
Abstract
Objective:
Post-tracheotomy swallowing function has not been well described in the pediatric population. This study aims to (1) determine differences in swallowing functioning pre- and post-tracheotomy and (2) examine the association between postoperative dysphagia and indication for tracheotomy, age at the time of tracheotomy, and time between tracheotomy and modified barium swallow (MBS).
Methods:
A retrospective chart review was performed on 752 patients who underwent a tracheotomy from 2003 to 2018 and had adequate documentation for review. Patients were included if they received a post-operative MBS. Descriptive statistics, logistic regression, and Fisher’s exact test were used to analyze the data.
Results:
The cohort included 233 patients. The mean age at the time of tracheotomy was 25 months (±50.5). The indications for the tracheotomy were upper airway obstruction (110/233, 47.2%), chronic respiratory failure (104/233, 44.6%), and neurologic disease (19/233, 8.2%). The mean time from tracheotomy to post-operative MBS was 224 days (±297.7). Of the patients who had documented pre- and post-tracheotomy diets, nearly half of patients had improvement in their swallowing function after tracheotomy placement (82/195; 42.1%). Post-tracheotomy MBS recommended thickened liquids in 30.9% of the patients (72/233) and 42.5% (99/233) were recommended thin liquids. The remainder (62/233, 26.6%) remained nothing by mouth (NPO). Patients with neurological disease as the indication for the tracheotomy were more likely to remain NPO (P = .039).
Conclusion:
A tracheotomy can functionally and anatomically affect swallowing in pediatric patients. The majority of our studied cohort was able to resume some form of an oral diet postoperatively based on MBS. This study highlights the need for objective measurements of swallowing in the postoperative tracheotomy patient to allow for safe and timely commencement of an oral diet.
Level of Evidence
Level 3.
Introduction
Pediatric tracheotomy is a procedure with associated morbidity and mortality. An important, but understudied sequelae, is post-tracheotomy dysphagia. 1 The presence of a tracheotomy tube can interfere with the normal physiologic mechanisms of swallowing and has been reported in 50% to 87% of patients with patients with tracheotomies. 2 The tracheotomy tube can anchor the larynx, preventing the normal and protective movement of the larynx superiorly and anteriorly during swallowing. 2 Other protective mechanisms may be compromised including the glottic closure reflex and loss of the ability to generate subglottic air pressure. 3 A study of the physiologic effects on swallow elucidated additional mechanisms of dysphagia which included decreased superior excursion of the arytenoid and epiglottis, slower laryngeal movement including slower opening of the upper esophageal sphincter and slower closing of the vestibule during swallow, and delayed initiation of a swallow response. 4 Additionally, in the pediatric population, tracheotomies are often performed in patients who are already at high risk of dysphagia, further exacerbating this risk.
If dysphagia is left undiagnosed or untreated, aspiration can lead to a number of serious complications including aspiration pneumonias, gastroesophageal reflux, and failure to thrive. 5 However, if aspiration is appropriately recognized as a postoperative risk and correctly identified, interventions can be started to mitigate the aspiration risk. For example, the use of a 1-way speaking valve has been shown to improve oral and pharyngeal sensation and increase subglottic pressure during swallowing, thus decreasing the risk of aspiration.6,7 Additionally, compensatory exercises and maneuvers can be trialed, along with other low-cost modifications such as use of different feeding bottles, nipples, and the initiation of thickened fluids. 8
Given the high risk of dysphagia in pediatric patients with tracheotomies, it is important to characterize the postoperative swallowing patterns to prevent aspiration complications, to allow commencement of early rehabilitation techniques as mentioned above, and to provide appropriate pre-operatively education to families. The aims of this study are to compare swallowing function before and after tracheotomy placement, quantify postoperative swallow results in pediatric patients with tracheotomy, and examine whether post-operative swallowing function was associated with indication for tracheotomy, age at the time of tracheotomy, and time between tracheotomy and modified barium swallow study (MBS).
Materials and Methods
After institutional review board approval (STUDY20060017), a retrospective chart review of electronic medical records (EMR) was performed on consecutive pediatric patients from 2003 to 2018 who underwent a tracheotomy at a tertiary care children’s hospital. Patients were identified through a search of the procedure code for placement of a tracheotomy (CPT 31600, 31601, 31603, 31605, 31610) within the study timeframe. Patients were included if a tracheotomy was performed before the age of 18 and the patient underwent at least 1 post-operative MBS. Demographic data, indication for tracheotomy, and comorbid conditions were collected. Indication for tracheotomy was determined by operative reports and consultation notes from the otolaryngology service. If there was any overlap in diagnoses, the diagnosis that was the primary indication for tracheotomy was used. Neurologic disease was defined as either congenital or acquired and was determined by the Department of Neurology clinic notes. The parameters assessed were pre-tracheotomy diet, MBS results, and recommendation of post-tracheotomy diet before and after the MBS.
Descriptive statistics were used to report the indication for tracheotomy. Patient characteristics were reported as mean (standard deviation) if they were continuous and frequency (percentage) if they were categorical. SPSS version 27 was used for analysis with P < .05 indicating significance. Logistic regression and Fisher’s exact test were used to analyze the data for association between final recommended diet and tracheotomy indication and age at the time of tracheotomy. McNemar’s test was use for paired categorical data and Mann-Whitney U test was used continuous data analysis.
Results
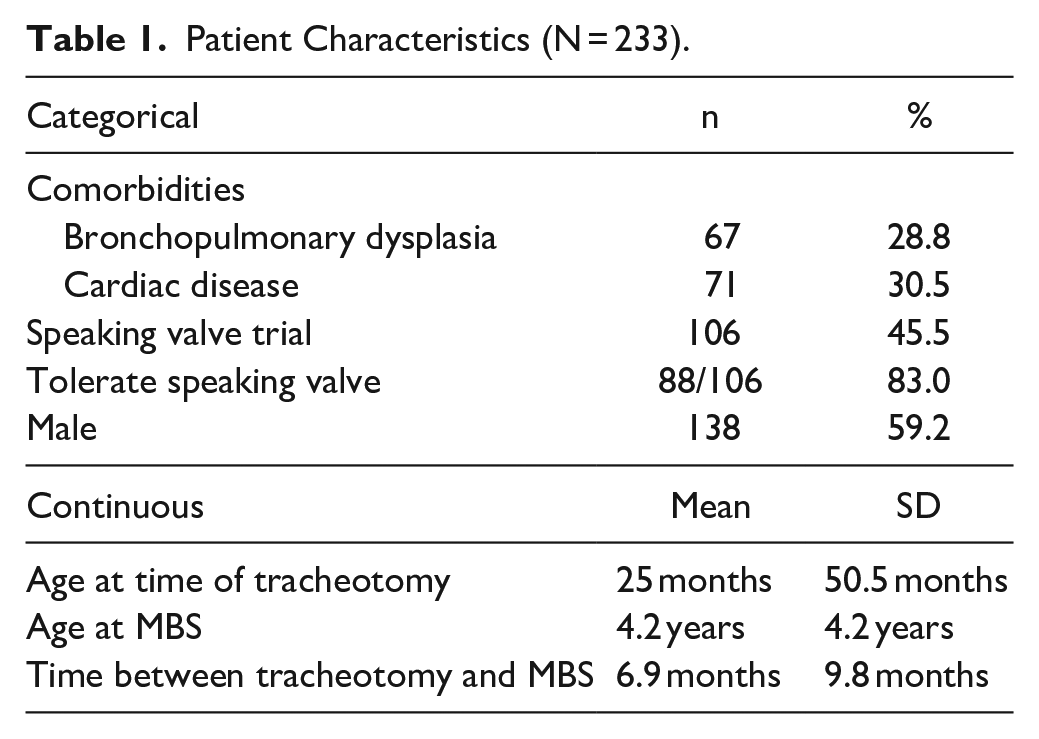
After review of 752 electronic medical records, 233 records met inclusion criteria. Of the 519 patients that were excluded, 359 did not have a post-operative MBS evaluation, 31 patients underwent an additional airway procedure between the tracheotomy and MBS, 40 patients were over 18 years of age at the time of tracheotomy and 89 patients were deceased before initiation of post-operative swallow was attempted. Patient demographic characteristics are summarized in Table 1. Mean age at the time of tracheotomy was 25 months (±50.5). Most children were male (138/233, 59%). Less than half of the patients trialed a speaking valve (106/233, 45.5%) with a majority tolerating the valve (88/106, 83.0%).
Patient Characteristics (N = 233).
The indications for placement of a tracheotomy are summarized in Figure 1. The most common indication for a tracheotomy was upper airway obstruction (110/233, 47.2%) with chronic respiratory failure/pulmonary disease (104/233, 44.6%) as the second most common indication. Neurologic disease represented the indication for the remainder of the cohort (19/233, 8.2%). Acquired verses congenital neurological diagnoses for each patient are shown in Supplemental Material Data.
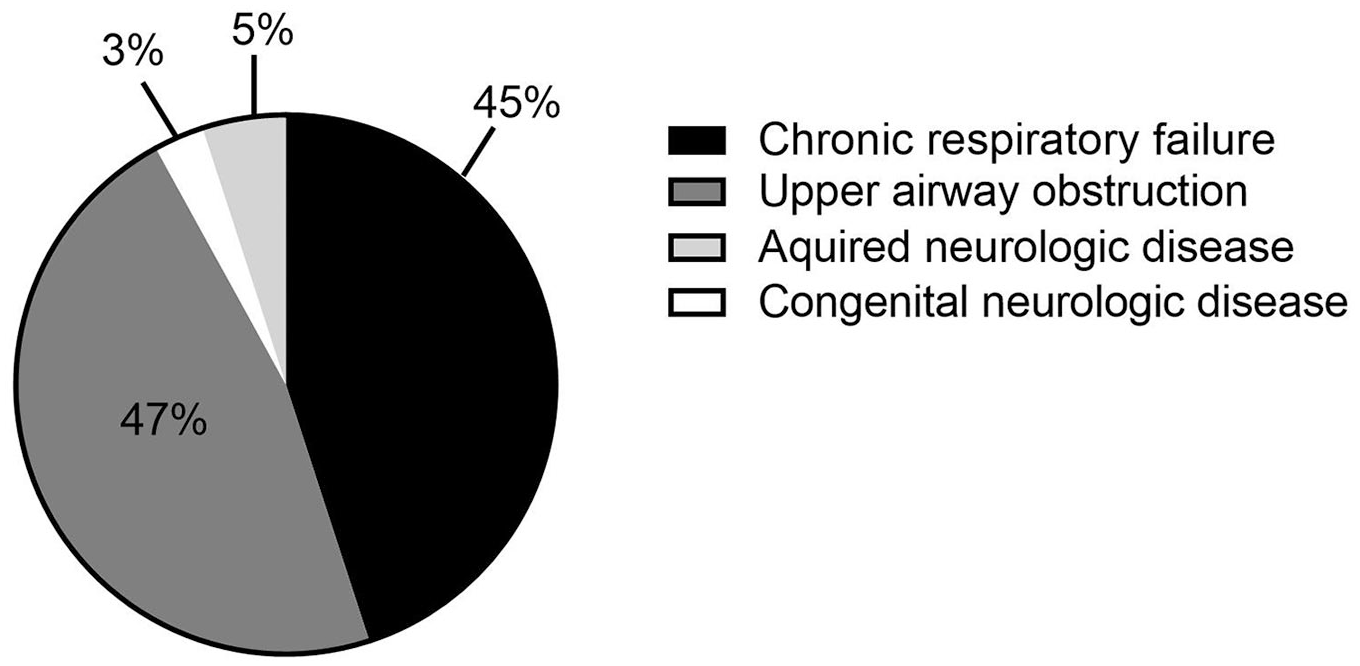
Indications for tracheotomy in our study population.
Patient diets were noted at time of admission to the hospital when tracheotomy tube placement was performed. Pre-tracheotomy, 107/233 (45.9%) patients were NPO, 69/233 (29.6%) were on thin liquids, 19/233 (8.2%) were on thickened liquids and 38/233 (16.3%) were unknown due to missing/unclear/unspecified information. Before tracheotomy, diet recommendations were predominantly determined by clinical evaluation by a multidisciplinary team. However, 55/233 (23.6%) patients had a documented MBS. Of those patients, 3/55 (5.5%) had an inconclusive MBS due to inadequate volume of oral feeds during the study, leaving 52 patients with MBS results that could guide diet recommendations. About 16/52 (30.8%) patients were NPO, 18/52 (34.6%) were cleared for thin liquids, and 18/52 (34.6%) were cleared for thickened liquids.
Table 2 compares diets noted before tracheotomy and diet recommendations post tracheotomy guided by an MBS.
Feeding before Tracheotomy Tube Placement and Feeding Recommended Post-Tracheotomy MBS, n = 195.
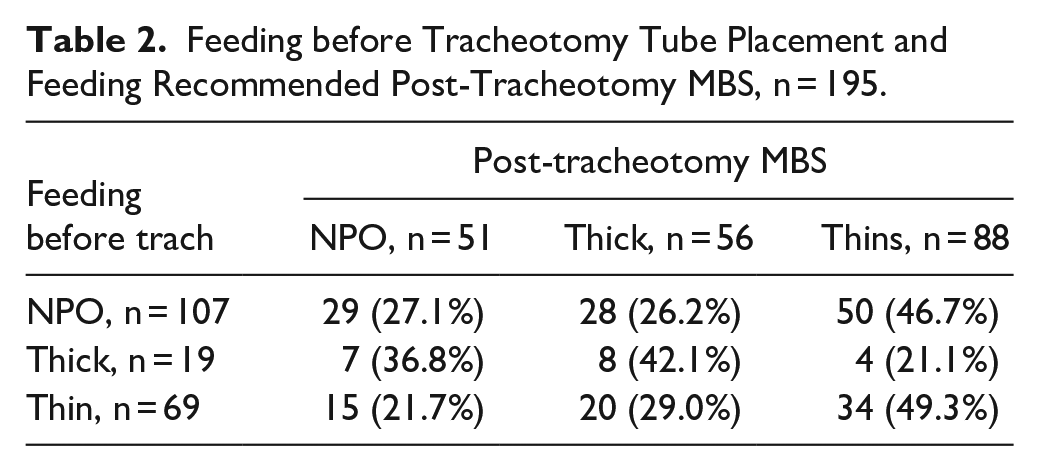
Of the 233 patients who had a post-tracheotomy MBS, 38 had incomplete data, leaving 195 patients for complete pre- and post-tracheotomy feeding recommendations for review. We defined poorer to better feeding as a progression from NPO to thickened liquids to thin liquids. The nearly half of patients (82/195; 42.1%) had their diets advanced after tracheotomy. About 71/195 (36.4%) had the same recommended diet and 42/195 (21.5%) had poorer feeding noted. The majority of those who had poorer feeding post-operatively had airway obstruction (19/42, 45.2%) or chronic respiratory failure/ pulmonary disease (16/42, 38.1%). There was a significant difference in age at tracheotomy between those with their diets advanced, same recommended diet, and poorer feeding, P < .001. Those with poorer feeding after tracheotomy were older at tracheotomy (M ± SD = 4.12 ± 6.20 years) than those with their diets advanced (M ± SD = 0.60 ± 2.62), P < .001 (adjusted p value with Bonferroni correction for multiple tests). However, there was no correlation between age at the time of tracheotomy and ability to tolerate an oral diet (thin or thickened) on post-tracheotomy MBS (P = .575). There were no differences in likelihood of trialing nor tolerating a speaking valve between those with diets that advanced, remained the same, and had poorer feeding (P > .05).
The mean time period between tracheotomy and post-operative MBS was 224 days (±297.7). Patients had clinician recommended diets right after tracheotomy but before their post-tracheotomy MBS was performed. The recommended post tracheotomy diet for patients before and after evaluation with an MBS is shown in Figure 2. In the immediate post-operative period before MBS was performed, the majority of patients were recommended an NPO diet (149/233, 63.9%). Of the patients who were recommended a diet by mouth, 24/233 (10.3%) were recommended thickened liquids and 60/233 (25.8%) were cleared for thin liquids. Diet recommendations were modified after assessment with an MBS. After MBS, the majority of patients were recommended some form of oral diet. Thickened liquids were recommended in 72/233 (30.9%) patients and 99/233 (42.5%) were allowed thin liquids. The remainder (62/233, 26.6%) remained NPO. The long interval of time between tracheotomy and post-operative MBS was due to being too ill to consider oral feeds (76/233, 32.6%) and persistently high ventilatory requirements (5/233, 2.1%). Reasons were unclear by data review in 152/233 (65.2%) patients.
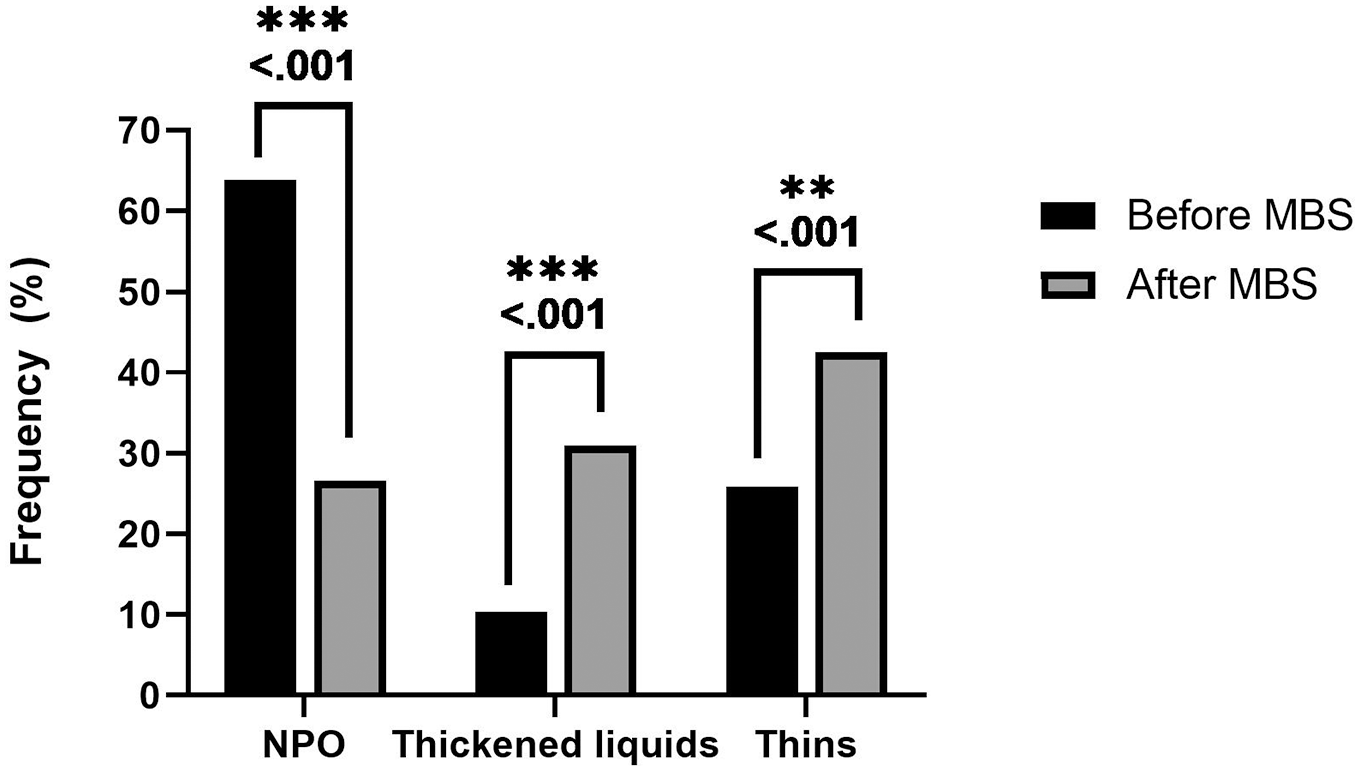
Recommended diets in post-operative tracheotomy patients before and after a modified barium swallow (MBS).
Post-tracheotomy placement, most patients required mechanical ventilation (160/233, 68.7%). About 70/233 (30.0%) did not require ventilatory assistance and it was unknown in 3/233 (1.3%) of patients. At time of MBS, 107/233 (45.9%) of patients were on mechanical ventilation, 117/233 (50.2%) were not, and it was unknown in 9/233 (3.9%). Those that had their diet advanced were 2.4 times more likely to be on mechanical ventilation compared to those with poorer feeding post-operatively, OR = 2.353, 95% CI: 1.091 to 5.075 (P = .029). However, there was no difference in likelihood of an oral feeding (thin or thickened) versus NPO for those with and without mechanical ventilation (P = .829).
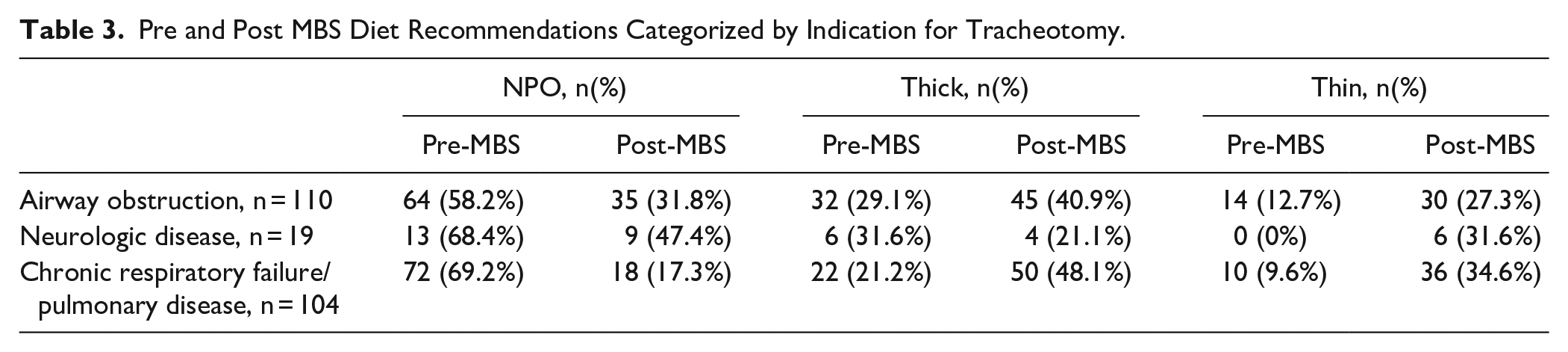
The data was then assessed for correlation between post-tracheotomy diet and indication for tracheotomy. This is represented in Table 3. NPO was the most common diet recommendation post-tracheotomy, pre-MBS across all indications for a tracheotomy. Post MBS, patients with neurological disease had the highest percentage of patients who remained NPO. Patients who underwent a tracheotomy for neurological disease (OR = 0.373, 95% CI: 0.144-0.966, P = .039) and chronic respiratory failure (OR = 2.444, 95% CI: 1.307-4.573, P = .003), were more likely to stay NPO after the MBS when compared to those with upper airway obstruction (OR = 0.625, 95% CI: 0.347-1.128, P = .078).
Pre and Post MBS Diet Recommendations Categorized by Indication for Tracheotomy.
When assessing the most common comorbidities, there was no difference in likelihood of advancing to an oral diet (thick or thin liquids) in patients with congenital cardiac disease versus none (OR = 1.363, 95% CI: 0.709-2.619, P = .353). Those with bronchopulmonary dysplasia (BPD) were 5 times more likely to have an oral diet post MBS compared to those without, (with BPD and oral diet, 61/67 (91.0%) vs without BPD and oral diet, 110/166 (66.3%), OR: 5.176, 95% CI: 2.108-12.707, P < .001).
Discussion
This study showcases a large single center review that presents a representative sample of pediatric tracheotomy patients. Upper airway obstruction was the most common indication for tracheotomy, followed closely by chronic respiratory failure/pulmonary disease, which is comparable to other large tracheotomy populations in the literature.9,10 The mean age of 25 months at the time of the procedure represents a slightly younger population than previously reviewed large cohorts of patients with a tracheotomy. 11
Our data show that the majority of patients, 73%, were safe for oral feeds post-tracheotomy per MBS. This finding is consistent with what is published in the literature. A retrospective review by Joseph et al reported 81% of patients were safe for oral feeds at the time of discharge after tracheotomy. 12 Norman et al 9 reported 81% of post-operative patients had evidence of dysphagia determined with a clinical swallow assessment. By comparison, our study indicates a lower percentage of patients with dysphagia preventing oral intake. In Norman’s study, the use of only a clinical swallow assessment was performed, rather than a fiberoptic endoscopic evaluation of swallowing (FEES) or MBS. Using a clinical assessment method could lead to an underestimation of dysphagia rate due to missed silent aspiration or an overestimate from conservative assessments.
In our population, the average time between tracheotomy and MBS was 224 days. In the time period between tracheotomy and MBS, the majority of patients, 63%, were NPO. This number decreased to 28% after assessment with an objective swallow study. The reason for the long lag time was unclear by chart review in most patients, but severe illness and high mechanical ventilation needs explained the delay in some. A number of factors are known to influence the post-operative swallow including severity of illness, comorbidities, neurological status and assessment by a multidisciplinary team. 12 At our center, post-operative diet is determined by input from otolaryngology, speech, and language pathology and occasionally pulmonology and gastroenterology. FEES is another tool that can be used to assess aspiration and swallowing function. There is significant variability in proceduralist technique, experience and patient cooperation. We intentionally elected to solely evaluate patients who underwent MBS in attempts to create a more uniform cohort. The results raise the question of whether an earlier MBS could lead to patients swallowing sooner. Early introduction of an oral diet could provide this population critical time for oral motor skill practice, shorter time in hospital, and improved quality of life. 13 A better understanding of reasons for delay in swallowing evaluation could identify avenues to more timely evaluation and thus more timely commencement of swallowing.
The indication for tracheotomy is an important variable to consider for dysphagia. Our finding that neurological and respiratory indications for tracheotomy positively correlated with a final NPO diet is consistent with the physiologic mechanisms of swallowing. Neurologic deficit is a known independent risk factor for dysphagia and patients with only upper airway obstruction and normal neurological function may be able to overcome the physiologic swallowing changes caused by a tracheotomy.5,14 Additionally, patients with chronic respiratory failure are more likely to have comorbid risk of aspiration such as prematurity and need for chronic mechanical ventilation.15,16
This study is subject to the known limitations inherent with a retrospective review. The primary outcome that we chose to report was recommended diet post-tracheotomy. This diet recommendation was based on objective findings of the MBS along with clinical information that would contribute to the decision. Factors such as family preference, oral aversion, disease prognosis, or current rehabilitation therapies that could all play an important role in this complex decision were not specifically analyzed. Evaluating these factors could provide more information as to the reason for the diet recommendations post-tracheotomy/pre-MBS, but it would be difficult to standardize across all patients due to the retrospective nature of the study. These data cannot indicate that an earlier MBS would definitely change patient’s outcomes. Delay in the timing of MBS could be due to the critical illness of the patients and readiness for MBS could also indicate readiness for oral intake. Though our results show that the majority of patients had an improved swallowing function based on pre and post-tracheotomy swallow evaluation, this does not indicate that the tracheotomy was the sole reason for this improvement. Patients who require a tracheotomy are typically intubated; therefore, an oral diet is not possible. The retrospective nature of this study relied on documentation of diet pre-tracheotomy and there was limited data as to what a patient’s diet may have been prior to the illness that necessitated tracheotomy placement; this could have falsely elevated the number of patients who had advancement of their diet post-tracheotomy. Additionally, only a small percentage of patients received a pre-operative MBS. Directly comparing pre and post-tracheotomy MBS results prospectively would help shed light on the true impact a tracheotomy has on swallowing function. About half of the cohort had ventilatory requirements. It is likely that this represented a more acutely ill patient population. Due to the retrospective nature of this study, ventilation settings or trials off of the ventilator could not be assessed. Lastly, the categorization of patients by tracheotomy indication relied on accurate charting from the consulting provider and surgeon.
This study is strengthened by being the largest cohort of pediatric tracheotomy patients specifically assessing postoperative swallowing. It is the only study assessing the impact of common comorbidities and indication for tracheotomy on postoperative swallow. The findings highlight a need for timely and objective assessment of postoperative swallowing status in pediatric tracheotomy patients. This applies more specifically to the identified higher risk population who underwent tracheotomy for neurologic or chronic respiratory disease. Prospective studies in the future could better assess the impact of early swallow assessments and examination of other barriers to an oral diet would provide further data in this complex decision.
Conclusion
Pediatric patients with a tracheotomy are at risk for dysphagia, but this risk has not been well defined. This study found that the majority of patients were able to return to some form of an oral diet after objective assessment of swallowing. However, the swallow assessment is often delayed and patients remain NPO for a long postoperative period. This study highlights the consideration for timely and objective measurements of swallowing in postoperative tracheotomy patients.
Supplemental Material
sj-pdf-1-aor-10.1177_00034894211025179 – Supplemental material for Dysphagia in Pediatric Patients with Tracheostomy
Supplemental material, sj-pdf-1-aor-10.1177_00034894211025179 for Dysphagia in Pediatric Patients with Tracheostomy by Kimberly Luu, Michael A. Belsky, Harish Dharmarajan, Thomas Kaffenberger, Jennifer L. McCoy, Kristin Cangilla, Allison B. J. Tobey, Jeffrey P. Simons, Raymond Maguire and Reema Padia in Annals of Otology, Rhinology & Laryngology
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.