
Abstract
Objectives:
To elucidate differences in demographic and clinical characteristics between patients with episodic and chronic dizziness.
Methods:
A cross-sectional, observational study of 217 adults referred for dizziness at 1 tertiary center was undertaken. Subjects were split into a chronic dizziness group (>15 dizzy days per month) and an episodic dizziness group (<15 dizzy days per month).
Results:
217 adults (average age, 53.7 years; 56.7% female) participated. One-third (n = 74) met criteria for chronic dizziness. Dizziness handicap inventory (DHI) scores were significantly higher in those with chronic dizziness compared to those with episodic dizziness (53.9 vs 40.7; P < .001). Comorbid depression and anxiety were more prevalent in those with chronic dizziness (44.6% and 47.3% vs 37.8% and 35.7%, respectively; P > .05). Abnormal vestibular testing and abnormal imaging studies did not differ significantly between the 2 groups. Ménière’s disease and BPPV were significantly more common among those with episodic dizziness, while the prevalence of vestibular migraine did not differ according to chronicity of symptoms. A multivariate regression that included age, sex, DHI, history of anxiety and/or depression, associated symptoms, and dizziness triggers was able to account for 15% of the variance in the chronicity of dizziness (pseudo-R2 = 0.15; P < .001).
Conclusions:
Those who suffer from chronic dizziness have significantly higher DHI and high comorbid rates of depression and anxiety than those with episodic dizziness. Our findings show that factors other than diagnosis alone are important in the chronification of dizziness, an observation that could help improve on multimodal treatment options for this group of patients.
Introduction
Dizziness is extremely common in the adult population, with a 1-year prevalence approaching 11% in the U.S and a lifetime prevalence of greater than one-third.1-3 A multitude of studies have shown that dizziness decreases work productivity, increases social isolation, and contributes to generalized avoidance behaviors that preclude dizziness sufferers from participating in everyday activities.4-6
Dizziness can be subdivided into chronic dizziness and acute dizziness based on a chronicity criterion. For example, Bronstein et al. describe chronic dizziness as evolving from 2 groups of conditions: episodic dizziness (eg, BPPV, Ménière’s disease, migraine), a single episode of vertigo (eg, vestibular neuritis), or a progressive condition (eg, idiopathic bilateral vestibular failure) over time. 7 Chronicity is an important clinical feature of many diseases that should be analyzed because those with chronic features or symptoms can have poorer outcomes. For example, chronic migraine, compared to episodic migraine, has been associated with increased disability, psychiatric disorders, and financial and employment barriers. 8 However, prior investigation into these categories (chronic versus episodic) have been lacking.
The demographic and clinical characteristics that might help predict why some patients suffer from chronic versus episodic dizziness remain poorly understood. Staibano et al 9 found that functional dizziness was more common among patients in a chronic dizziness (>3 months) clinic (21%) compared to those in an acute dizziness (<1 month) clinic (0.5%). This study also found differences in Dizziness Handicap Inventory (DHI) 10 scores between groups. In particular, there was a high percentage (15%) of chronically dizzy patients with a DHI score greater than 60 (severe handicap), as well as a high prevalence of comorbid depression (67%) or anxiety (54%) in the chronically dizzy population. 11
Using a different definition of chronic dizziness (>6 months) and acute dizziness (<6 months), Kruschinski and colleagues showed that, compared to subjects with acute dizziness, those with chronic dizziness were likelier to have experienced one or more falls in the preceding 6 months (38% vs 13%), to report duration of dizzy episodes lasting seconds (59% vs 41%), and to endorse continuous dizziness (20% vs 11.5%). 11
Importantly, these prior studies used duration as the defining feature of acute versus chronic dizziness. Chronicity of dizziness based on frequency of symptoms has not been extensively studied. While many diagnoses do contain duration criteria for episodes of dizziness, diagnosis alone does not distinguish episodic from chronic symptoms, and it is well known that even episodic symptoms can cause chronic suffering and vice versa. Therefore, the purpose of this study was to systematically explore how clinical, audiometric, and vestibular findings might differ between subjects with chronic dizziness and those with episodic dizziness through a cross-sectional study at our tertiary dizziness clinic, using frequency of symptoms as a discriminating factor.
Methods
Institutional Review Board
This investigation was approved by the University of California—San Francisco’s Institutional Review Board.
Setting and Patients
The study population consisted of 217 consecutive adult English-speaking patients evaluated at a tertiary balance and falls center between October 2016 and April 2019. Patients were included only if they had accompanying vestibular testing with a vestibular audiologist.
Data Collection
Standardized new patient templates at the balance and falls center of the study institution are used to ensure uniformity and completeness of data recording. Clinical diagnoses followed Bárány Society criteria, when available.
Data Analysis
All responses and results were stored electronically in Research Electronic Data Capture (REDCap). 12 Subjects were grouped into chronic dizziness (experiencing greater than 15 dizzy days per month) and episodic dizziness (experiencing fewer than 15 dizzy days per month). The whole dataset and the 2 dizziness subgroups (chronic and episodic) were analyzed separately. Stata V.14 (StataCorp, College Station, TX, USA) was used to compute t-tests for differences in continuous variables between the episodic and chronic dizziness groups, and Pearson’s Chi-square test for differences in counts (percentages) between the 2 dizziness groups. Univariate and multivariate regression analysis was undertaken for subgroup analysis of the factors important in predicting episodic versus chronic dizziness.
Results
Total Cohort
Two hundred and seventeen adults (average age, 53.7 years; 56.7% female) were included. Based on our predefined criteria for chronic and episodic dizziness, 74 subjects (34.2%) experienced chronic dizziness, while 143 (65.8%) experienced episodic dizziness. The average DHI score for the full cohort was 45.2 (SD, 25.8). Approximately half (48.8%) had a personal history of migraine, 24.0% had a smoking history (either current or former), and 18.4% had experienced at least 1 fall due to dizziness or imbalance. Comorbid anxiety and depression were common, with 40.1% of the total cohort endorsing chronic depression, 39.6% with anxiety, and a full quarter (25.3%) with both anxiety and depression. Imaging studies were both commonly obtained, with 154 subjects (71.0%) having undergone magnetic resonance imaging (MRI) or computed tomography (CT) imaging, or both (Table 1). Most subjects had undergone VNG testing (91.2%) or VHIT (86.6%), with a smaller number having undergone VEMP testing (35%). Overall, the most common diagnoses, in decreasing order, were vestibular migraine (46.1%), vestibular hypofunction (15.2%), Ménière’s disease (13.4%), BPPV (9.2%), and PPPD (7.8%) (Table 2).
Sociodemographic and Clinical Differences between Chronic and Acute Dizziness.
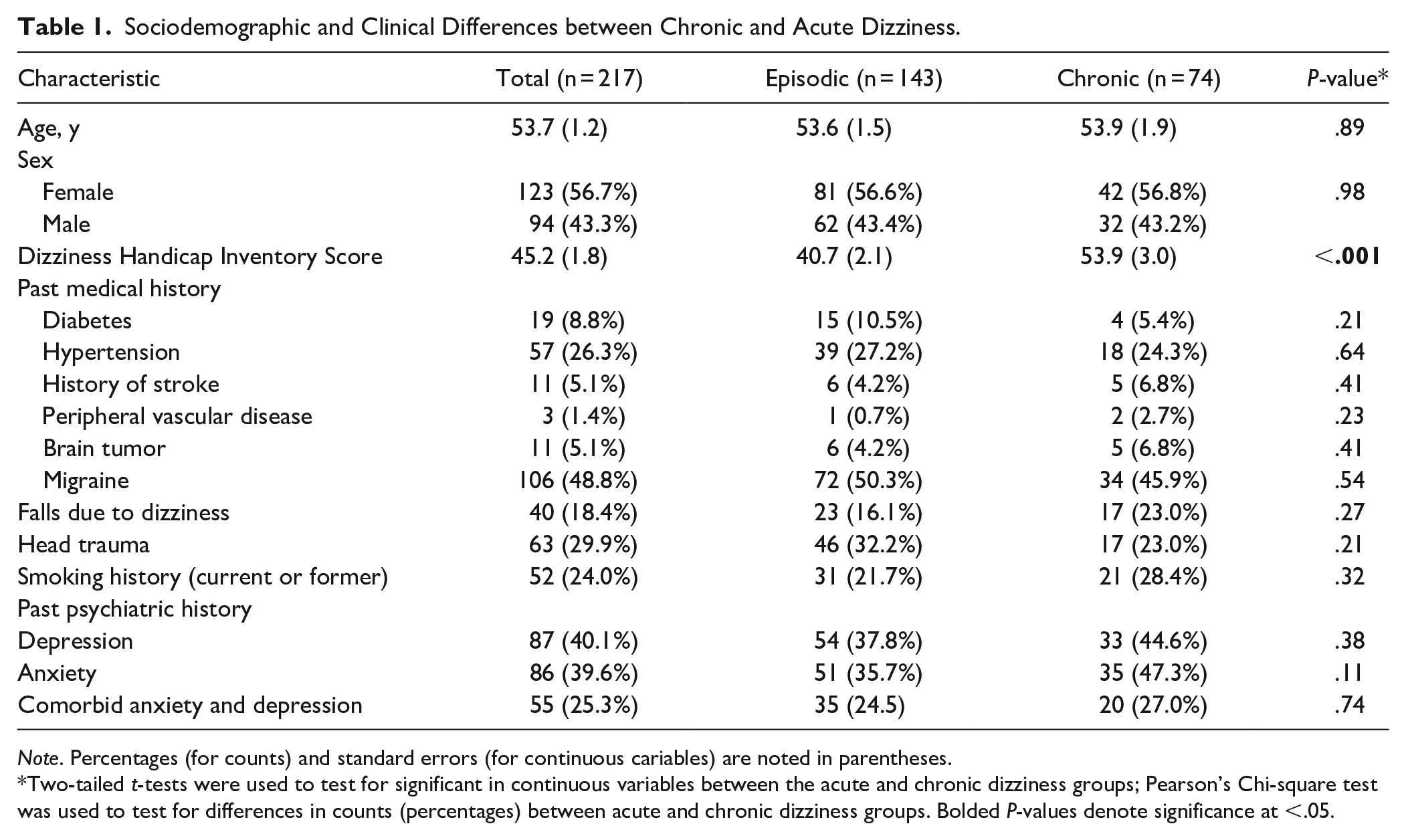
Note. Percentages (for counts) and standard errors (for continuous cariables) are noted in parentheses.
Two-tailed t-tests were used to test for significant in continuous variables between the acute and chronic dizziness groups; Pearson’s Chi-square test was used to test for differences in counts (percentages) between acute and chronic dizziness groups. Bolded P-values denote significance at <.05.
Diagnostic, Audiovestibular, Imaging, and Physical Exam Results, Comparing Chronic and Acute Dizziness.
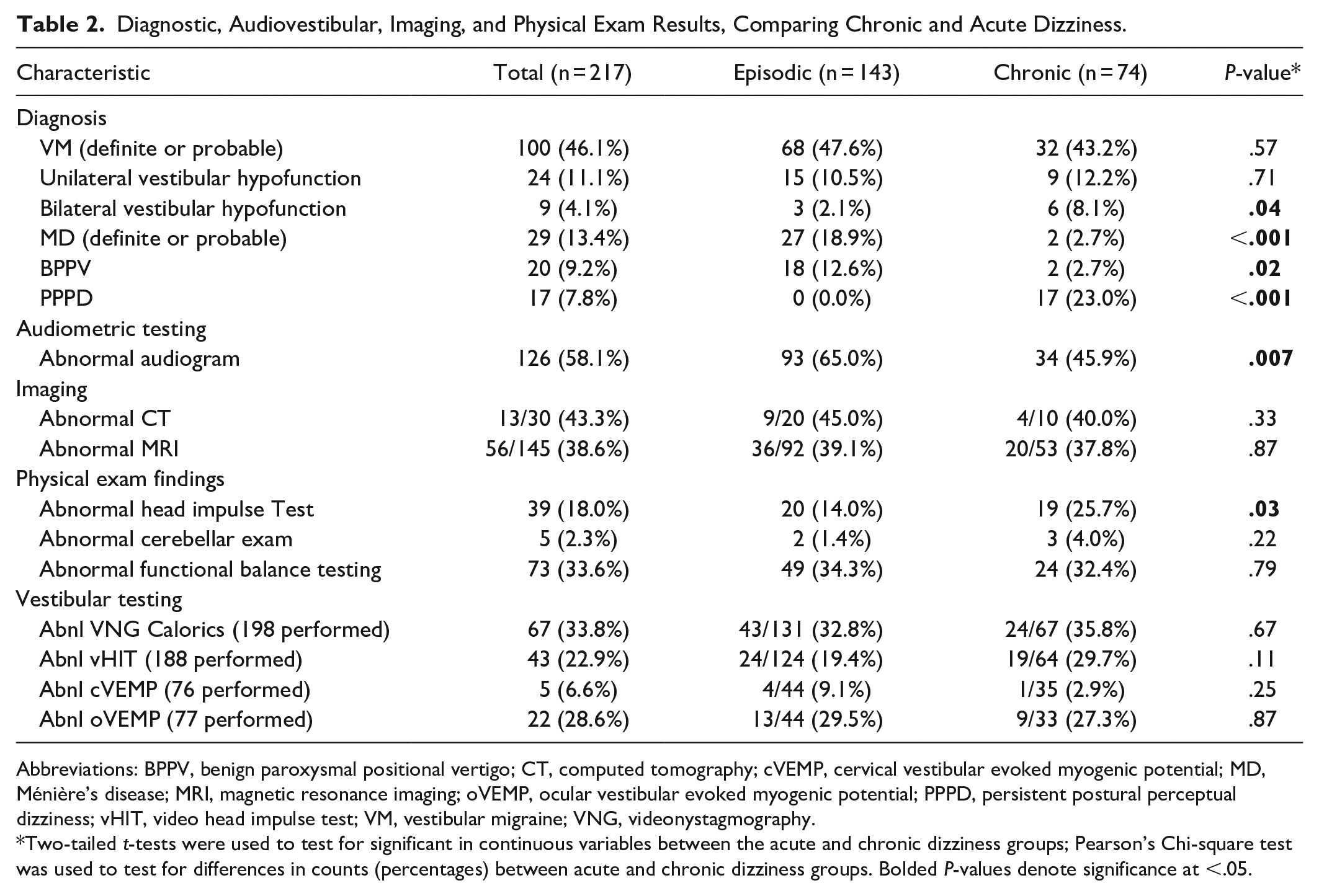
Abbreviations: BPPV, benign paroxysmal positional vertigo; CT, computed tomography; cVEMP, cervical vestibular evoked myogenic potential; MD, Ménière’s disease; MRI, magnetic resonance imaging; oVEMP, ocular vestibular evoked myogenic potential; PPPD, persistent postural perceptual dizziness; vHIT, video head impulse test; VM, vestibular migraine; VNG, videonystagmography.
Two-tailed t-tests were used to test for significant in continuous variables between the acute and chronic dizziness groups; Pearson’s Chi-square test was used to test for differences in counts (percentages) between acute and chronic dizziness groups. Bolded P-values denote significance at <.05.
Episodic Versus Chronic Dizziness
When comparing the episodic (n = 143) and chronic dizziness (n = 74) cohorts, age, percent female, and specific medical comorbidities (hypertension, diabetes, and stroke) did not differ between the 2 groups. A history of migraines was slightly more common in the episodic dizziness group (50.3%) versus the chronic dizziness group (45.9%; P > .05). Likewise, comorbid depression (44.6% vs 37.8%; P > .05) and anxiety (47.3% vs 35.7%; P > .05) were more common in those with chronic dizziness compared to episodic dizziness. DHI scores were significantly higher in those with chronic dizziness compared to those with episodic dizziness (53.9 vs 40.7; P < .001). Abnormal objective vestibular testing and abnormal imaging studies did not differ significantly between the 2 groups, though there was a higher proportion of abnormal vHIT in those with chronic dizziness (29.7%) versus episodic dizziness (18.5%; P = .08). Furthermore, head impulse testing on physical exam was abnormal in a significantly higher proportion of subjects with chronic dizziness (25.7%) compared to those with episodic dizziness (14.0%; P = .03). Abnormal audiograms were more common in those with episodic dizziness (65.0%) versus those with chronic dizziness (45.9%; P = .007). A significantly higher proportion of those with episodic dizziness were diagnosed with Ménière’s disease (18.9% vs 2.7%; P < .001) and BPPV (12.6% vs 2.7%; P = .02) compared to those with chronic dizziness) (Table 2, Figure 1), a finding that accounted for the higher percentage of abnormal audiograms in the episodic dizziness group.
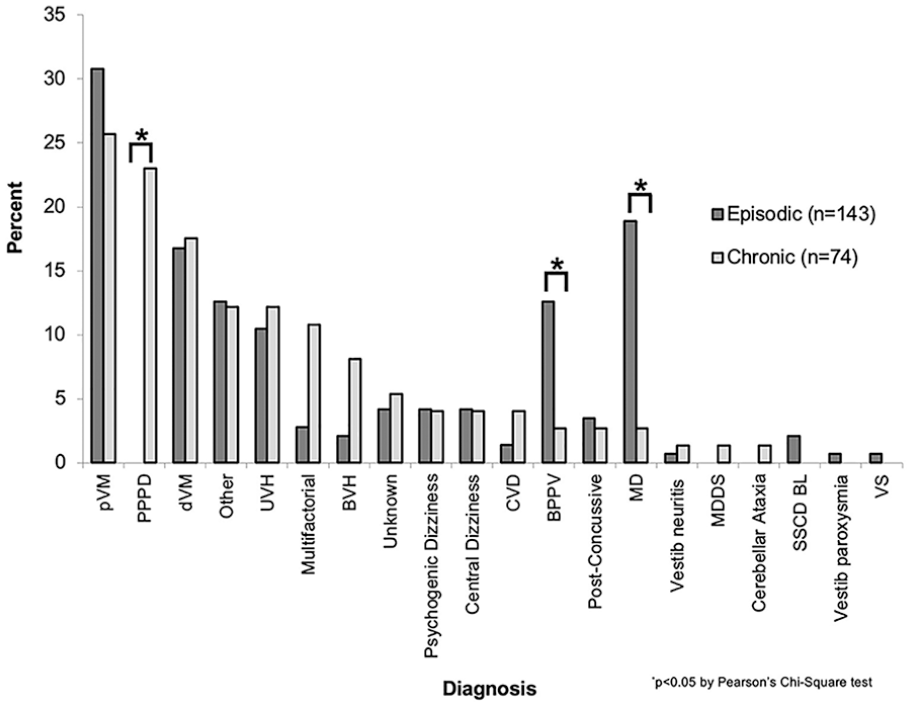
Etiology of dizziness according to episodic or chronic presentation.
Dizziness Triggers and Associated Symptoms
Comparing the chronic and episodic dizziness groups, several differences were noted in triggers of symptoms as well as symptoms experienced during dizziness episodes. Notably, subjects with chronic dizziness identified busy visual scenes (21.6%) or “any body movement” (29.8%) as triggers for their dizziness significantly more often than those with episodic dizziness (9.1% and 18.2%, respectively). Associated nausea or vomiting (53.0%) or a subjective perception of hearing decrement (25.9%) occurred significantly more often in the episodic dizziness cohort than the chronic dizziness cohort (36.5% and 12.2%, respectively; P = .02 for both comparisons) (Table 3).
Dizziness Triggers and Symptom, Comparing Between Chronic and Acute Dizziness.
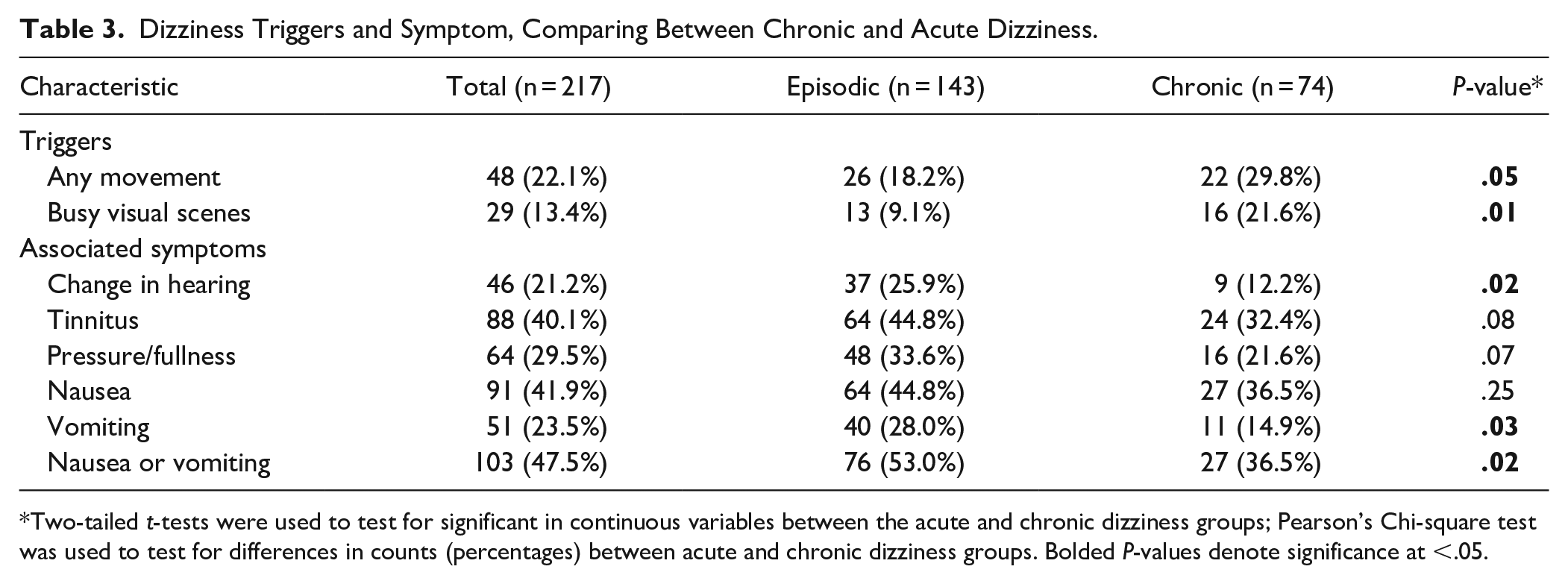
Two-tailed t-tests were used to test for significant in continuous variables between the acute and chronic dizziness groups; Pearson’s Chi-square test was used to test for differences in counts (percentages) between acute and chronic dizziness groups. Bolded P-values denote significance at <.05.
Subgroup Analysis by Dizziness Diagnosis
In order to focus on potential differences between diagnoses that could be explaining the classification of episodic versus chronic dizziness, subgroup analyses with 5 common dizziness diagnoses (VM, MD, UVH, BPPV, and PPPD) were undertaken (Table 4). These subgroup analyses revealed that abnormal audiograms were present at a significantly higher rate in MD (100%), UVH (83%), BPPV (80%), and VM (48%) while only 18% of the PPPD group had abnormal audiograms (P < .01 by Pearson Chi-square test). Thus, the higher percentage of abnormal audiograms in the episodic dizziness group was at least partially explained by the high prevalence of abnormal audiograms in the diagnoses with an episodic preponderance (MD, BPPV). Similarly, the lower rate of abnormal head impulse testing (HIT) in the episodic group (14%) could be partly explained by the fact that 2 diagnoses that were significantly more common in the episodic group (MD and BPPV) rarely showed abnormal HIT results (P < .01 by Pearson Chi-square test) compared to diagnoses that were more common in the chronic dizziness group (UVH, PPPD).
Subgroup Analysis of Audiovestibular and Imaging Findings According to Dizziness Diagnosis for 5 Common Diagnoses.
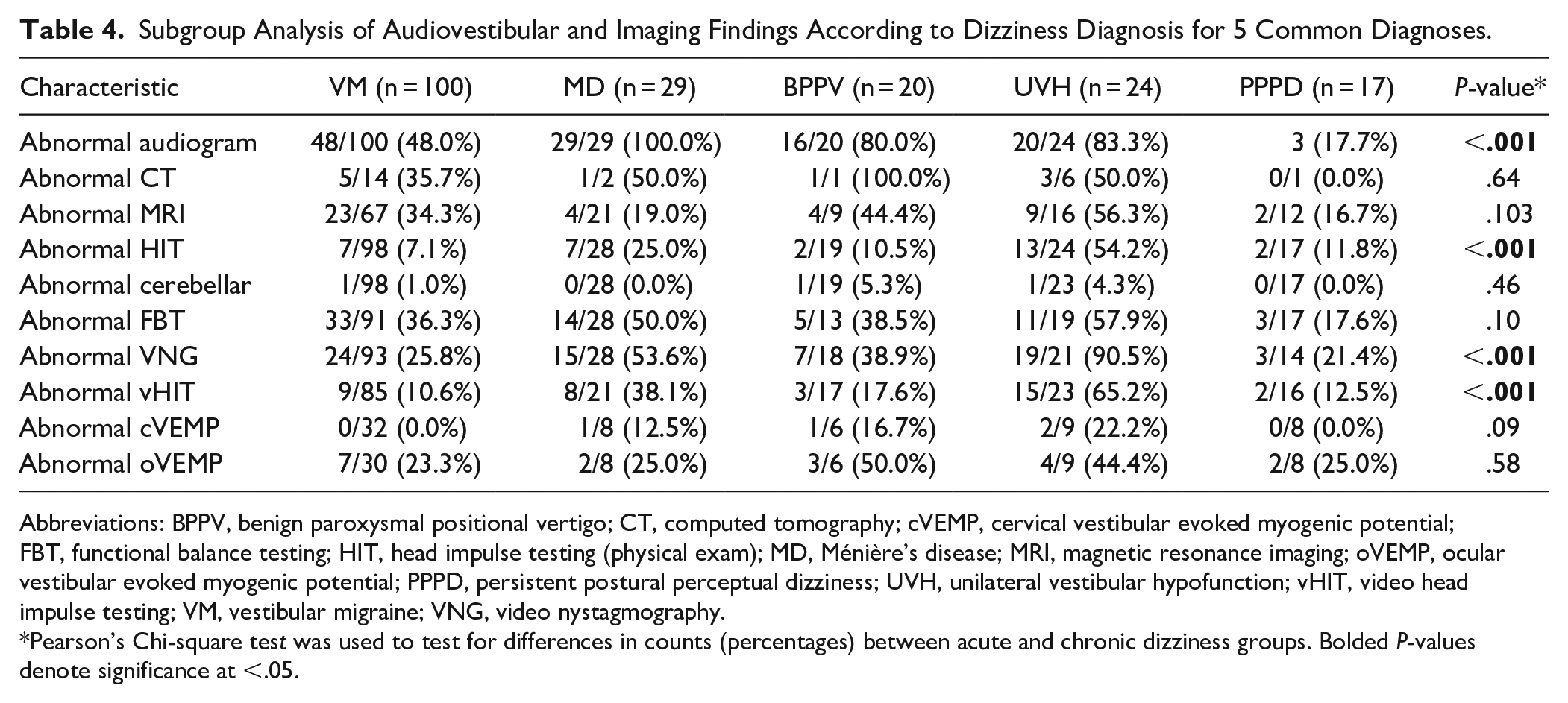
Abbreviations: BPPV, benign paroxysmal positional vertigo; CT, computed tomography; cVEMP, cervical vestibular evoked myogenic potential; FBT, functional balance testing; HIT, head impulse testing (physical exam); MD, Ménière’s disease; MRI, magnetic resonance imaging; oVEMP, ocular vestibular evoked myogenic potential; PPPD, persistent postural perceptual dizziness; UVH, unilateral vestibular hypofunction; vHIT, video head impulse testing; VM, vestibular migraine; VNG, video nystagmography.
Pearson’s Chi-square test was used to test for differences in counts (percentages) between acute and chronic dizziness groups. Bolded P-values denote significance at <.05.
Multivariate Analysis of Predictors of Chronic Dizziness
A multivariate logistic regression that included age, sex, DHI, history of anxiety and/or depression, associated symptoms, and dizziness triggers but did not include a specific diagnosis was able to account for 15% of the variance in the chronicity of dizziness (pseudo-R2 = 0.15; P < .001). After adding each specific diagnosis separately to the model with the aforementioned predictors, the psuedo-R2 for predicting chronic dizziness only changed marginally (0.16-0.22), with the largest increase in pseudo-R2 value occurring when PPPD was added into the model as a diagnosis (Table 5).
Multivariate Analysis of Predictors of Chronic Dizziness.
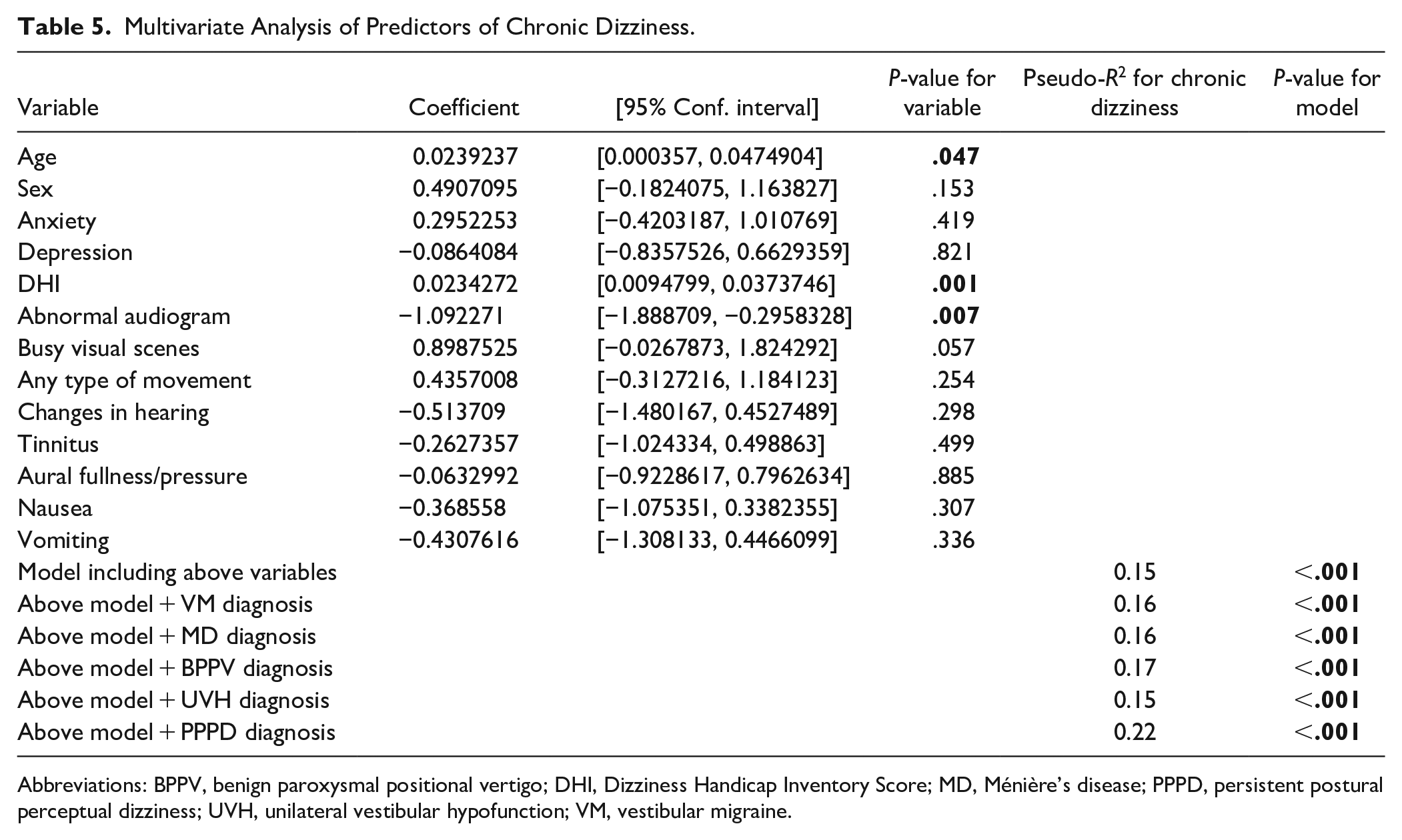
Abbreviations: BPPV, benign paroxysmal positional vertigo; DHI, Dizziness Handicap Inventory Score; MD, Ménière’s disease; PPPD, persistent postural perceptual dizziness; UVH, unilateral vestibular hypofunction; VM, vestibular migraine.
Discussion
In this study, we found that about one-third of those presenting to a tertiary dizziness clinic met criteria for chronic dizziness, and that among this group, depression, anxiety, and DHI scores were significantly higher compared to those with episodic dizziness. Importantly, we showed through an iterative multivariate logistic regression model that diagnosis alone did not account for differences in the distinction between episodic and chronic dizziness.
Very few prior studies exist that attempt to resolve the issue of so-called acute or chronic dizziness.7,9,11 Additionally, these studies used separate definitions for chronic dizziness, focusing on the total duration of symptoms, as opposed to the number of recurrent, discrete episodes. In our chronic dizziness group, fewer than 3% of subjects endorsed dizziness lasting seconds, minutes, or hours, compared to 25%, 38%, and 39% of the episodically dizzy subjects, respectively. The significant difference in dizziness duration categories between the 2 groups suggests our definition of chronic dizziness truly does capture and characterize a group of dizzy subjects who are distinct from those with episodic dizziness. Our study is novel in that we defined chronic dizziness by using a more specific timeline that focused on recording the subject’s frequency of symptoms (dizzy days per month), then sought to find determinants of what might predispose one to experience symptoms chronically. We found that the majority of those presenting to our dizziness clinic (66%) met our definition of episodic dizziness, with 80.4% of subjects in this group describing episodes lasting seconds, minutes, or hours
Similar to other large studies,5,13,14 we found that comorbid depression and anxiety were highly prevalent in both chronic and episodic dizziness groups, occurring in at least one-third of patients in each cohort. In addition, there was a trend toward increasing anxiety in the chronic dizziness group (47.3%) compared to the episodic group (35.7%; P = .11). The high prevalence of comorbid anxiety in the chronic group might be accounted for by catastrophizing, a maladaptive coping mechanism that involves an exuberant cycle of fear and worry related to the condition. Pothier et al 15 recently developed a dizziness catastrophizing scale and showed in a recent analysis of 457 dizzy adults that catastrophizing was independently associated with dizziness related disability, depression, and anxiety. Staab and Ruckenstein 16 have written about the interplay between chronic dizziness and anxiety extensively, and suggested that dizziness and anxiety may reciprocally influence the other—that is, dizziness resulting from vestibular disorders can cause anxiety, and anxiety can negatively modulate preexisting dizziness.
Because of this established interplay between anxiety, depression, and dizziness, 17 depression and anxiety should be aggressively treated, either medically or with cognitive behavioral therapy approaches, 18 in dizzy subjects suffering from these comorbidities. In a prospective trial, Staab et al 19 found that approximately three-quarters of those with chronic subjective dizziness treated with 100 mg of daily sertraline saw improvement in their dizziness symptoms. The interested reader should be directed to a review of the interplay between neurotology and psychiatry. 17
Though diagnosis does predict chronicity of symptoms based on the definition or criteria required to make specific diagnoses, we found clear exceptions to this rule. In particular, syndromes such as BPPV, VM, and MD, which are traditionally thought of as diseases with episodic dizziness, can become chronic for a subset of patients. In the current study group, 32% of those with VM had chronic symptoms, 7% of those with MD had chronic symptoms, and 10% of those with BPPV had chronic symptoms (Table 2). For those in whom dizziness becomes chronic, potentially modulated by a cycle of catastrophizing and maladaptive signal processing of body movement, treatment approaches should be different than those with symptoms that only last minutes to hours.
A noteworthy finding from our analysis is that slightly greater than one-third of subjects referred for dizziness evaluation endorse symptoms on more than half of the days of any given month. Although the DHI itself does not assess chronicity or frequency of symptoms, 20 our study design allowed us to determine that those with chronic symptoms suffer at a statistically significantly higher level (average DHI, 53.9) compared to those with episodic symptoms (average DHI, 40.7; P < .001). We previously reported that depression, anxiety, and quality of life as measured by validated questionnaires are all significant predictors of increased DHI scores in the dizzy population, and that the number of dizziness days per month in particular accounted for 18% of the variance in DHI scores. 14 Thus, it is not surprising that depression and anxiety were significantly higher in those with chronic dizziness symptoms.
Subjects with chronic dizziness identified busy visual scenes and any bodily movement as elicitors of their dizziness at a higher rate than those with episodic dizziness (29.8% and 21.6% for any movement and busy visual scenes, respectively, vs 18.2% and 9.1% in the episodic cohort; P = .05; P = .01). This finding illuminates important factors that could contribute to chronification of dizziness symptoms. In particular, these data suggests that motion sensitivity might underlie a larger maladaptive sensory processing that in turn could lead to chronification of dizziness symptoms. It is well known that migraineurs are much likelier to suffer from motion sickness, even during interictal states. 21 Investigators have characterized this sensitivity to motion or perception of motion as arising from an impaired ability to resolve the “intravestibular sensory conflict” that occurs when signals are received from the otolith organs and semicircular canals simultaneously due to inability for the brain to centrally suppress these conflicting stimuli. 22 The distressing nature of these episodes could then lead to further stress due to anticipation and dread of future episodes, thereby increasing sensitivity to motion. 21 It is reasonable to hypothesize that migraineurs with chronic dizziness symptoms have suffered from particularly maladaptive responses to stress and symptoms that lead to chronification, perhaps in part due to increased motion sensitivity leading to a state of chronic anxiety or worry about the next episode.
In subjects who experience visual or motion hypersensitivity as triggers or exacerbators of chronic dizziness, as is commonly true in vestibular migraine,23,24 patients may benefit from vestibular rehabilitation exercises. Both optokinetic exercises and vestibular ocular reflex adaptation exercises have been shown to be effective in those with chronic dizziness with motion sensitivity or visual hypersensitivity.24,25 In addition to reducing DHI scores in those with vestibular migraine, 26 there is at least one report which describes the efficacy of triptans (eg, rizatriptan) for specifically reducing motion sensitivity in migraineurs. 27
To further explore the distinction between episodic and chronic dizziness, we performed a multivariate analysis that included selected associated symptoms and dizziness triggers, as well as age, sex, DHI score, and abnormal audiogram findings, in order to construct a model that could help account for the variance in chronic dizziness (Table 5). We found that this model could only predict about 15% of the variance (pseudo-R2 = 0.15), a finding that essentially did not change after adding in specific diagnoses that would be expected to account for variance in episodic versus chronic dizziness classification (eg, MD, BPPV). Only the addition of PPPD as a specific diagnosis increased the model’s ability to account for the variance appreciably (pseudo-R2 = 0.22; P < .001). This supports the argument that diagnosis alone does not fully explain the existence of chronic dizziness for some. The remaining 85% of the variance in those with chronic dizziness symptoms is a topic of discussion that warrants investigation in future studies. For example, the SF-36 quality of life questionnaire was absent from the present study, which we previously showed to be one of the singular factors most strongly correlated with DHI scores (R2 = 0.59, P < .001). 14
Migraine is an extremely common disease entity and can overlap considerably with other otogenic sources of dizziness, 28 including PPPD 29 and Ménière’s disease. 30 Migraines should be treated to the fullest extent, as we have found that treating migraine can mitigate dizziness symptoms of other peripheral vertigo etiologies. We start conservatively with a headache diary and migraine elimination diet, followed by initiation of amitriptyline or nortriptyline with increasing daily dosage for those who do not respond, and consideration of an SSRI or SNRI if there are features of significant anxiety, depression, or mood lability associated with headaches.
Limitations
This study is subject to several limitations. First, it is a retrospective, single institution study that reflects the experiences of the referral base to a single geographic region in the United States. Second, though the sample size (n = 217) is comparable to many other studies of dizzy patient characteristics, increasing the number of subjects could further crystallize existing relationships or elucidate new associations. Additionally, we chose what we regarded as a reasonable cutoff for defining “episodic” versus “chronic” dizziness, given no validated definition exists. It is possible that differences in outcome measures for the current cohorts could change based on more stringent criteria. Lastly, there is always the risk of recall bias when using patient questionnaires.
Conclusions
In conclusion, we present a novel analysis of the characteristics of dizzy subjects according to the chronicity with which they experience dizziness symptoms. Among subjects with chronic dizziness, significantly higher DHI scores and higher rates of comorbid depression and anxiety were found. Anxiety and depression should be treated to help mitigate or prevent the processes of chronification and catastrophization. Similarly, providers should ask about and adequately treat migraine headaches, regardless of the etiology of dizziness or vertigo, to help minimize symptom burden in any dizzy patient. Lastly, vestibular rehabilitation exercises should be considered in any subject who offers a history of motion or visual hypersensitivity.
Footnotes
Authors’ Note
This work was presented at the Combined Otolaryngology Spring Meetings in Atlanta, GA, April 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.