
Abstract
Background:
Sinocutaneous fistulae (SCF) are abnormal communications between the paranasal sinuses and the overlying skin. They may be difficult to manage due to facial geometry, scar contraction, and poor tissue vascularity. We describe a novel use of the buccal flap and review the literature to examine management options for this disease process.
Methods:
A PubMed/MEDLINE literature search was performed for studies published between January 1, 1950 and April 29, 2020 that describe management strategies for SCF. The clinical record, imaging, and operative reports were reviewed of the case in which the buccal fat flap was used in reconstruction.
Results:
A total of 359 articles were retrieved. After removing duplicate articles, non-English studies, animal studies, duplicate articles and studies that mentioned SCF without specific mention of management strategies, 51 articles were reviewed. Management paradigms throughout the articles include (1) removal of infection, (2) ensuring patency of sinus outflow tracts, (3) tensionless multilayered closure using well vascularized tissue, and (4) prevention or minimization of future risk factors for fistula formation.
Conclusion:
This article informs surgeons on reconstructive options for sinocutaneous fistulae including a novel description of the buccal fat flap.
Introduction
Sinocutaneous fistulae (SCF) are abnormal communications between the skin and an underlying paranasal sinus. Management of these wounds is challenging secondary to complex anatomy, poor tissue healing, and compromised vascular supply. We describe a novel use of the buccal fat flap as a reconstructive option with a brief review of the literature.
Materials and Methods
A Medline literature search was performed for studies published between January 1, 1950 and April 29, 2020 that describe risk factors and management strategies for SCF. Search terms included “sinocutaneous fistula,” “sinoorbital fistula,” “orbitocutaneous fistula,” “nasocutaneous fistula,” “craniofacial resection fistula,” “sinonasal fistula,” and “buccal fat flap,” “paramedian forehead,” “pericranial,” “inferior turbinate,” “middle turbinate,” “nasoseptal, “temporalis,” and “free flap” which yielded a total of 359 articles. Eleven articles were duplicates and were removed. About 348 records were screened. Six non-English language articles were excluded. Five animal studies were excluded. And 286 articles were excluded that described oroantral fistula repair, orbital fracture repair without mention of fistula, airway management in the patient with SCF, branchial cleft deformities, congenital anomalies, oncologic outcomes of skull base tumors, degloving approaches for sinonasal tumors, and endoscopic dacryocystorhinostomy. In general, articles were excluded if they did not specifically describe the operative technique for sinocutaneous fistula closure. Following this, a total of 51 English-language articles were reviewed that specifically described reconstructive techniques for SCF in humans (Supplemental Material 1). Additionally, we reviewed the electronic medical record for 1 patient who had repair of a SCF via a pedicled buccal fat flap, which to our knowledge has not been previously reported.
Case Report
A 76-year-old female had a previous history of oral squamous cell carcinoma of the left tongue treated with surgery including a hemimandibulectomy and radiotherapy 16 years earlier. She presented with a left cheek mass that showed evidence of sinonasal undifferentiated carcinoma. She underwent neoadjuvant chemotherapy before undergoing a left total maxillectomy with reconstruction of the orbital floor with titanium mesh, placement of a Crawford tube to maintain nasolacrimal duct patency and obturation of the hard palate. Five years later the patient presented with left ectropion and lower eyelid and cheek erythema, edema, and discharge at the medial canthal region. She was admitted for IV ampicillin sulbactam and was determined to have a SCF 1.2 cm × 1.6 cm directly over the medial screw of the titanium mesh plate (Figure 1). She was ultimately discharged on oral amoxicillin/clavulanate. After resolution of the acute infection she continued to have a persistent SCF and was taken to the operating room for removal of hardware and closure of the fistula. The SCF was excised and the exposed hardware was removed with a final defect size of 3.5 cm × 2.0 cm (Figure 2). A Mustarde flap was created by incising medially along the nasal sidewall and into the melolabial fold. A superolateral subciliary incision was made and extended over the orbital rim and arching into the temple and preauricular region. The flap was elevated and include the entire midface and cheek in a subcutaneous plane (8 cm × 14 cm). An inferiorly based pedicled buccal fat flap was mobilized superiorly, placed into the defect, and secured with circumferentially using absorbable monofilament suture to create a water-tight inner layer (Figure 3a and b). This was also secured superiorly to the nasal bone using the JuggerKnot fixation system with 3-0 MaxBraid sutures (Zimmer Biomet, Warsaw, Indiana). Both medial and lateral canthopexies were then performed for ectropion repair. The zygomaticofacial flap was then advanced over the buccal fat and suspended superiorly to bone using the JuggerKnot fixation system with 3-0 MaxBraid sutures to provide support the lower eyelid. The incisions were then closed in a layered fashion with absorbable suture. The patient did well post-operatively and had a small area of crusting 2 months after surgery (Figure 3c). She continued to heal well and shows no signs of SCF recurrence 7 months after surgery (Figure 3d). The institutional review board deemed this case exempt from review as it is a single description of a technique and does not qualify as research defined as a systematic investigation of 3 or more cases that includes research development, testing, and evaluation, designed to contribute to generalizable knowledge.
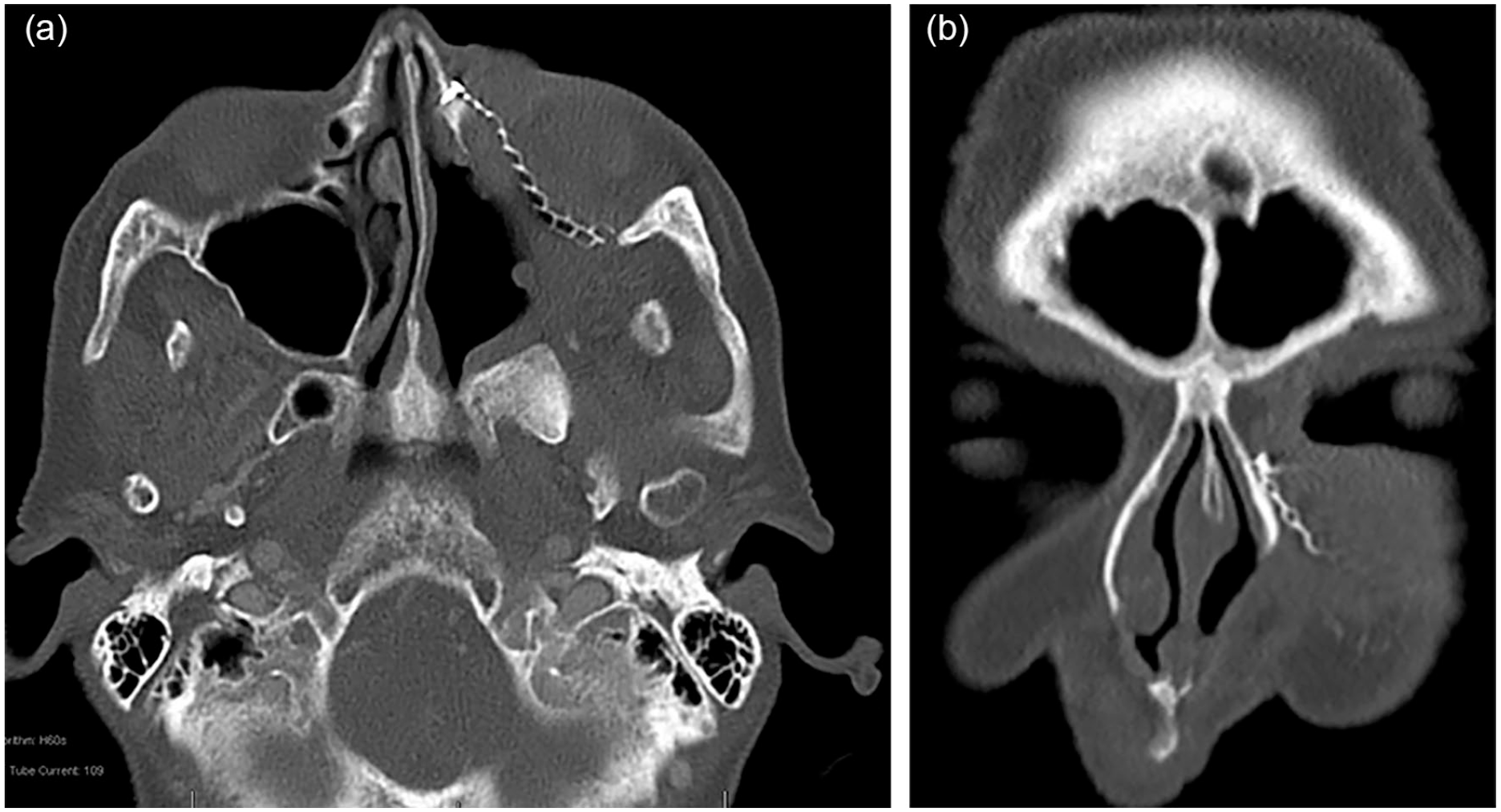
(a) Axial CT of sino. (b) Coronal CT of sinocutaneous fistula.

Intraoperative excision of SCF.
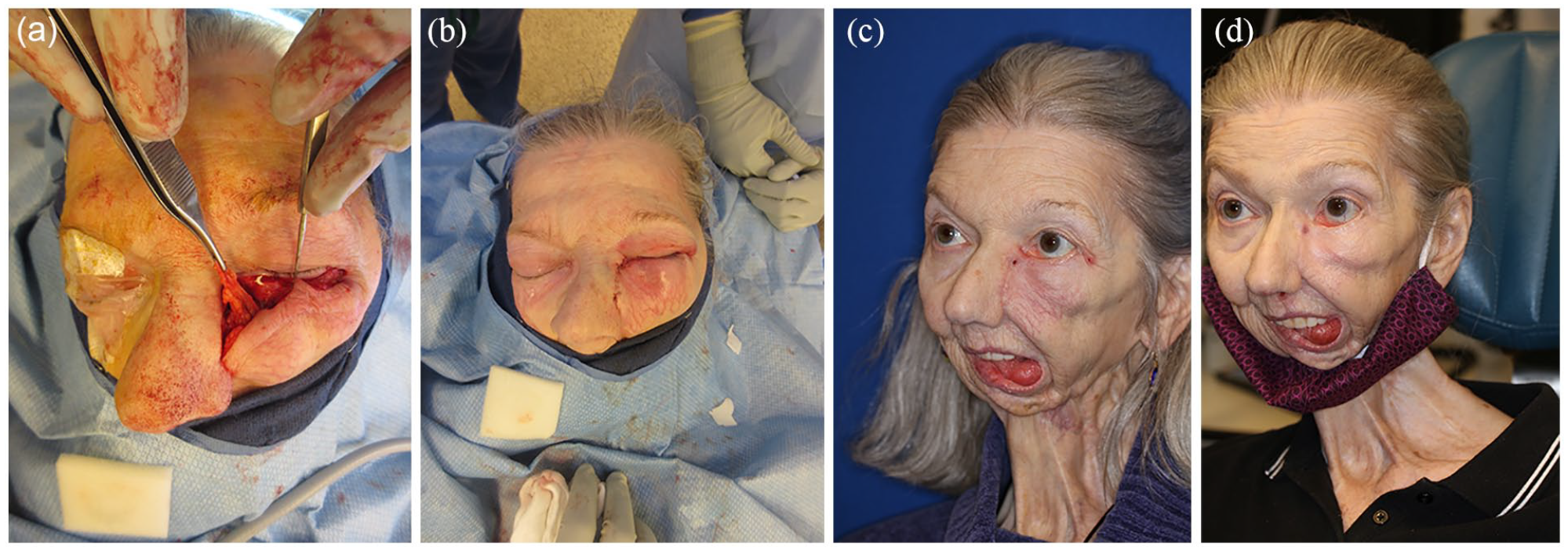
(a) Inferiorly based buccal fat flap covering SCF. (b) Water-tight layered closure. (c) Two months post-operative closure of SCF. (d) Seventh month post-operative result.
Treatment Options
General principles for the reconstruction of SCF include (1) removal of infection including offending hardware, (2) ensuring patency of sinus outflow tracts, (3) tensionless multilayered closure using well vascularized tissue, and (4) prevention or minimization of future risk factors for fistula formation.
Management of the Sinuses
SCF secondary to sinusitis alone usually present in the frontal sinuses as the consequence of an obstructed frontal sinus outflow tract. Surgical treatment involves debridement of infection and nonviable tissue via wide frontal sinusotomy (Draf IIb/Draf III).1,2 Silicone stents can be left in the frontal outflow tract if there is concern for extensive mucosal injury to scar and re-obstruct the outflow tract.1,3 Frontal sinus outflow tract obstructions due to migration of implants or hardware require removal of those entities. Some authors endorse irrigation via trephination of the existing SCF beforehand but no studies have examined the efficacy of this practice. Post-operative care includes saline irrigations, systemic antibiotics, an oral steroid taper, and topical steroid sprays. 1 Stents can safely be removed in 2 to 3 months. 1 Any involved sinus with a pattern of chronic sinusitis in conjunction with a SCF should be addressed endoscopically in addition to management of the fistula to prevent recurrence.
Fistula Closure Techniques
Conservative Management
Small, asymptomatic SCF following orbital exenteration can heal well with routine socket hygiene.1,4 Up to 3 mm SCF have been described to close via this technique over the course of 32 months in patients with minimal risk factors. 1 Primary closure can also be considered in small SCF after the wound has been allowed to heal maximally. 1
Operative Management
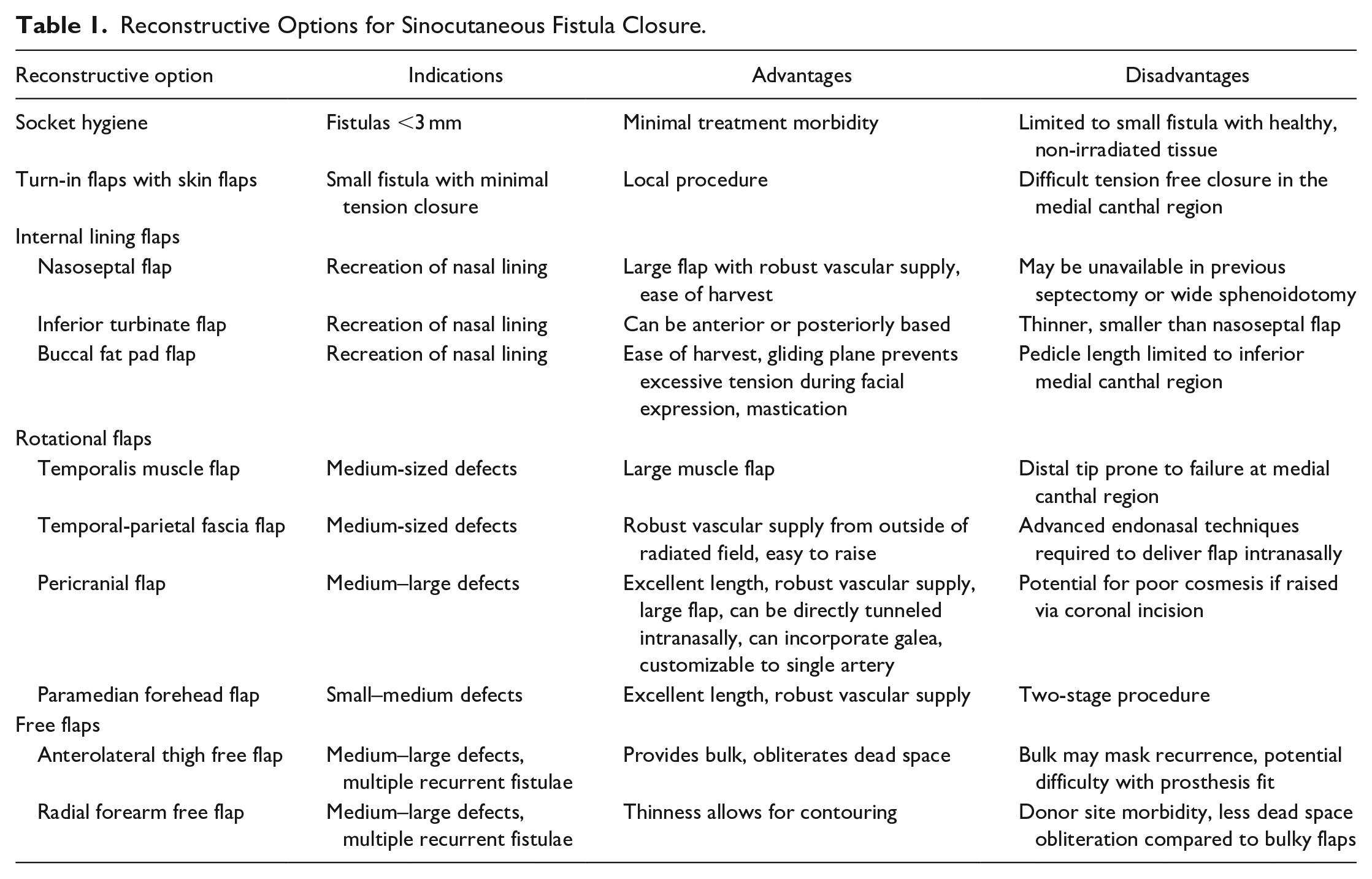
Fistula closure can be approached from the cutaneous side, endonasally, or a combination of approaches. Key components of a successful closure of SCF are using atraumatic surgical technique, complete de-epithelialization of the tract, eversion of flap edges, and tensionless multilayered-closure (Table 1).
Reconstructive Options for Sinocutaneous Fistula Closure.
Turn-in Flaps with Skin Flaps
To recreate the internal lining of a SCF, the cutaneous edges of the fistula itself can be turned in as vascularized flap and sutured together. This allows for reconstruction of the internal defect of the fistula. 5 This alone is not typically adequate for closure. Elevation of a skin flap may then be performed and mobilized to close the cutaneous defect for a 2-layered closure. This skin flap may be a rotation, advancement, rotation-advancement, or an island advancement flap. Multiple designs are possible depending on the location and size of the defect.
Grafts and Endonasal Flaps
Scleral patch grafts and skin grafts for small wounds following orbital exenteration have been described. However, given the need for well vascularized tissue and the necessity of neovascularization, grafts often fail in the medial canthal region following radiation.4,6 Nasoseptal flaps (NSF), and inferior turbinate flaps (ITF) have been described to provide closure from the sinonasal side.4,6
The nasoseptal flap has been well described in the literature and is considered the workhorse in closing sinonasal defects due to its robust consistent vascular supply, ease of harvest, and relatively lengthy pedicle. 7 It is based off the nasoseptal artery, a branch of the posterior septal artery, a terminal branch of the sphenopalatine artery. 7 The flap is raised by making an inferior incision at the superior border of the choana across to the poster margin of the vomer and down to the nasal floor. 8 The inferior incision extends anteriorly along the junction of the nasal septum and floor but can be carried laterally to include the IT mucosa if needed. The anterior-most limit is the junction of the septal mucosa and vestibular skin. The superior incision is begun at the sphenoid os and carried superiorly toward the skull base, leaving 1 cm of mucosa superiorly to preserve olfactory function. The incision is brought anteriorly to the end of the septum. A vertical incision connects the inferior and superior incisions and the flap is raised in a submucoperichondrial and submucoperiosteal plane. 8
The inferior turbinate flap can be considered in patients in which a nasoseptal flap cannot be used secondary to vascular disruption of the blood supply via prior septectomy or wide sphenoidotomies. 9 The flap can either be anteriorly- or posteriorly-based. 10 The anterior-based flap is raised via a Cottle elevator in the inferior meatus that is then pushed superiorly to perforate the bony attachment to the lateral nasal wall. The anterior 1cm of the turbinate remains attached to its native site and the posterior aspect of the IT is detached posteriorly via the Cottle.
The posteriorly-based ITF is based off of the inferior turbinate artery, a terminal branch of the posterior lateral nasal artery (PLNA). 11 The PLNA enters the IT posteriorly at the superior aspect of the lateral attachment approximately 1.0 to 1.5 cm from the posterior tip of the IT. 12 The IT can be medialized to allow for optimal exposure of the mucosa. Parallel incisions superior and posterior to the IT are made and then connected via a vertical incision over the anterior head of the turbinate. 9 The flap is thinner than the NSF and can be made wide by extending the lower incision to the nasal floor and the superior incision as high as the middle meatus. 8 The mucoperiosteum (and bone if necessary) is then elevated in an anterior to posterior direction with care taken to avoid injuring the vascular pedicle. 9 Silicone splints are left in place for 10 to 21 days to protect the denuded lateral wall. 9
Buccal Fat Pad Flap
While regularly used in the closure of oral and palatal defects <5 cm, we describe the novel use of the buccal fat pad flap for the closure of SCF. The buccal fat is distinct from subcutaneous fat and allows for gliding during mastication and protects important structures from damage. The axial flap has a robust vascular supply based off of anastomosing branches of the facial, transverse facial, and internal maxillary arteries. The procedure begins with a 2 to 3 cm incision >2 cm below Stenson’s duct. With the mucosa gently retracted, dissection proceeds until the buccinator and zygomaticus major are cut. Blunt dissection through the muscle allows the fat pad to herniate without injuring its capsule. Small blood vessels overlying the fat pad should be preserved so as to maintain adequate blood supply to the flap. This case was unique in that the patient had a maxillary obturator that allowed the flap to be easily rotated into the lateral nasal area. Previous studies have demonstrated that this flap can be rotated over the maxillary prominence in patients with intact facial skeletons. 13 This flap is an attractive option for SCF closure due to the ease of harvest, strong vascularity, assistance with multilayered closure, and potential to provide a gliding plane for surrounding tissue, preventing excessive tension with facial expression and mastication. In this case, we utilized the buccal fat flap in a 2-layered closure as an internal lining flap covered by vascularized skin flap. If possible, we prefer a 3-layered closure in complex, post-radiated or recurrent cases in the midface or medial canthal regions and the buccal fat flap provides a well-vascularized interposition layer.
Temporoparietal Fascia Flaps
Temporalis myofascial flaps are commonly used in the closure of medial canthal defects. 14 Their ease of harvest and ability to be tunneled into the medial canthal region make them an initial option for many surgeons resecting tumors in this area. However, the distance to the medial canthal region coupled with radiotherapy can put the distal tip of the flap at risk for failure and subsequent fistula formation. 6 Tensionless, multilayered closure is critical to the success of this technique.
The procedure for temporalis based flaps in the begin with creation of the transpterygoid corridor. Total ethmoidectomy, wide medial maxillectomy and SPA ligation are performed. The pterygopalatine ganglion is exposed posterior to the SPA by removing the lateral wall of the maxillary antrum and the posterior maxillary wall. The ganglion is followed medially to identify the vidian nerve and the pterygoid canal. The vidian nerve is transected and the descending palatine vessels and nerve are dissected from the greater palatine canal to displace the contents of the ptyerygopalatine fossa (PPF) inferiorly. Next, the root of the pterygoid plate is exposed. Using a high-speed drill, the anterior aspect of the pterygoid plates is removed and the transpterygoid corridor is created. This dissection can be done entirely endoscopically using 0° endoscopes although the use of transnasal and Caldwell-Luc approaches have been described. 15 Furthermore, inferior turbinectomy or anterior septal window can allow for more superior and lateral views respectively.
A Doppler may be useful in identifying the superficial temporal artery (STA) before flap harvest. A hemicoronal scalp incision or via a Y-shaped incision may be used (Figure 4a and b). The incision should be superficial and not extend deeper than the hair follicles. Dissection proceeds in the subfollicular plane in order to reduce the risk of post-operative alopecia. The anterior limit of the flap should not extend beyond the hairline to minimize the risk to the frontal branch of the facial nerve. After adequate exposure, margins of the fascial flap are incised and the flap is dissected from the cranium superior to the superior temporal line and the deep temporal fascia in the temple. The flap narrows at the pedicle with special attention to preserve the STA and allow adequate flap rotation.
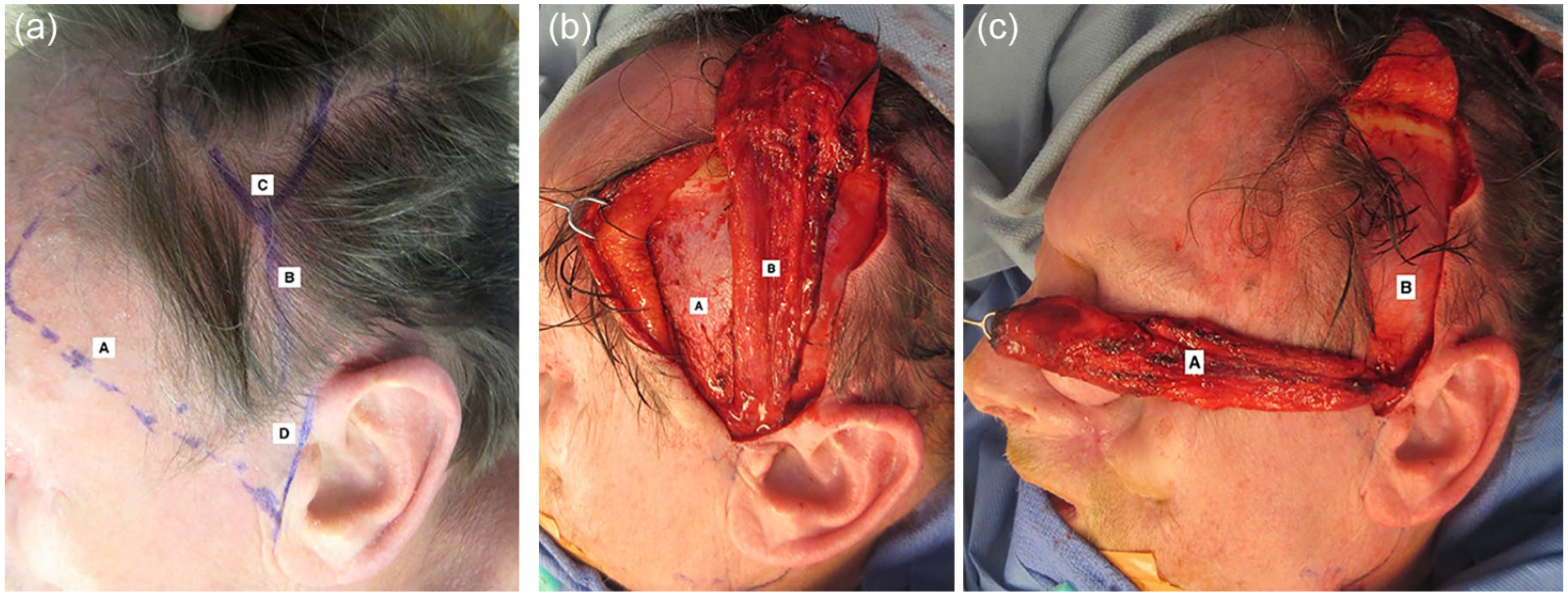
(a) Incision planning for temporoparietal facia flap. (A) Pitanguy’s line, (B) superficial temporal artery, (C) Y-shaped incision, (D) preauricular incision. (b) (A) Superficial layer of deep temporal facia, (B) temporoparietal facia flap. (c) Length of TPF flap is sufficient to treat defects in the medial canthus. (A) temporoparietal fascia flap, (B) superficial layer of deep temporal fascia.
The TPF flap is then connected with the PPF. The superficial layer of the deep temporal fascia is incised several centimeters above the zygomatic arch so as to safely elevate the periosteum off of the arch and minimize risk to the frontal branch of the facial nerve. Additionally, the anterior edge of the temporalis muscle can be elevated off of the lateral orbital wall and pterygomaxillary fissure in order to further develop a soft tissue tunnel.
The soft tissue tunnel is bluntly dilated by passing percutaneous tracheostomy or vaginal dilators over a guidewire or through a 1 in penrose drain deep to the zygomatic arch, lateral to the orbit, and through the maxillary defect. The tip of the wire or penrose is grasped endoscopically. Following adequate dilation, the flap is pulled through via Seldinger technique by securing the flap to the wire or drain with sutures. The internal maxillary artery should be freely mobile within the PPF in order to safely perform this maneuver.
Pericranial Flap
Pericranial flaps allow for a richly vascularized flap outside of previously irradiated fields and can be considered in instances where the temporalis-based flaps cannot reach the medial canthal region.4,16-19 Benefits of the pericranial flap include ease of elevation, large flap size and long reach. Authors have suggested pericranial flaps have better cosmetic results than the paramedian forehead flap while providing a thin flap of well-vascularized tissue. Intranasal coverage may be used but is not required as mucosal cells migrate over the flap, creating a lining similar to native mucosa. 20
The pericranial flap is based off the supraorbital and supratrochlear arteries and can be raised via coronal approach or endoscopically via browlift incisions.21,22 After incision, dissection in a subgaleal plane is directed toward the superior orbital rim. Minimizing separation of the galeal from the pericranium near the supraorbital rim will preserve communicating branches between the superficial and deep vascular systems and enhance the flap’s blood supply. 18 After adequate dissection, the pericranium is incised under direct visualization and tapered to approximately 3 cm in width as it nears the supraorbital rim in order to ensure incorporation of the supraorbital and supratrochlear arteries. However, the flap may be customized as necessary and may be based on a single vessel. Galea can be incorporated into the entirety of the flap for a more robust reconstruction or extended superior to the coronal incision if more length is needed. 23 The flap is then tunneled subcutaneously and sutured to the fistula site. The supraorbital rim and glabella may need to be drilled to avoid pressure on the pedicle.17,18 A skin graft or advancement flaps such as a check advancement flap can be used to cover the flap/fistula superficially. 18
Paramedian Forehead Flap
The paramedian forehead flap is an option for small to moderate sized defects due to its robust and reliable vascular supply in the supratrochlear artery (Figure 5a and b: Paramedian Forehead Flap). Authors have described success using a nasolabial flap to line the sinonasal aspect of the fistula and a paramedian forehead flap to line the cutaneous side. 24 Potential disadvantages of this technique are the creation of 2 donor sites and the need for a 2-staged reconstruction. Alternatively, even if intranasal sources of vascularized tissue is not available, the forehead flap may be folded upon itself to create a multilayered closure as seen in Figure 5c.
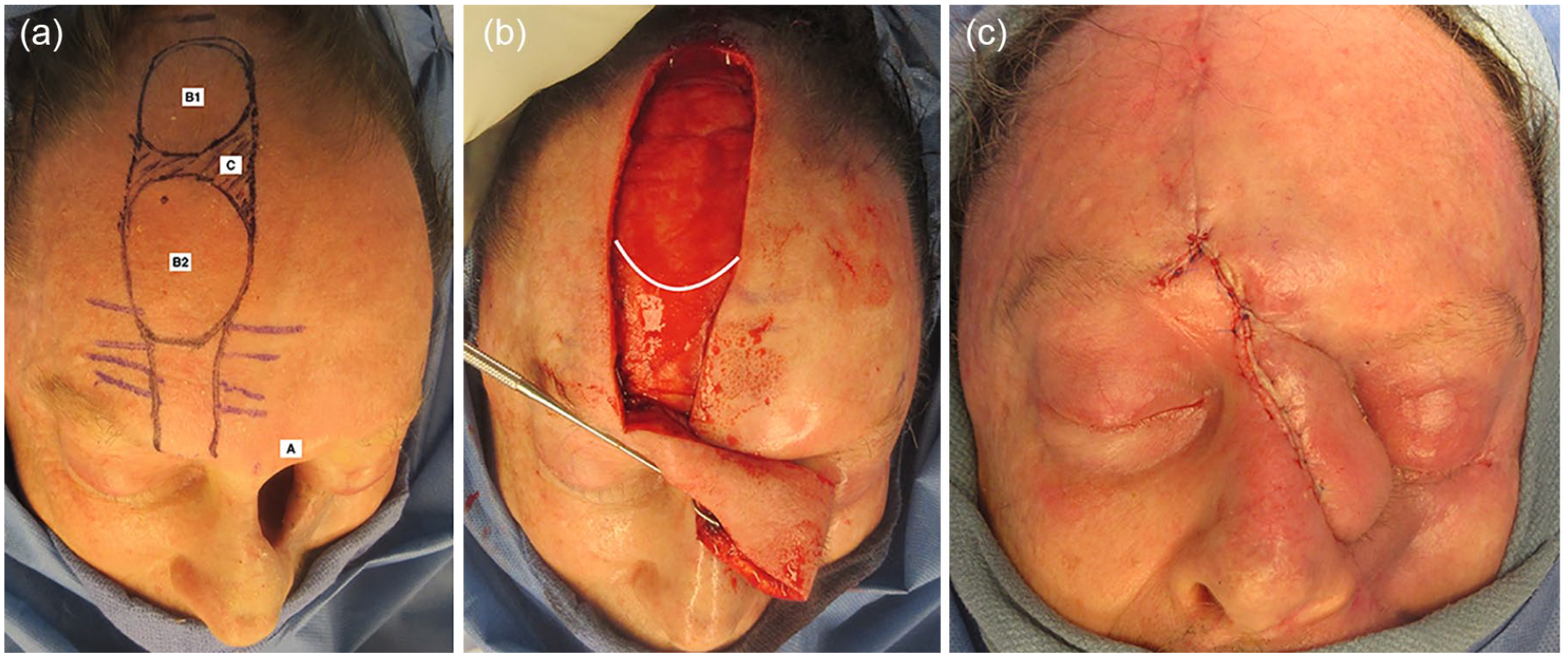
(a) (A) Large sinocutaneous fistula defect, (B1) intranasal portion of paramedian forehead flap and (B2) extranasal portion, (C) area of de-epithelialized tissue for turn-in flap. (b) Turn-in paramedian forehead flap for intranasal lining and external skin. White line demonstrates transition to periosteum to protect pedicle. (c) Immediate post-operative result following division and inset of turn-in paramedian forehead flap for SCF repair.
The flap is based off of the supratrochlear artery, 1.7 to 2.2 cm from midline. Some authors 24 suggest using a Doppler to trace the course of the artery as it improves flap survival and allows for a narrower pedicle base (1.2 cm minimum). 23 A template is made following the contour of the defect and traced onto the paramedian forehead position at a height above the brow equal to the distance from the medial aspect of the brow to the defect. The flap is raised contralaterally in order to decrease the arc of rotation needed to reach the defect and decrease visual obstruction until the flap is divided. Gauze can be rotated from the medial brow as its pivot point in order to assess this distance. Incisions at the distal end of the flap can be made suprafrontalis, subgaleal, or subpericranial. About 1.5 cm superior to the eyebrow, the dissection must be made in a subperiosteal plane to protect the vascular supply. 18
Free Flaps
The role of free flaps in primary closure of large defects at high risk of fistula formation, or of secondary SCF, is to provide a large amount of well vascularized tissue to obliterate the wound. Limawararut et al 6 suggest pre-emptively reconstructing large orbital exenteration defects with free flaps if radiotherapy is anticipated. However a meta-analysis has shown no difference in fistula formation between free flap and other reconstructive options following orbital exenteration.6,25 It is important that these flaps completely obliterate dead space as dead space is hypothesized to serve as a nidus for infection and ultimately, fistula formation. 25
The 2 most common free flaps used for SCF are the radial forearm free flap (RFFF) and the anterolateral thigh (ALT) flap. Variable rates of SCF formation following free flap reconstruction of the primary defect have been reported with rates of ranging from 5.8% to 16%.25-28 The ALT provides good bulk and is ideal for obliterating dead space in the medial canthal and sinonasal region while the RFFF is thin and allows for good contouring. The serratus anterior free flap has also been described in successful SCF closure. 29 While useful in the reconstructive algorithm, bulky flaps may mask tumor recurrence or affect the contour of the orbital rim, making facial prosthesis fitting difficult. 6 Although locoregional flaps are primarily used for closure of SCF, free flaps are an excellent options for large, complex, multiply recurrent fistulae.
Conclusion
SCF are disfiguring and frustrating complications for the patient and the surgeon. Knowledge of predisposing risk factors and reconstructive options give the reconstructive surgeon the best chance at a closing the gap. We describe a novel use for the buccal fat pad flap for successful closure of the fistula at 5 month follow up.
Supplemental Material
sj-docx-1-aor-10.1177_00034894211014299 – Supplemental material for Novel Use of the Buccal Fat Pad for Sinocutaneous Fistulae Closure and a Review of Reconstructive Options
Supplemental material, sj-docx-1-aor-10.1177_00034894211014299 for Novel Use of the Buccal Fat Pad for Sinocutaneous Fistulae Closure and a Review of Reconstructive Options by Christopher Pool, Neerav Goyal and Jessyka G. Lighthall in Annals of Otology, Rhinology & Laryngology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.