
Abstract
Objective:
The main objective of this research was to evaluate the correlation between the severity of hearing loss and the facial emotional recognition as a critical part of social cognition in elderly patients.
Methods:
The prospective study was comprised of 85 individuals. The participants were divided into 3 groups. The first group consisted of 30 subjects older than 65 years with a bilateral pure-tone average mean >30 dB HL. The second group consisted of 30 subjects older than 65 years with a PTA mean ≤30 dB HL. The third group consisted of 25 healthy subjects with ages ranging between 18 and 45 years and a PTA mean ≤25 dB HL. A Facial Emotion Identification Test and a Facial Emotion Discrimination Test were administered to all groups.
Results:
Elderly subjects with hearing loss performed significantly worse than the other 2 groups on the facial emotion identification and discrimination tests (P < .05). Appealingly, they identified a positive emotion, “happiness,” more accurately in comparison to the other negative emotions.
Conclusions:
Our results suggest that increased age might be associated with decreased facial emotion identification and discrimination scores, which could be deteriorated in the presence of significant hearing loss.
Introduction
Social cognition is a process that enables people to analyze and interpret information about other people and social groups. This adaptive process may help an individual to undertake appropriate actions for consistent social interaction after generating several expectations. It is also possible for a subject to form predictions from relevant information obtained within his or her social network.1,2 These findings suggest that understanding facial perception and emotions is essential to sound social cognition status. Personal social judgments and subsequent behaviors rely heavily on this status.1,3 Hereby, humans use facial expressions to convey their emotions and understand those of others.3,4 Consequently, awareness of facial emotions strengthens interpersonal relationships and enhance psychosocial functionality and well-being. 5
The ability to recognize facial emotions, especially negative ones, was shown to be decreased with increasing age.6-8 The decreasing capacity to process the emotional signs has become a rapidly growing social problem as the number of the aging population increases worldwide. 8 Sensorineural hearing loss is one of the most common chronic conditions associated with senility. Several studies showed that this devastating disorder reduces not only the physical and psychological welfare of the individuals but also the cognitive functions, including the ones related to social cognition.9-11 Research on the social cognition ability of individuals with hearing loss was concentrated particularly on their ability to recognize vocal emotions. 5
Several studies have shown that individuals with hearing loss showed significantly decreased ability of vocal emotional recognition, suggesting that the auditor part of emotional recognition is critical in the recognition process. 5 It is also worth mentioning that a person’s vocal emotion recognition might also change their own facial emotion recognition which is an important part of social cognition perceived by others. Schirmer 12 suggested that besides a central interaction there is also a mechanistic link between facial and vocal expressions allowing that altered mouth shape might alter vocal, acoustic patterns. Conversely, the vocal expression’s nature might significantly impact the look of the face suggesting an interactive relationship between the mouth, as a resonance of the body, and vocal expression. These findings together provide a strong rational basis for our findings showing decreased facial emotion identification and discrimination scores in hearing-impaired patients. Herein, we have confirmed that healthy subjects performed significantly better identification and discrimination scores than the older individuals with hearing impairment.
Several studies have suggested that intact visual and auditory inputs are required for an effective social cognition between individuals, especially in terms of encoding and interpretation of emotional cues of other’s. 13 In this respect, one of our goals was to determine the relationship between hearing function and facial emotional awareness and test whether hearing comprehension might enhance the facial emotion identification and discrimination process. Several studies have revealed that hearing comprehension is related to facial emotions. For instance, Ambert-Dahan et al 14 have suggested that progressive deafness is strongly associated with decreased emotional reactivity to visual facial expressions. These findings were confirmed in children showing decreased facial emotional recognition scores compared to healthy populations which could not be reversed with a cochlear implant.15,16
It can also be hypothesized that individuals with impaired hearing could compensate their deficiency by focusing on lip-reading rather than on emotional cues from a person’s eye, which can further deteriorate the impaired facial recognition.14,17
In this connection, several studies indicated that various neuropsychiatric diseases and neurodegenerative disorders are related to diminished social cognition associated with critical neuropathological changes affecting brain network connections. 13
In rare studies evaluating the role of hearing loss on social functioning, hearing deterioration affected social functioning differently in age groups.10,18 However, although these studies found a meaningful association between socializing and decreased hearing, these studies did not evaluate specific cognitive correlates of social functioning. Hence a direct relationship between social isolation and cognition has not been shown. A recent study reported a significant association between hearing loss and poor social functioning 19 which prompted us to investigate the role of facial emotion identification and discrimination on social cognition. Previous studies also pointed out a meaningful relationship between hearing loss and socializing, which in turn could lead to some variations in specific age groups.10,18,19 Our rationale was to test whether older age with or without hearing loss might show significant differences in terms of facial emotion discrimination and identification scores compared to younger individuals.
Material and Methods
The prospective study comprised 85 individuals admitted to the outpatient clinic of the otorhinolaryngology department of a tertiary center between November 2019 and February 2020. We recruited individuals including healthy and older subjects with or without hearing impairment who were admitted for a health check-up. The duration of hearing impairment was determined as at least 1 year. At the beginning of the study no individuals suffered from cognitive problems which was confirmed with MMSE scores >24.
We categorized patients into 3 groups: Group A consisted of 30 patients older than 65 years old with a bilateral pure-tone average (PTA) mean of 0.5, 1, 2, and 4 kHz >30 dB HL. Group B consisted of 30 patients older than 65 years old with a PTA mean ≤30 dB HL. Group C consisted of 25 patients aged 18 to 45 years with a PTA mean ≤25 dB HL. Detailed medical histories were obtained from all participants. They also underwent a complete otological and audiological examination as well as a standard audiometric analysis by using a clinical audiometer device in sound-proof booths (AC40, Interacoustics, Middelfart, Denmark).
Only patients with normal facial functions were included in this study, so there were no defects or sequelae that would prevent them from making facial expressions that might affect their facial emotion identification and discrimination scores.
Specifically, they were literate, able to communicate with the researcher, and made sure that those with presbyopia wore their glasses while looking at the screen. Those who had visual difficulty that could affect the visualization of emotions with facial expression were excluded.
Shortly, the exclusion criteria were determined as illiteracy and an age of younger than 18. Written informed consent was obtained from the participants. The study was approved by the Ethical Committee (KAEK 2020/178) and performed in accordance with the recent version of the Helsinki Declaration. In testing the cognitive parameters, we have also included critical demographic parameters that would affect the cognitive functioning. In a similar vein, education level is an important factor that determines the cognitive reserve and plays a critical role in the development of cognitive impairment and dementia.20-23 In an effort to eliminate possible confounding factors, we specifically evaluated the presence of hypertension and diabetes and the educational levels in each patient group
Validated Turkish versions of the Facial Emotion Identification Test (FEIT) and the Facial Emotion Discrimination Test (FEDT) were used to evaluate the facial emotion identification and discrimination abilities of the participants.24,25
FEIT was comprised of a slide presentation of 19 black-and-white facial photographs (9 females and 10 males) that showed 6 main emotions (happiness, sadness, anger, surprise, fear, and shame). This slide presentation displayed the photos for 15 seconds with 10-second intervals between them. Participants were given a 19-question response form and they were asked to choose the emotion portrayed in the photographs. They received one point for a correct answer and zero point for a wrong one. The highest obtainable score was 19.
FEDT consisted of 30 pairs of black-and-white facial photographs (15 pairs of females and 15 pairs of males) showing either identical or different emotions, including the 6 main ones. The paired photos were also presented described above and participants were asked to mark whether the emotions in each photo were identical. They received one point for the correct answer and zero point for the wrong one. The highest obtainable score was 30.
Statistical Analysis
Using the G-POWER program with 0.35 effect size, 80% power, and 0.05 margin of error based on the percentage measurement values for the methods to be studied, the total sample size found was n = 84. Statistical analysis was done using the Statistical Package for the Social Sciences, version 21.0 (SPSS Inc., Chicago, IL). Descriptive analyses were presented as means ± standard deviations. The χ² test was used for categorical variables expressed as observation counts and percentages. The Mann-Whitney U tests were used to analyze the variables. Correlation of FEIT and FEDT with age, gender, and education levels were assessed using Spearman’s rank correlation analysis. Multivariate analysis was used to determine variables affecting FEIT and FEDT. A 2-sided P value of <.05 was considered significant.
Results
Among the 85 subjects included in the present study (Group A, n = 30; Group B, n = 30; Group C, n = 25) 54 of the participants were females, and 31 were males. The mean age of the female subjects was 59.12 ± 17.05 years (range 20-85 years) and the mean age of the male subjects was 57.48 ± 18.18 years (range 20-80 years). Demographic characteristics, mean hearing thresholds, the speech discrimination scores, and the clinical features of the subjects are presented in Table 1. When comparing the average number of correct answers we observed that FEIT and FEDT scores of older individuals with mild-moderate hearing loss (Group A) were significantly lower than the older individuals with PTA ≤30 dB HL (Group B) and the younger subjects (Group C) (Table 2 and Figure 1). All 3 groups were different for FEIT and older patients with and without moderate hearing loss, consecutively, were different than younger patients on the FEDT.
Demographic Characteristics and the Clinical Features of the Subjects.
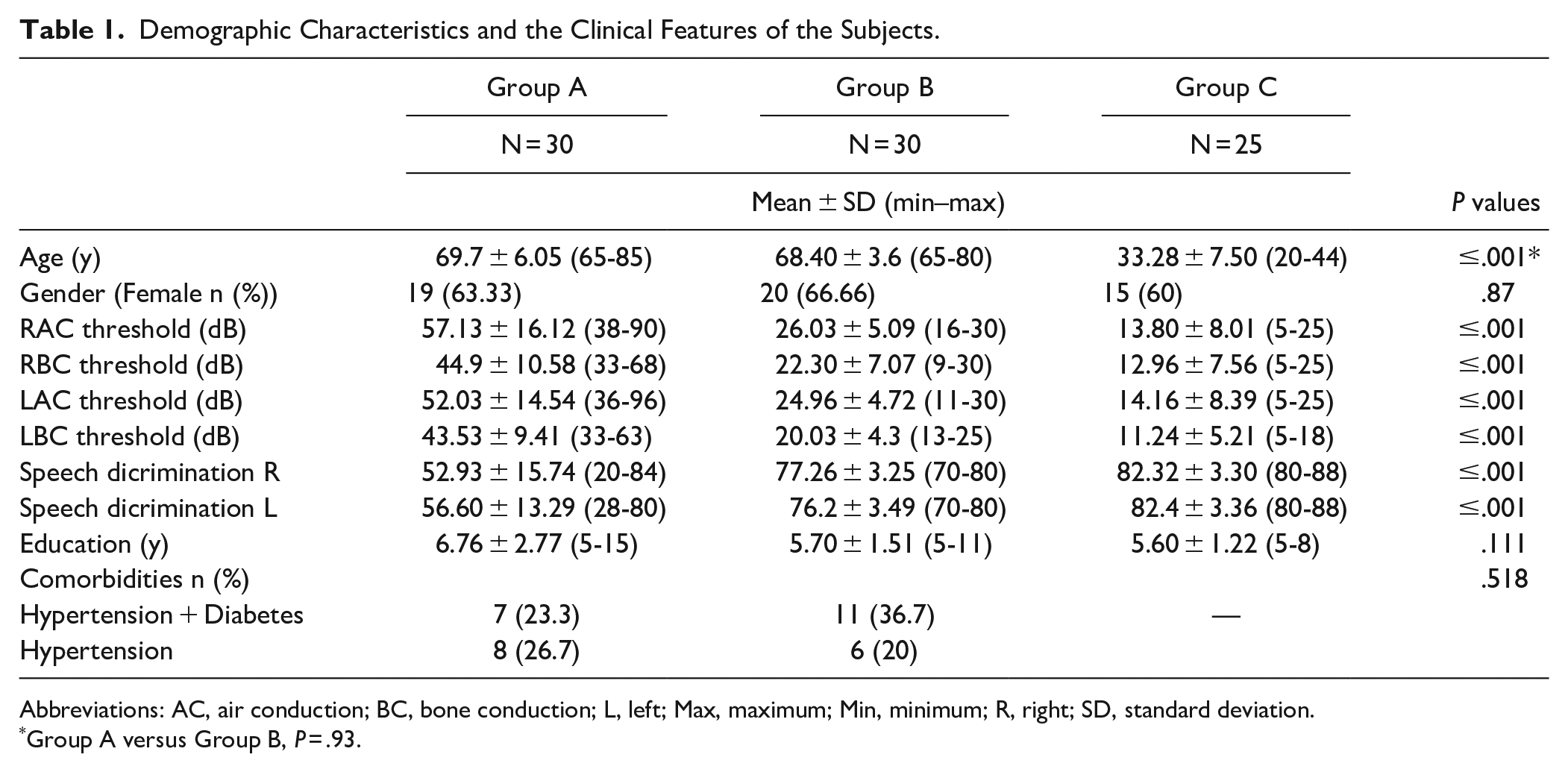
Abbreviations: AC, air conduction; BC, bone conduction; L, left; Max, maximum; Min, minimum; R, right; SD, standard deviation.
Group A versus Group B, P = .93.
FEIT and FEDT Scores of Groups.
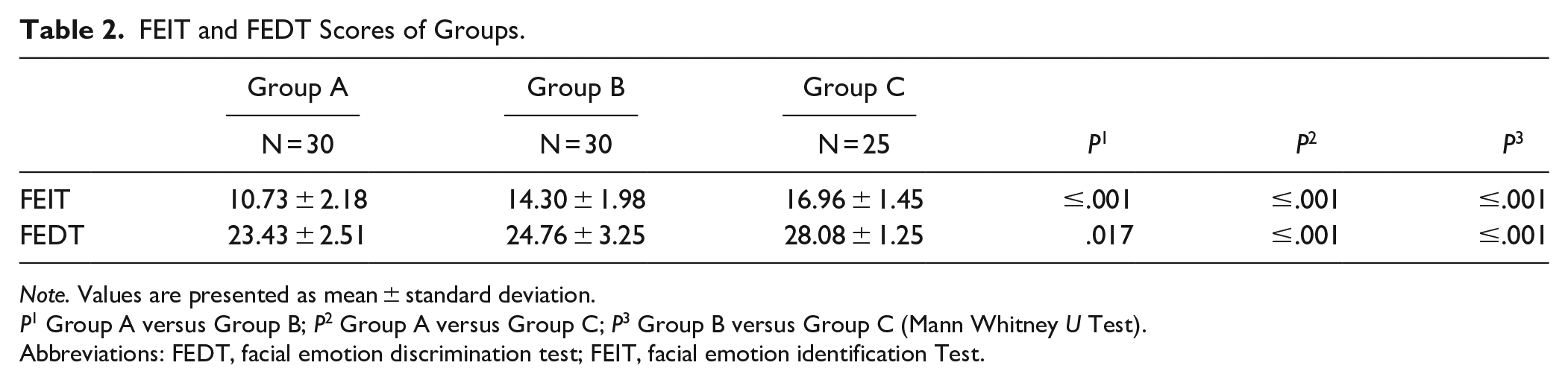
Note. Values are presented as mean ± standard deviation.
P1 Group A versus Group B; P2 Group A versus Group C; P3 Group B versus Group C (Mann Whitney U Test).
Abbreviations: FEDT, facial emotion discrimination test; FEIT, facial emotion identification Test.
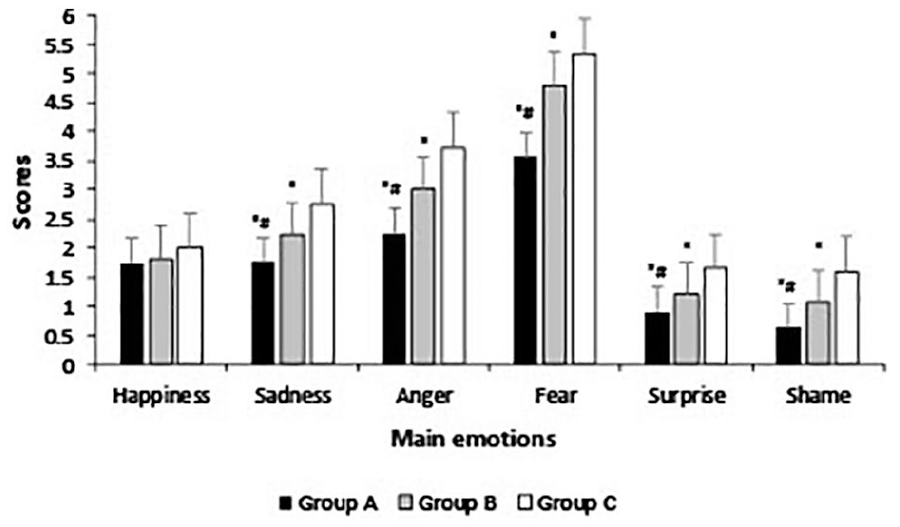
Main emotion scores of the groups.
In evaluating the emotion-specific components of the FEIT, we found that Group A showed statistically lower scores than the Group B for all emotions except “happiness” (happiness: P = .351; sadness: P = .044; anger: P = .028; fear: P = .000; surprise: P = .044; shame: P = .023). We also observed that both groups (A and B) achieved lower recognition scores for all emotions except “happiness” when compared to the Group C. (Group A [happiness: P = .077; sadness: P = .000; anger: P = .00; fear: P = .000; surprise: P = .000; shame: P = .000] and Group B [happiness: P = .341; sadness: P = .007; anger: P = .02; fear: P = .008; surprise: P = .012; shame: P = .006]) (Figure 1). We found a significant inverse correlation between the hearing threshold levels and FEIT and FEDT scores (r = −.78, P = .000; r = −.59, P = .000), as well as the age and FEIT and FEDT scores (r = −.57, P = .000; r = −.63, P = .000). A statistically significant positive correlation was also found between mean FEIT and FEDT scores and speech discrimination scores (r = .73, P = .000; r = .58, P = .000) while education level and gender were not significantly correlated with the FEIT and FEDT scores (P > .005).
In the linear regression analysis done to determine the effect of independent variables on FEIT and FEDT, there was a negative relationship with age (P < .001) and PTA (P < .001), and a positively significant relationship with speech discrimination scores (P < .001). No statistically significant relationship was found on the effects of education, MMSE test levels, and comorbidity (respectively P = .628, P = .757, P = .280, P = .269) on the FEIT and FEDT scores. The most effective factors on FEIT were determined as age (β = −.24, P < .001), PTA (β = −.48, P < .001) and speech discrimination scores (β = .23, P = .02) while the most significant factors affecting that FEDT scores were determined as the age (β = −.45, P < .001) and PTA (β = −.26, P = .012).
Discussion
The findings of the present study revealed that age-related changes, when accompanied by hearing loss, may lead to difficulties in facial emotion identification and discrimination. Understanding emotions through facial expressions is a form of non-verbal communication that plays an important role in interpersonal relationships. 26 The ability to recognize and react accordingly to the emotional content of others is the most important component of social cognition. A functional neural infrastructure is required to recall the emotional information.2,5 Individuals without these abilities can experience several communication drawbacks in social situations that can severely impair their social life. 5
It was shown that hearing loss in the elderly was associated with decreased cognitive functionality. 27 Social isolation resulting from the absence of auditory input and age-related neurodegenerative changes of the nervous system were proposed for the coexistence of hearing loss and cognitive decline in the elderly.28,29 Hearing loss is known to decrease the quality of sensory information reaching the cortex which in turn results in structural and functional alterations in the central auditory and cognitive systems. For instance, several neuroimaging studies revealed that hearing loss was associated with a decrease in the primary auditory cortex and temporal lobe volumes. 30 In line with this, a recent study comparing elderly individuals with and without hearing loss revealed that hearing loss was associated not only with whole-brain atrophy, but also with specific volume declines in the right superior, middle, and inferior temporal gyri. 31 These areas are also well-known for their functions in emotional information processing. 32 Moreover, cognitive decline with age were found to interfere significantly with the ability to recognize facial emotions, predominantly negative and neutral expressions rather than positive ones. 33 Although older individuals could recognize expressions of happiness as much as younger individuals could, they experienced considerable difficulties in defining the negative and neutral expressions.8,33,34 These findings are generally in accordance with a recent metanalysis, showing that recognizing specific emotions such as anger, fear, and sadness was mostly affected by age, except for “happiness.” They also proposed that factors other than the age-related difference in overall cognition status could be responsible for different emotional processing. 32 For instance, Keightley et al 35 recently showed that younger individuals showed wider patterns of neural activity in different regions of the brain and the amygdala while they were distinguishing “happy expressions” from all other expressions. However, no reliable and distinctive neural activity could be obtained in elderly patients during their efforts to discriminate different emotional responses.4,36 These findings, altogether, indicated that when it comes to identifying the emotions, age-related regional differences exist, but aging had the least effect on the process of defining “happiness.” Furthermore, different activities for negative and neutral expressions in older people may indicate that these individuals rely rather on simulating emotions observed in other people to identify those emotions and activate regions that are more prone to the aging process. 37 Nevertheless, it is difficult to explain why “happiness” was the only preserved emotional expression throughout the groups. One plausible explanation could be that the elderly may have learned better to control positive emotions over negative ones than younger individuals with activating specific brain regions which change little with age, such as, ventromedial prefrontal cortex, lingual gyrus, and dorsal anterior cingulate gyrus. 38
Apart from hearing loss, there are critical studies suggesting that the central component of auditory processing is significantly affected in elderly patients.39-42 For instance, electrophysiological evaluation of elderly individuals with and without hearing loss showed that older adults’ difficulties in comprehension speech might be related to impaired temporal sensitivity in the aging of the central auditory system 43 These studies collectively indicated a strong relationship between difficulties in recognition of speech and advanced aging in the central auditory system. 42
Our finding of speech discrimination scores were found as the most influential factor on FEIT scores suggesting that there are also other regions responsible for the processing of facial emotion discrimination in addition to the separate processes for central facial emotion identification. Furthermore, advanced aging and related naming difficulties become more prominent during FEIT as FEDT does not require a central naming processing. 44 Thus, it is reasonable to assume that speech discrimination score has the most significant effect on FEIT instead of FEDT.
The findings of the present study suggest that central alterations secondary to hearing loss might be partly responsible for impaired processing of facial emotional expressions. The decrease in facial emotion identification and discrimination scores was not statistically different when male and female subjects were compared. This finding was inconsistent with the previous literature emphasizing the superiority of the female individuals at recognizing emotions, particularly the negative ones. 45
We revealed that there were several significant statistical differences between the groups. Here it is worth mentioning that decreased facial emotion discrimination and identification in older individuals are more prominent than healthy older and younger individuals. From a clinical perspective this would mean that besides the aging process, hearing loss might also contribute to the maladaptive neuroplasticity processing that might involve the cochlea and its central connections. This would suggest that older individuals with hearing loss might have more difficulties in cognition which may in turn, increase their risk for neurodegenerative diseases, such as Alzheimer disease. 46
Although it is nearly impossible to exclude confounding effects of other variables, we excluded a possible effect of impaired vision with a detailed ophthalmological examination showing intact visual functions. However, a real distinction between hearing and visual-based processing would require a dynamic functional neuroimaging. Thus, several studies indicated that visual and vocal emotions are processed in an interactive manner between specific brain structures. In other words, there are specific regions in the brain, such as, superior temporal cortex, responding both to vocal and visual emotional stimuli suggesting that the voice has an auditory face when it comes to brain network interactions.12,47
Although our data contributes to the literature in several ways, the lack of comparative groups within different age groups can be considered as the main limitation of our study. To fill this gap, we are planning to conduct further research with such comparative groups, involving facial and vocal emotion identification at varying degrees of hearing losses, in which the cognition status will also be evaluated.
Conclusion
The aging process may lead to difficulties in facial emotion recognition which significantly increases when accompanied by a hearing loss. The effects of hearing deterioration on social cognitive skills as well as the mechanisms underlying the sparing of specific emotional recognition (ie, happiness) may be the subject of future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human Rights
The study has been approved by the Ethical Committee (2020/178) and has been performed according to the ethical standards of the Helsinki Declaration.
Informed Consent
Additional informed consent was obtained from all individual participants for whom identifying information is included in this article. We declare that all authors have contributed to read and approved the final manuscript for submission.