:
Post airway reconstruction dysphonia (PARD) is common and has a significant effect on the quality of life of patients. Vocal fold injection augmentation (VFIA) is one treatment that can be used to improve glottic insufficiency in some patients. The goal of this study was to characterize the use and outcomes of VFIA for PARD.
Methods:
Retrospective chart review from January 2007 to July 2018 at a tertiary pediatric care center. Consecutive patients with PARD who underwent VFIA, who had a preoperative voice evaluation and a follow-up evaluation within 3 months after VFIA (fat, carboxymethylcellulose gel, hyaluronic acid).
Results:
Thirty-four patients (20 female) underwent VFIA. The mean age at the time of the injection was 13.6 years (SD 6.1). Twenty patients (58.8%) had a history of prematurity and a mean of 1.8 open airway surgeries. After injection, 29/34 patients (85.3%) noted a subjective voice improvement. The baseline Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V) overall severity score decreased by a mean of 5.7 (SD = 19.6) points, P = .12. Total pediatric Voice Handicap Index (pVHI) improved by 6.0 (SD = 19.5) points, from 57.4 (SD = 20.0) to 51.4 (SD = 17.2), P = .09. Functional pVHI subscore demonstrated a significant improvement, with a decrease of 3.4 (SD = 7.3) points, P = .02. All procedures were performed as an overnight observation and no complication occurred.
Conclusion:
Patients with PARD represent a complex subset of patients. VFIA is a straightforward intervention that may improve voice perception. Many patients reported subjective improvement despite minimal objective measurement. Further work is warranted to elucidate the role of injection in management of PARD
Keywords
Introduction
Post airway reconstruction dysphonia (PARD) is defined as any type of dysphonia created or aggravated by an airway surgery.1-7 Numerous surgical techniques have been described to improve airway patency, from a laryngotracheoplasty (LTP) with cartilage graft to a cricotracheal resection (CTR). Each of these procedures has its advantages and disadvantages regarding surgical correction of the stenotic airway. Similarly, these techniques, as well as the initial airway injury, impact the voice outcome to various degrees.2-7 Postsurgical causes of dysphonia include, but are not limited to, abnormal vocal fold mobility, persistent subglottic stenosis, posterior glottic diastasis, vertical asymmetry of vocal folds, vocal fold scaring, and supraglottic compression. Risk factors for poor voice outcomes after an airway reconstruction are numerous and include complete laryngofissure, cricotracheal resection, posterior grafting, higher grade of subglottic stenosis, revision surgery, and history of multiple past airway surgeries.4,5 On the opposite, patients with low-grade stenosis (grade 1-2), single stage procedure and fewer comorbidities are less likely to demonstrate PARD.6,8,9
When present, PARD is categorized as severe for half of these patients and has a significant effect on their quality of life (QOL). 9 Childhood dysphonia is associated with social withdrawal and depression, as well as having negative influence on emotional, educational, and occupational outcomes. 10 Moreover, it has been reported that teachers have a negative bias toward adolescents who have a voice disorder.7,10 Ultimately, voice disorders may lead to psychosocial problems that will affect patients over their lifetime, specifically their career choices and their long-term QOL. Once a patent airway has been secured, efforts should be made to improve patient’s voice and overall QOL as it can have significant effects on their well-being.
Patients with PARD represent a unique subset of patients. The majority of them have undergone numerous hospitalizations, are premature, and are typically involved in multiple complex medical and surgical interventions. When caring for pediatric airway patients, consideration of additional interventions should be individualized, which requires a thorough and complete workup. Voice evaluation provides further crucial, detailed functional information that can specifically direct the management of ongoing airway and voice problems.11-13
Given complex medical history, management of PARD should prioritize minimally invasive procedures both to protect airway improvements gained and to minimize comorbidity of voice surgical interventions. Vocal fold injection augmentation (VFIA) has proven to improve voice quality and reduced mean airflow rates in several group of patients.14,15 However, no data exist regarding patients with PARD. Recent evidence points to safety and efficacy in both the short and long term, though complications of extrusion and foreign body reaction have been reported.16,17 All these positive outcomes have been mostly studied for patients with isolated vocal fold paralysis, almost exclusively in an adult population.
Our institution provides voice evaluation through the Center for Pediatric Voice Disorders. This center has provided voice assessment and treatment for more than 14 years. Our team consists of otolaryngologists with training in laryngology, speech-language pathologists, and nurses. The whole team evaluates each new patient and a tailored treatment plan is established at the end of the visit. More than 200 new patients are seen annually.
The goal of this study is to characterize the use and outcomes of VFIA for PARD in a pediatric setting at Cincinnati Children’s Hospital Medical Center. We hypothesized that VFIA would improve voice quality in this specific and complex group of patients.
Methods
This study design was reviewed and approved by our institution review board (IRB) prior to collecting data (IRB #2017-1912). The records of all patients with a history of airway reconstruction seen at the Aerodigestive & Esophageal Disorder Center at a tertiary pediatric care center from January 2007 to July 2018 were retrospectively identified with our electronic medical record (EMR) database, which includes a list with all patients with prior airway surgery. A query was designed to pull all children who underwent airway reconstruction by filtering the EMR for the following CPT codes 31592, 31551-31554, 31580, 31584, 31587. We reviewed notes and included patients who underwent voice clinic evaluation and vocal fold injection under general anesthesia.
All patients from this cohort were also seen for initial voice evaluation at the Center for Pediatric Voice Disorders during the same period. Demographic data, operative notes, and endoscopic and stroboscopic evaluations were obtained. We also obtained the Pediatric Voice Handicap Index (pVHI), 17 the Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V), 18 aerodynamic and acoustic parameters at the time of the visit for voice evaluation. The pVHI is a survey reflecting a parent’s responses about their child’s voice quality on overall communication, development, education, social, and family life. The higher the score, the higher the negative impact on the child’s life is. The CAPE-V is a tool developed to promote a standardized approach to evaluating and documenting auditory-perceptual judgments of voice quality. CAPE-V reflect clinician’s direct observations of the patient’s performance during the evaluation and is not taking into account patient report or other sources. The higher the score is, the lower the voice quality is.
All patients then underwent VFIA procedures under general anesthesia combined with a microlaryngoscopy and bronchoscopy (MLB). VFIA included endoscopic injection of carboxymethylcellulose (Prolaryn™, Radiesse voice gel™), hyaluronic acid (Restylane™), or homologous fat both in a unilateral or bilateral fashion. The amount of material injected was based on clinician’s judgment to provide enough bulk to the vocal fold to allow complete closure during phonation. The product injected was based on both clinician’s judgment and product availability. All patients underwent another formal voice evaluation between 1 and 3 months after their surgery. Furthermore, patients were asked to rate their voice as “improved” or “not improved” as their subjective assessment during that encounter.
Endoscopic Examination and Voice Evaluation
Each patient underwent a transnasal flexible and/or transoral rigid examination. Selection of the flexible and/or rigid endoscope used was made by the team of pediatric otolaryngologists and speech-language pathologists who determined the most appropriate instrument given the size of the child and the technical needs of the examination. The standard voice evaluation includes several aspects of laryngeal function, including the source of phonation, glottic closure pattern, and determination of presence and pattern of a glottal gap. If there was adequate tracking of the acoustic signal, simulated slow motion stroboscopy was captured to identify the source of vibration (vocal folds or other structures) and any vibratory characteristics of the primary voice source. Source of phonation was defined as the localization of laryngeal closure during the closed phase of phonation, most commonly glottic or supraglottic. Glottic closure pattern refers to the extent of vocal fold closure during the closed phase of phonation, described as complete, incomplete, or inconsistent. Glottal gap was defined as any incomplete glottic closure. These evaluations were performed by both speech pathologist and otolaryngologist who agreed on their findings.
Statistical Analysis
Descriptive statistics were calculated on all variables, including means with standard deviations or medians with interquartile ranges for continuous variables or frequencies and percentages for categorical variables. Paired t-tests were used to examine differences in CAPE-V, pVHI scores, acoustic, and aerodynamic measures. McNemar’s test was used to examine change in vibration source among matched pairs. Measures from the initial voice evaluation were compared to measures post voice surgery. P values of <.05 were used to determine significance. Statistical analysis was performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Fifty-one patients (51) underwent VFIA for PARD with 34 patients (20 female) having pre- and post-surgical voice evaluation. The 17 patients without complete data had similar age, sex, comorbidities, number of past airway surgery; baseline pVHI and CAPE-V (P > .05). For the 34 patients with complete data, the mean age at the time of the injection was 13.6 years (SD = 6.1) (Table 1). Twenty patients (59%) had a history of prematurity. Patients had a mean of 1.8 open airway surgery, with 8/34 (24%) with more than 3 prior open airway surgeries. Twenty-six (26/34, 77%) had a history of tracheostomy. All patients were decannulated at the time of the VFIA. Time between airway surgery and voice concerns was 8.2 years (SD 5.4 years).
Demographic Data and Preoperative Laryngoscopy and Stroboscopy Findings for Patients with Vocal Fold Augmentation Following Airway Reconstruction.

A mean of 0.3 cc (SD 0.2) was injected in the vocal fold. There was no correlation between the amount of injected materials and the voice outcomes. After injection, 29/34 patients (85%) noted a subjective voice improvement. The 5 patients without improvement appeared to have different baseline characteristics compared to the rest of the patients, including age at injection (16.7 years, SD 6.1) and the number of past airway surgeries (2.8, SD 1.1), but was not statistically significant (P > .05). The baseline CAPE-V overall severity score decreased from 62.7 (SD = 21.9) to 56.9 (SD = 22.3), P = .12. The pVHI improved by 6.0 (SD = 19.5) points, from 57.4 (SD = 20.0) to 51.4 (SD = 17.2, P = .09). The functional pVHI subscore demonstrated the most improvement, with a decrease of 3.4 points (SD = 7.3), P = .02. All subscores are available in Table 2. All patients with more than 5 points of improvement on the pVHI scale only had one past open airway surgery. Material injected consisted of carboxymethylcellulose (62%), hyaluronic acid (35%), and homologous fat (3%). There was no significant difference in voice evaluation with the material injected. Aerodynamic parameters remained similar after injection (all P > .05) (Table 3). The source of phonation also stayed similar before and after injection (P = .6). All procedures were performed as an overnight observation and no complications were observed after injection.
Pre and Postsurgical CAPE-V and pVHI Scores for Patients Undergoing Vocal Fold Augmentation.

Abbreviation: SD, standard deviation.
Aerodynamic Parameters Before and After Vocal Folds Augmentation.
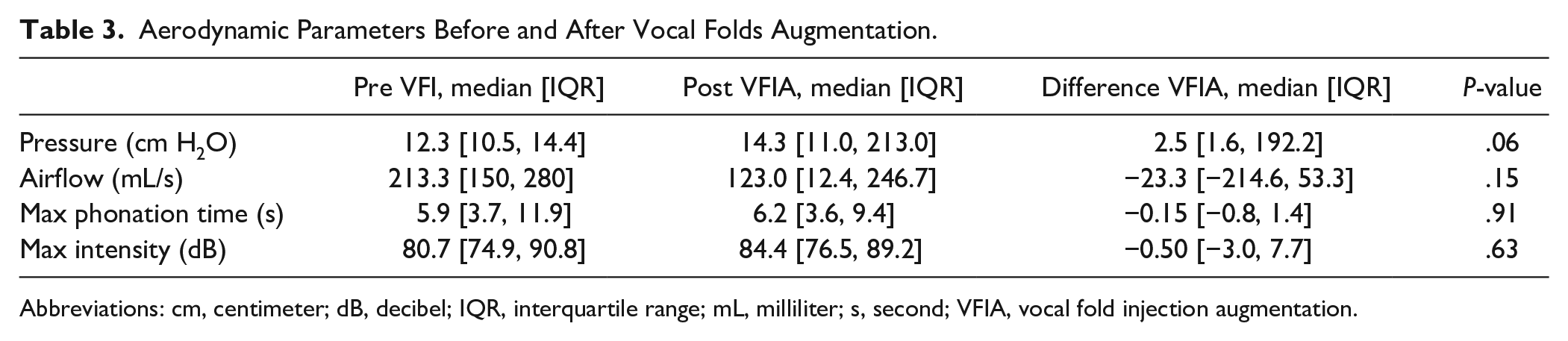
Abbreviations: cm, centimeter; dB, decibel; IQR, interquartile range; mL, milliliter; s, second; VFIA, vocal fold injection augmentation.
Discussion
This is the first paper to evaluate the impact for VFIA to improve voice in the setting of PARD. Many subjects reported subjective improvement despite minimal objective measurement in voice measures with the CAPE-V. Although the mean score was different for pVHI (57.4-51.4), the value was not statistically significant. However, there was a clinically and statistically significant improvement for the functional pVHI score. Most importantly, no complications occurred with the use of vocal fold injection in this complex population.
Most patients will report some degree of dysphonia after airway reconstruction. Typically, voice outcomes after airway reconstruction include roughness, breathiness, supraglottic phonation, or inappropriate pitch. These children often present when they are becoming more social or making decisions about future careers. Our study demonstrated that vocal fold injection is a fast and easy procedure and might improve the perception of their speech.
Five patients did not feel a subjective improvement of their voice after their treatments. Although the power to show a statistically significant difference, we found that these 5 patients were older than the rest of the group and had more past open airway surgeries. One of the reasons for the lack of subjective improvement might be the higher expectations before surgery for older teenagers. In adolescents, the voice is important for social interactions and they may fear of peer responses to their voice, as well as frustration and social isolation. Not nothing a tremendous change in their voice after injection may explain their results. It would be of utmost importance to discuss the possible improvement or non-improvement with patients before surgery, especially in this category of patients. Moreover, we noted that patients with more than 5 points of improvement on the pVHI scale only had one past open airway surgery. Having only one prelaryngeal muscle dissection during airway surgery compared to the rest of the patients may have an impact on the baseline voice contributing to a better improvement. Thus, patients with only one past airway surgery might have better outcomes. This might help preoperative counseling.
Objective perceptual dysphonia and perceived impacts of voice disorders as measured by CAPE-V and pVHI varied between subjects. This was not unexpected as, for this population, it has been demonstrated that the correlation between parent-reported pVHI scores and expert ratings using the CAPE-V is weak-to-fair at most. 19 The CAPE-V did not significantly improve for our patients. Despite improving glottic insufficiency, there are other factors contributing to persistent dysphonia, including vocal fold scarring, height mismatch, and alternative phonatory sources. Improving the glottis insufficiency by vocal fold injection may be a factor resulting in the observed improvement in the functional scale of the pVHI. This subset addresses questions such as “People have difficulty hearing my child in a noisy room” and “My child tends to avoid communicating because of his voice.” Parents state that it is easier for them to hear their child on the phone, or the child does not fatigue as much after surgery, all similar concepts of the functional subset.
However, the overall pVHI showed a notable but not significant differences pre–post surgery. One reason may be because parents and patients anticipated a more significant voice change. Although it is clearly discussed prior to surgery that voice change may not be substantial, families may expect a more substantial voice change; therefore, they do not report the small voice changes in the pVHI. Another reason might be the sample size that was not sufficient to pick up the difference, given the varied presentation, there is large variance in the sample thus needed a larger sample size to pick up a modest improvement.
An important factor is that no patients or parents noted their voices worsened with injection. Furthermore, no complications occurred with vocal fold injection for PARD. As already mentioned, this group of patients represents a unique challenge with their multiple comorbidities and their surgically-altered airway. The balance between airway and voice is often precarious. The intervention to improve PARD should be as less invasive as possible. Vocal fold injection appears to be an adequate initiate procedure when indicated for these patients.
In our cohort of patients, no product demonstrated better outcomes. Zeitels et al (2019), demonstrated that cross-linked hyaluronic acid (Restylane™) showed a superior injection localization, tissue compatibility and residence in time. 20 We could not appreciate objectively a difference in voice quality, possibility due to our relatively small samples of patients. Furthermore, all patients were evaluated within 3 months after injection, which is below the time of resorption of these products.
Patients reported concerns regarding their voice 8 years after their initial airway surgery, and at mean age of 13.6 years. Children with a history of airway surgery often present when they are becoming more social or they are making decisions about future career. As children reach middle school age, they may have more issues related to being in multiple different classroom settings with different peer groups and teachers who are not familiar with their voice. Concerns include peers reporting this dysphonia as well as having difficulty being heard in a noisy environment. In teenagers and adolescents, the voice is important for social interactions, defining their identity, and determining their future occupation. Dysphonia for such patients should not be overlooked as even minimal improvement might improve their QOL as it can have significant effects on their well-being.
This study is not without limitations. PARD represents a very specific and complex group of patients, with our results that cannot be generalized. We have a relatively small cohort of patients. A proportion of patients did not complete post procedure outcomes or did not follow up because of distance travelled. These patients may have had better voice outcomes and did not want a follow up because of they were satisfied with the results. However, our group of PARD still represents the largest cohort who underwent vocal fold injection. Our postoperative period is relatively short and does not extend further than 3 months. Lastly, patients referred to our Voice clinic and who subsequently underwent vocal fold augmentation likely represent a subset of patients with worse dysphonia. Outcomes may be better for patients with a less severe degree of PARD or a less complex airway history.
Conclusions
Patients with post-airway reconstruction dysphonia represent a complex subset of patients. Vocal fold injection augmentation is a straightforward intervention that may improve voice perception. Many subjects reported subjective improvement despite minimal objective measurement in voice measures. Further work is warranted to elucidate the role of injection in management of PARD.
Footnotes
Authors’ Note
This project was presented during the American Laryngological Association meeting in May 2019, Austin, TX.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.