
Abstract
Objective:
To evaluate the cost-effectiveness of open versus endoscopic surgical repair of Zenker’s diverticulum.
Methods:
In this study, an economic decision tree was utilized to compare the cost-effectiveness of open surgery compared to endoscopic surgery. The primary outcome in this analysis was the incremental cost-effectiveness ratio (ICER) that was calculated based on the economic decision tree. The probability of post-operative esophageal perforation complications, revision rates, and effectiveness of each procedure along with associated costs were extracted to construct the decision tree. Univariate sensitivity analysis was then utilized to determine how changes in esophageal perforation rate affect the cost-effectiveness of each surgical approach.
Results:
The ICER of open surgery for Zenker’s diverticulum was $67 877, above most acceptable willingness to pay (WTP) thresholds. Additionally, if the probability of esophageal perforation with endoscopic surgery is above 5%, then open surgery becomes a more cost-effective option. Probabilistic sensitivity analysis using Monte Carlo simulations also showed that at the WTP thresholds of $30 000 and $50 000, endoscopic surgery is the most cost-effective method with 83.9% and 67.6% certainty, respectively.
Conclusion:
Open surgery and endoscopic surgery are 2 treatment strategies for Zenker’s diverticulum that each have their own advantages and disadvantages that can complicate the decision-making process. With no previous cost-effectiveness analysis of open versus endoscopic surgery for Zenker’s diverticulum, our results support the endoscopic approach at most common WTP thresholds. Particularly with the current focus on rising healthcare costs, our results can serve as an important adjunct to medical decision-making for patients undergoing treatment for Zenker’s diverticulum.
Keywords
Introduction
Zenker’s diverticulum is a false diverticulum defined by an outpouching of esophageal mucosa into an area between the inferior pharyngeal constrictor and cricopharyngeus muscles known as Killian’s triangle.1,2 It can present as dysphagia and regurgitation in middle-aged adults and elderly patients during the seventh and eighth decades of life. 1 Treatment of symptomatic diverticulum has evolved over the last century and is accompanied by either (1) open surgery with cricopharyngeal myotomy or (2) the less-invasive endoscopic stapling or laser-assisted diverticulectomy with myotomy.3,4 Despite technological advances in endoscopic surgery that has led to this as a popular surgery option, 2 there continues to be debate of the effectiveness between open surgery and endoscopic surgery. 5 Open surgery has long been the conventional treatment, but it has been shown to result in higher complication rates, lengthy hospital stays, longer recovery time to oral diets, and significantly increased total hospital charges than endoscopic surgery. 6 However, endoscopic surgery can be associated with higher recurrence rates, thus requiring more revision surgeries and increasing the overall cost.3,5,7,8 With the lack of consensus on the effectiveness of 1 treatment versus the other, it is important to develop a more tailored selection approach that includes not only the patient’s surgical candidacy, but also the financial burden on the healthcare system.
In this study, an economic decision tree (based on the United States payer perspective) was utilized to compare the cost-effectiveness of open surgery compared to endoscopic surgery. With the advent of new technology and rising healthcare costs, it is important for physicians to consider the effectiveness along with the economic impact of medical treatments and operations available to patients. 8 The purpose of this evaluation is to increase understanding of the cost-effectiveness of open surgery and endoscopic surgery and promote improved patient decision-making in the context of Zenker’s diverticulum.
Methods
IRB approval was not needed for this project since all the data were extracted from previously published studies and no individual patient data was collected or used in this analysis. Detroit Medical Center (DMC) Institution Review Board waived the requirement for IRB. The primary outcome in this analysis was the incremental cost-effectiveness ratio (ICER) that was calculated based on the economic decision tree. The decision tree and subsequent cost-effectiveness analysis were performed using TreeAge Pro software (Version 2020). The ICER calculates the ratio of additional costs associated with a new intervention compared to the newly added benefit.
9
It is calculated by the following equation:
Economic Analysis
A decision tree model was constructed to simulate the surgical decision-making process of patients with Zenker’s diverticulum. The first node includes 2 decisions (to perform open or endoscopic surgery) in which the hypothetical patient would enter each decision by chance. Further decisions then included average length of surgery post-procedure, possible postoperative complications, and revision rates after surgery. Finally, effectiveness for each outcome was assigned based on prior quality of life studies in this patient population.
All probabilities were extracted from retrospective and meta-analysis studies summarized in Tables 1 and 2. The PubMed search engine was used to search for academic articles including the following terms: “Zenker’s diverticulum,” “open surgery OR open repair,” “endoscopic surgery OR endoscopic repair OR endoscopic technique.” Studies that compared open versus endoscopic treatment of Zenker’s diverticulum were included. Conversely, studies that did not compare both techniques were excluded. Surgery costs were based on the current procedural terminology (CPT) codes 43 130 for open surgical excision of Zenker’s diverticulum and 43 180 for endoscopic treatment of Zenker’s diverticulum that was reported by 2 large hospital systems in Southeast Michigan as summarized in Table 3. Additional hospital costs were also calculated based on the cost and number of hospital stays,6,15 and cost of major complications. 16 Effectiveness for each procedure was inferred from a previous study utilizing Gastrointestinal Quality-of-Life surveys obtained in patients undergoing open or endoscopic surgical repair. The survey includes self-reported pertinent symptoms including dysphagia, choking, regurgitation, and halitosis. 4
Complication Rate of Open Surgery and Endoscopic Surgery.
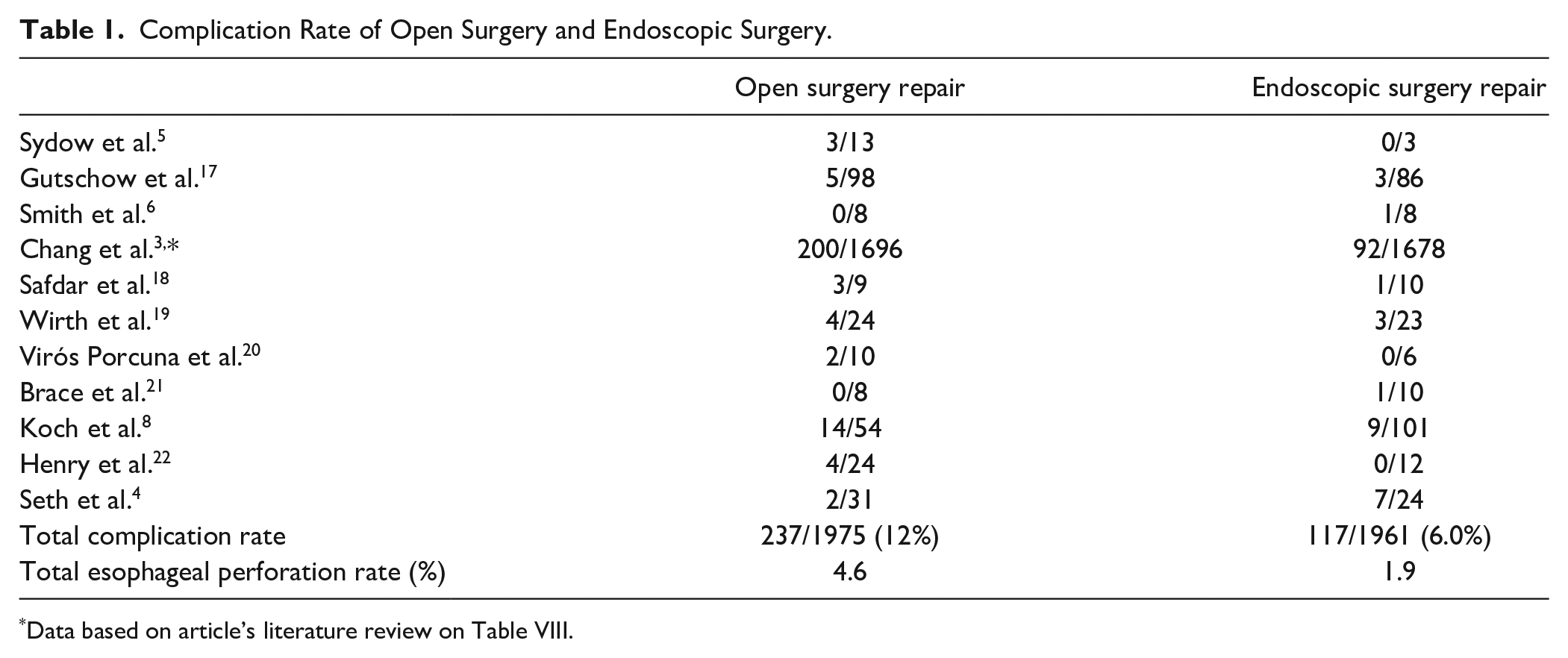
Data based on article’s literature review on Table VIII.
Revision Rate of Open Surgery and Endoscopic Surgery.
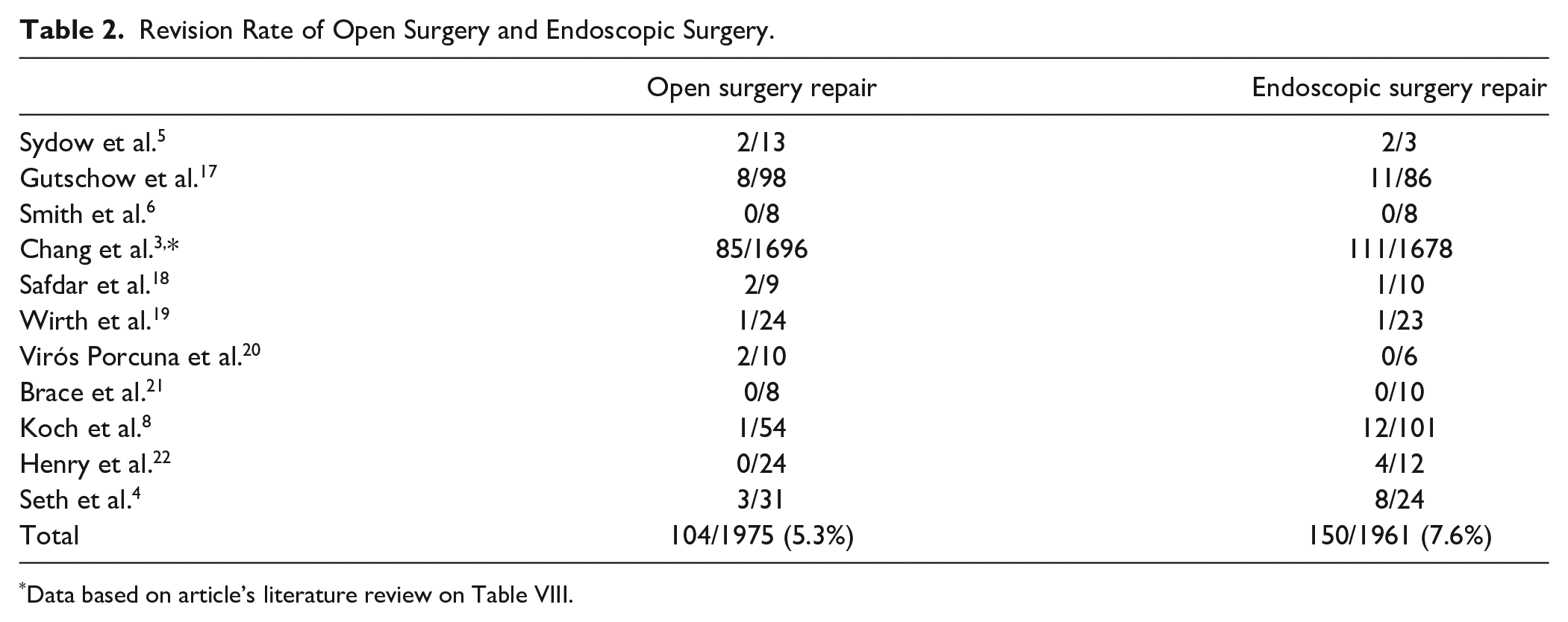
Data based on article’s literature review on Table VIII.
Costs of Open Surgery and Endoscopic Surgery.

Statistical Analysis
Univariate sensitivity analysis was used to determine what the probability of having a complication such as esophageal perforation would have to be to make 1 surgical approach more cost-effective than the other. The increase in probabilities required was set at $30 000 and $50 000 willingness-to-pay (WTP) thresholds that sets a predetermined monetary value for the maximum amount to be paid for every additional unit of effectiveness gained from a treatment choice. WTP thresholds ranging from $25 000 to $50 000 is often used in standardized healthcare economic analyses such as the National Institute of Health and Care Excellence in the United Kingdom when recommending the cost-effectiveness of new treatments. 23
Multivariate probabilistic sensitivity analysis was also performed with 10 000 hypothetical Monte Carlo simulations to determine the cost-effectiveness acceptability curve and the degree of certainty that 1 decision is more cost-effective than the other choice at each WTP threshold. The 2013 Consolidated Health Economic Evaluation Reporting Standards guidelines were followed for this economic evaluation. 24
Results
Utilizing the economic decision tree, the overall cost of using open versus endoscopic surgery of Zenker’s diverticulum were $48 433 and $34 179, respectively, with an incremental cost-effectiveness ratio of $67 877 for open surgery that is above the acceptable WTP thresholds of $30 000 and $50 000. (Figure 1, Table 4).
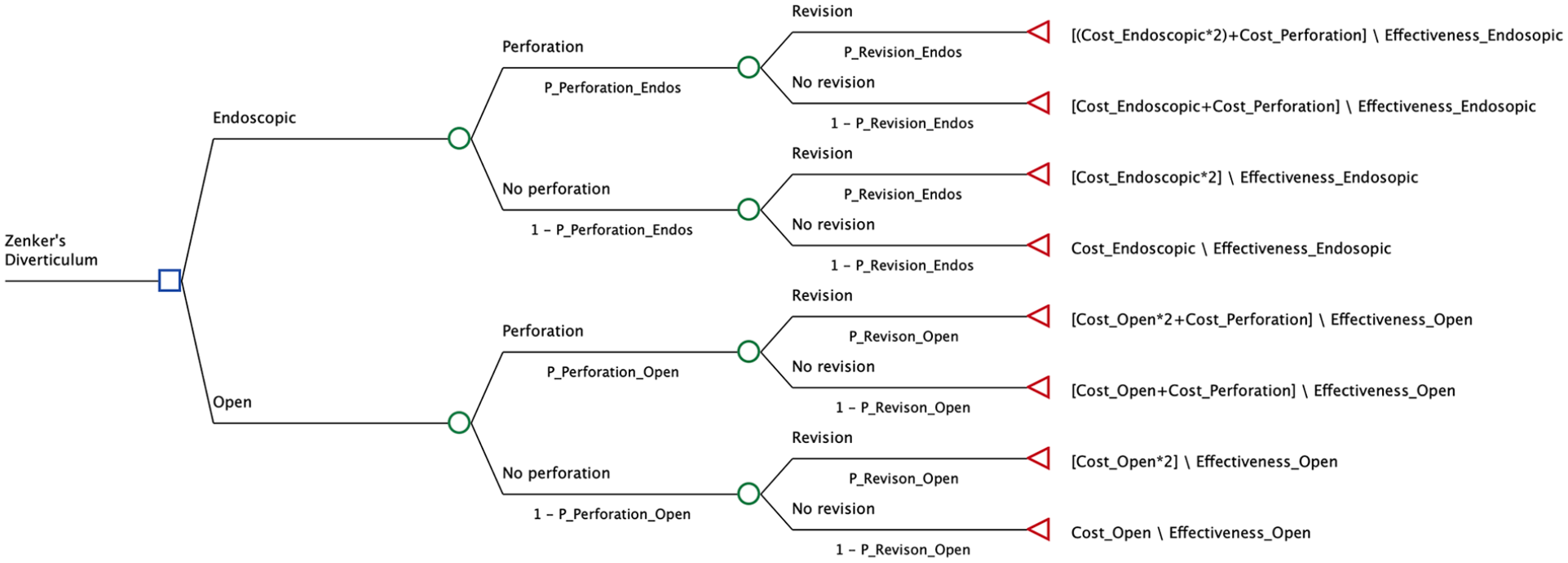
Decision tree model simulation.
Costs, Effectiveness, and ICER of Open and Endoscopic Surgery of Zenker’s Diverticulum.

Univariate Sensitivity Analysis showed that when esophageal perforation rate with endoscopic surgery was above 5% at a WTP threshold of $50 000, the open approach becomes more cost-effective with an average leak rate of 4.6%. (Figure 2)
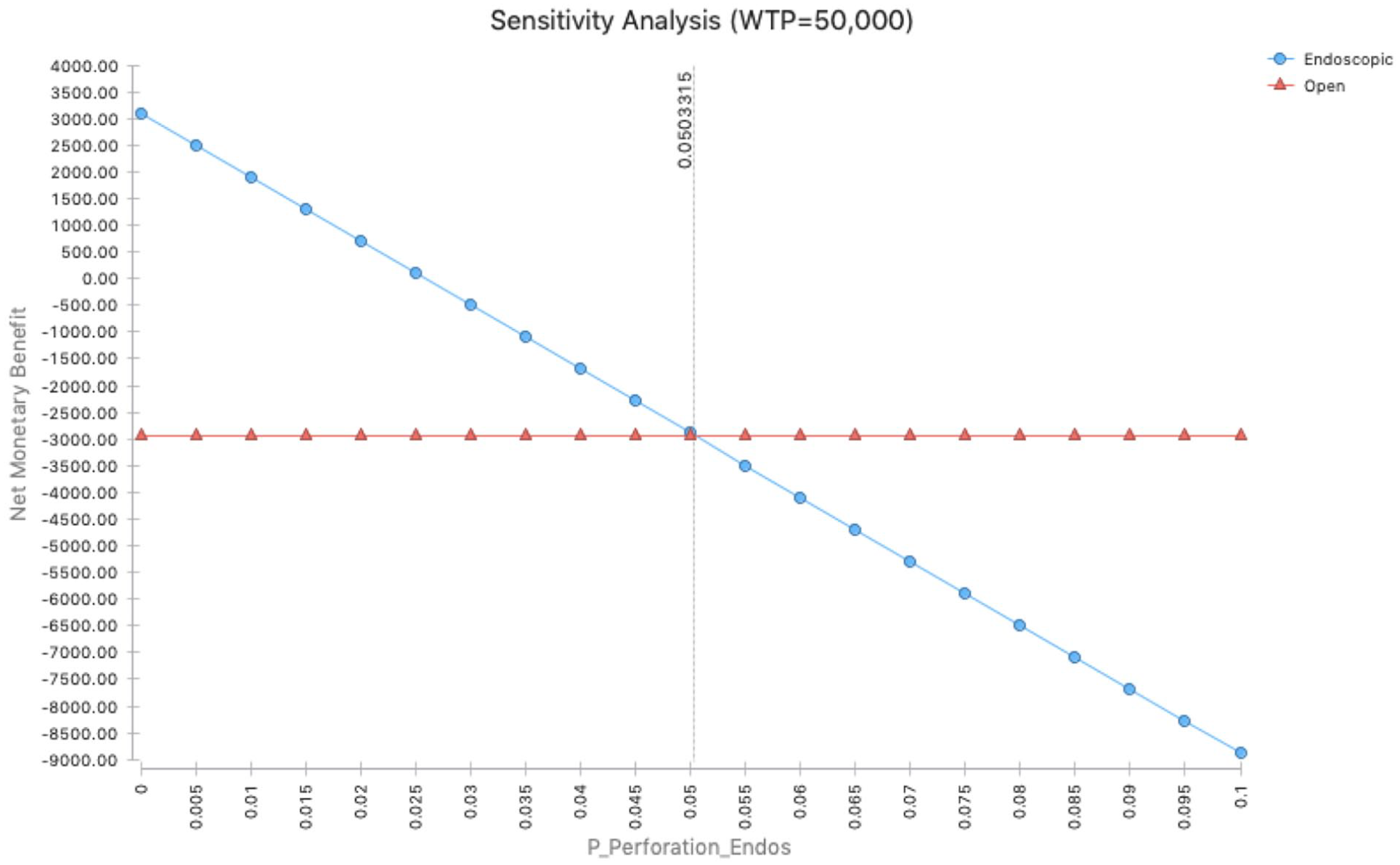
One-way sensitivity analysis of complications associated with endoscopic repair.
Next, probabilistic sensitivity analysis with Monte Carlo simulation was used to produce the cost-effectiveness acceptability curve, which showed endoscopic technique to be more cost-effective with 83.9% and 67.6% certainty at WTP of $30 000 and $50 000 (Figure 3). However, open surgery becomes a more cost-effective choice above a WTP threshold of $67 200.
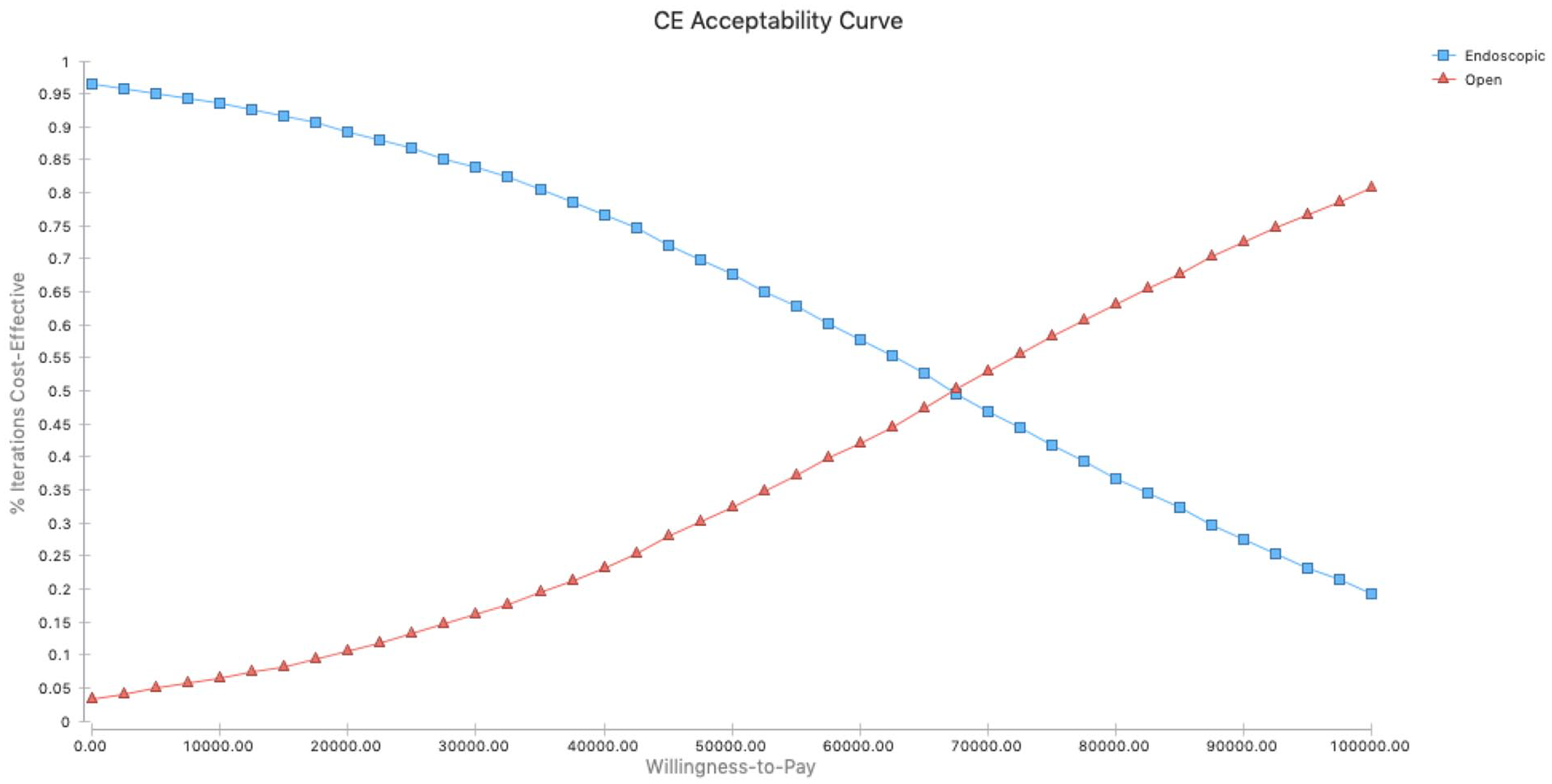
Multi variate sensitivity analysis of endoscopic versus open repair.
Discussion
Zenker’s diverticulum is the most common type of esophageal diverticulum with a reported prevalence ranging between 0.01% and 0.11%.1-3,5,6,7 While patients with small diverticula may be asymptomatic, most patients with larger diverticula present with dysphagia and accompanying regurgitation, hoarseness, or aspiration. 2 Although rare, complications if untreated may include pneumonia, peptic ulceration, vocal cord paralysis, and squamous cell carcinoma (incidence of 0.4% to 1.5%).1,2 While patients with mild symptoms can be monitored, patients with more severe symptoms require surgical correction via an open or endoscopic approach. 2
Currently, open and endoscopic surgery are 2 different approaches used to transect the septum between the diverticulum and the native esophageal lumen. Based upon the retrospective studies summarized in Tables 1 and 2, there is a 12% complication rate (with 4.6% esophageal perforation rate) and 5.3% recurrence rate with an open approach compared to a 6.0% complication rate (with 1.9% esophageal perforation rate) and 7.6% recurrence rate with an endoscopic approach. Since open surgery is associated with higher complications but fewer recurrences than endoscopic surgery, there is a limitation in the selection criteria between both surgical methods. While the decision has been largely variable and dependent on physician preference and patient age,1-7 the financial costs to the healthcare system should also be taken into account. A cost analysis study carried out by Smith et al. in 2002 reported lower hospital charges for endoscopic stapling due to shorter hospital stays (average of 1.3 days for endoscopic approach compared to 5.2 days for open approach) and time to oral diet. 6 However, no studies have directly compared the cost effectiveness between open and endoscopic surgery.
Based on the decision tree, an incremental cost-effectiveness ratio of open surgery was calculated to be $67 877, which is above the WTP threshold of $50 000 that is commonly used. In order to test for reproducibility and degree of certainty in the results, Monte Carlo Simulations were carried out, which showed endoscopic surgery as the most cost-effective method at the WTP threshold of $50 000 with 67.6% certainty.
This cost-effectiveness analysis adds an additional finding to previous studies that support endoscopic surgery as the preferred treatment for elderly patients with greater comorbidities and open surgery as the preferred treatment for patients of younger age with larger diverticula.2,4 Based on this study, the endoscopic approach is favorable to open surgery when the factors of cost, probability of esophageal perforation, cost of esophageal surgery, and long-term patient outcome on swallowing and revision rates are accounted for.
Taking all of this into consideration from an economic perspective, we recommend a decision-making process as shown in Figures 1 and 4 in which the surgeon first considers the likelihood of complications such as perforation as well as revision rates when choosing between endoscopic and open surgery for each patient. Patients in the older age groups of around 70 years are at high risk of complications from open surgery, 25 which supports endoscopic surgery as being more cost-effective at the acceptable willingness-to-pay thresholds of $30 000 and $50 000. As shown in Figure 2, the likelihood of perforation would have to be below 5% for endoscopic surgery to be more cost-effective at the willingness-to-pay threshold of $50 000.
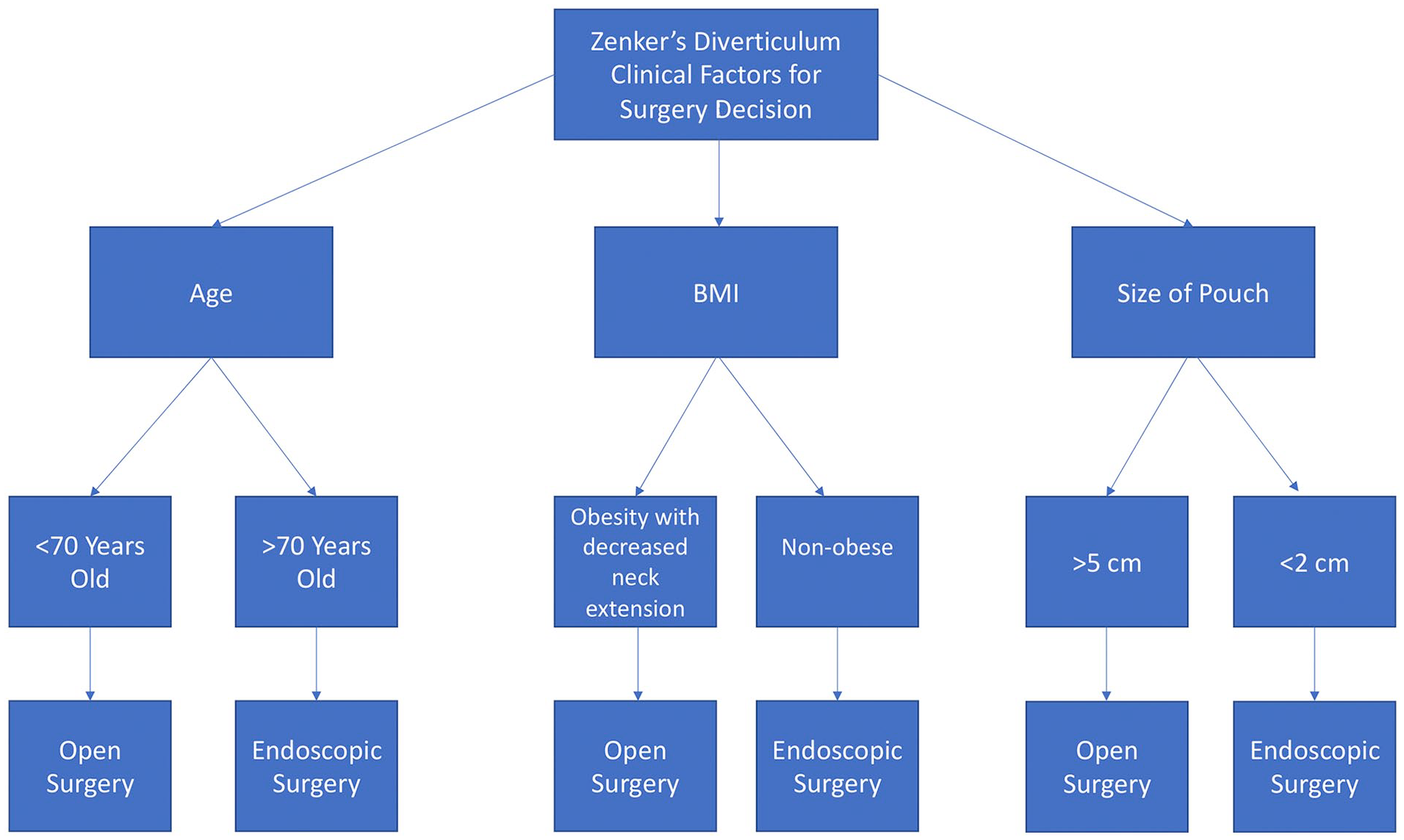
Clinical decision factors for deciding between open versus endoscopic surgery for Zenker’s diverticulum in context of cost-effectiveness.
However, the recurrence rate of Zenker’s diverticulum requiring revision surgery is higher for endoscopic surgery compared to open surgery as summarized in Table 2. As shown in Figure 3, open surgery becomes a more cost-effective option above the willingness-to-pay threshold of $67 200 when accounting for costs of further surgery revisions. As detailed in Figure 4, patients of younger age groups with additional characteristics of large diverticula, 26 higher body mass index,27,28 or difficulty with neck extension 28 who experience less success with endoscopic approach may find the open surgery to be more cost-effective at higher WTP.
Overall, endoscopic surgery is a more cost-effective approach at the WTP threshold of $30 000 and $50 000, but given the higher recurrence and revision surgeries required of endoscopic compared to open surgery, both endoscopic and open approaches are viable surgery options that should be considered on a case-by-case basis by physicians based on the degree of surgical complexity, patient comorbidities, and familiarity with the procedures.
There were several limitations of the study design. All the previous research utilized in this study were retrospective, reducing the reliability of results and conclusions. Also, Zenker’s diverticulum is a disease with higher prevalence in the elderly population. Given that the elderly population is more likely to have a greater number of comorbid conditions, results of this study may be confounded with complications due to other health problems. 7 In addition, the operation costs as determined by the CPT varied between different hospital systems. Nonetheless, we believe this economic model serves an important comparison between both surgical methods to provide patients and physicians today with greater selection criteria based on cost-effectiveness.
Conclusion
Zenker’s diverticulum is an outpouching of esophageal mucosa that can cause much discomfort to elderly patients and can lead to serious complications if left untreated. Open surgery and endoscopic surgery are 2 treatment strategies that each have their own advantages and disadvantages that can complicate the decision-making process. To our best knowledge, this study is the first to use a decision tree model to provide more direct cost-effective comparison between both open and endoscopic surgery. Overall, this economic evaluation supports endoscopic surgery as the more cost-effective strategy compared to open surgery at most common WTP thresholds.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.