
Abstract
Objectives:
Adenoid cystic carcinoma (ACC) is a commonly encountered salivary gland malignancy. However, it rarely occurs in the gingiva, an area generally thought to be devoid of minor salivary glands. We present a case occurring in this unusual site and review other reported cases.
Methods:
A 56 year-old male presented with a right-sided mandibular toothache for 1 year and underwent dental extraction. Due to persistent pain, follow up examination revealed a large gingival lesion. A biopsy was positive for adenoid cystic carcinoma.
Results:
The patient underwent a complete right segmental mandibulectomy and was reconstructed with a fibular osteocutaneous free flap. Three months postoperatively, during the planning for adjuvant radiation therapy, the patient developed pain in the left mandible. Imaging revealed extensive involvement of the left native mandible. Deep bone biopsies in several areas of the left mandible revealed ACC. He then underwent a complete left hemi-mandibulectomy and reconstruction with a fibular osteocutaneous free flap. Tensor fascia lata suspension slings were placed due to concern for an open mouth deformity attributable to disruption of bilateral masticator slings. He will undergo adjuvant radiation therapy. Our review of the literature revealed 50 cases of gingival ACC published since 1972. Disease recurrence and distant metastases were noted in several patients, occurring at the latest after 30 years follow-up.
Conclusions:
Given its indolent behavior, high proclivity for late recurrence and metastasis, and overall infrequency, ACC represents a pathology that requires early diagnosis and comprehensive long-term surveillance. While ACC is well described in oral cavity sites with high densities of minor salivary glands, it is not commonly seen in the gingiva. As such, gingival ACC may display a unique biological and/or clinical character. We offer the first literature review of this rare entity.
Keywords
Introduction
Adenoid cystic carcinoma (ACC) is an uncommon secretory gland tumor. 1 Although ACC accounts for just 1% of head and neck malignancies, it is the most common malignant tumor of the minor salivary glands. 2 It typically affects patients in the fifth and sixth decades of life, and while it may occur in the major or minor salivary glands, it most frequently occurs in the latter, commonly affecting the palate, paranasal sinuses, floor of mouth, and buccal mucosa.1,2 By some reports, <2% of oral cavity ACC occurs in the gingiva, and it remains unknown whether this unusual site confers a distinct prognosis. 3
We present a rare case of gingival ACC as well as a comprehensive literature review of all previously reported cases of gingival ACC. Our findings demonstrate the need for an aggregate analysis of this malignancy arising in this uncommon oral cavity site.
Case Report
A 56 year-old male presented with a 1 year history of dental pain and swelling that persisted after multiple teeth were extracted. Following these extractions, the patient noticed a large lesion arising in his right mandibular gingiva. The lesion was biopsied and was positive for adenoid cystic carcinoma, cribriform pattern predominant with lymphovascular invasion (Figure 1). There was radiographic evidence of cortical bone invasion. A CT scan showed a lytic lesion of the body of the right hemimandible involving the lingual and buccal cortices with tumor extension to the right floor of mouth (Figure 2). MRI showed an enhancing lesion of the right body and ramus of the mandible with direct extension along the course of the inferior alveolar nerve canal (Figure 3). Imaging of the chest revealed no evidence of pulmonary metastases.
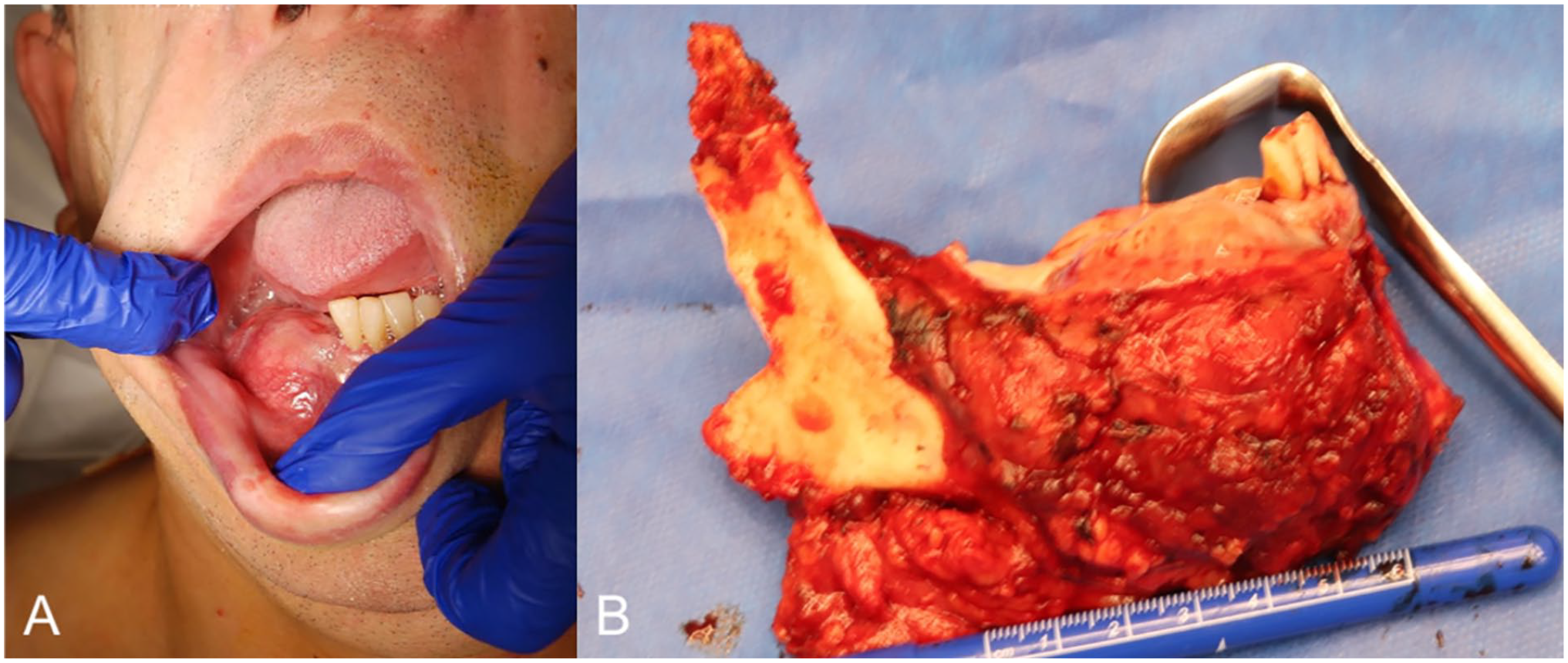
(A) Biopsy-proven adenoid cystic carcinoma of right mandibular gingiva. (B) Oromandibular resection specimen included the angle, coronoid process, and the entire body of the mandible to the midline.
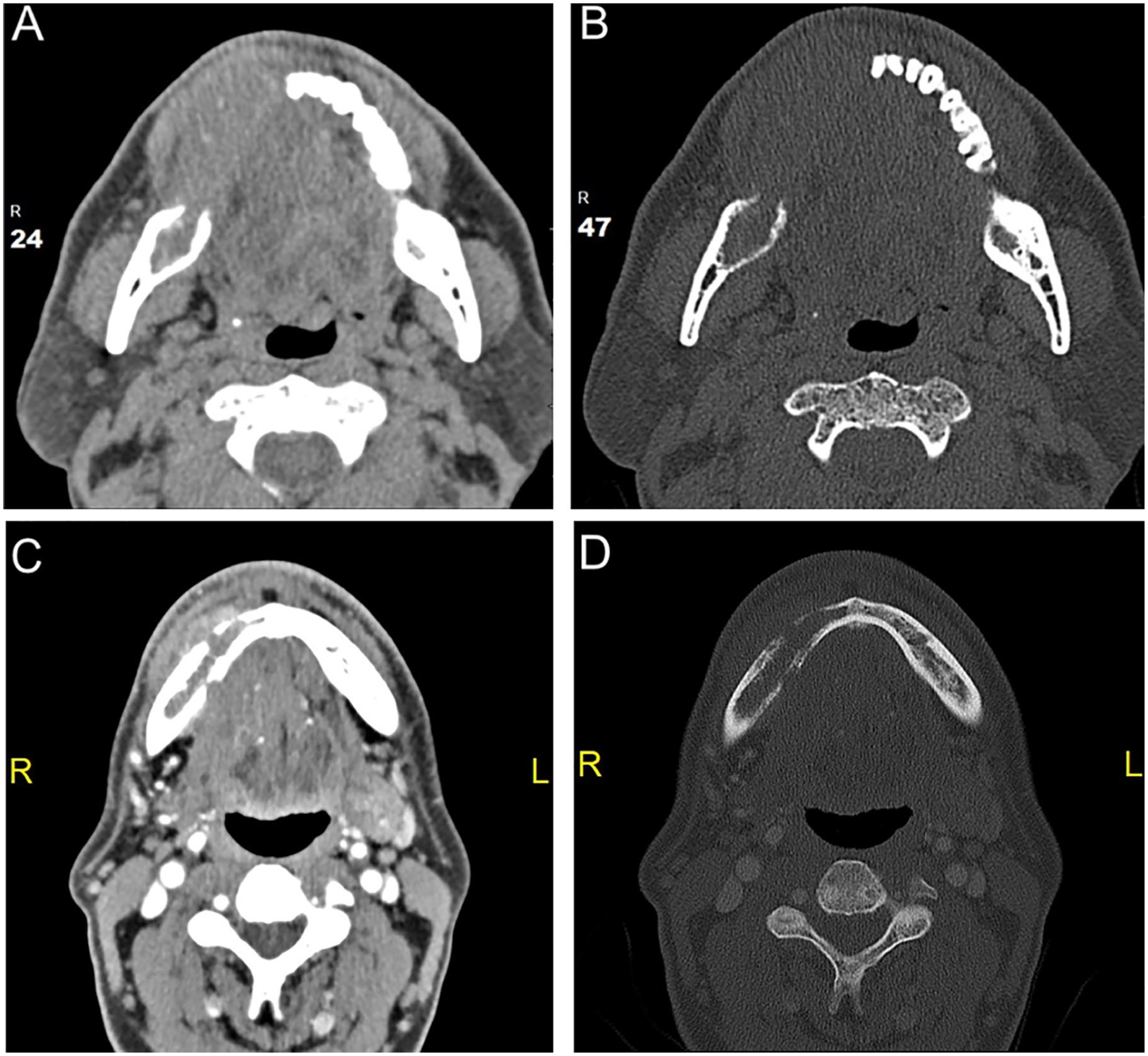
Axial CT soft tissue (A) and bone windows (B) demonstrate a soft tissue mass involving the right mandibular gingiva with extension to the gingivobuccal sulcus and erosion of the adjacent right body of the mandible. Additional axial soft tissue (C) and axial bone window (D) images demonstrate asymmetric soft tissue prominence and enhancement of the right gingivobuccal sulcus with lytic lesion of the body of the hemimandible. Erosive changes involve the trabecular and cortical surface of the mandible.
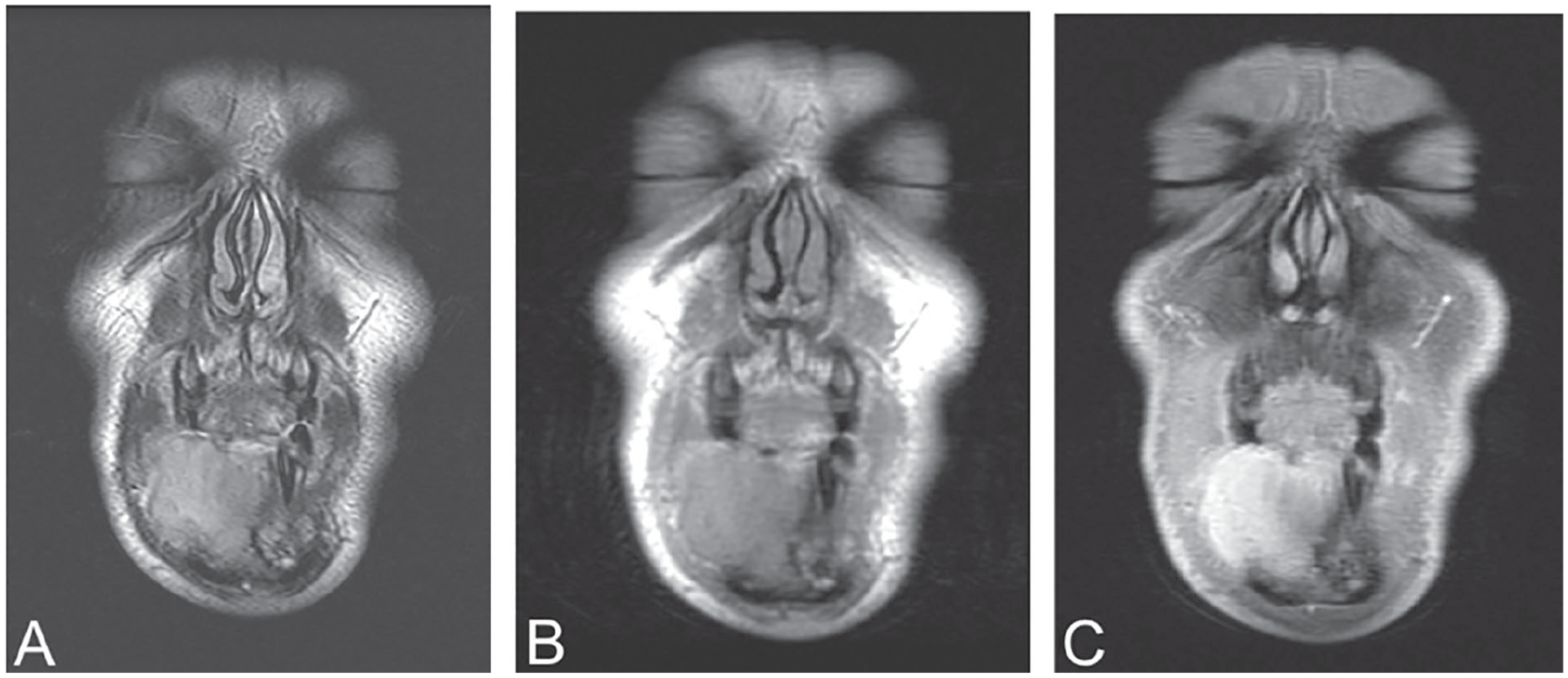
Coronal T1 weighted (A), T2 weighted (B), and postcontrast (C) images demonstrate a lesion involving the gingiva of the lower alveolar ridge with extension to the gingivobuccal sulcus and involvement of the adjacent right body of the mandible. This lesion is hypointense on T1, hyperintense on T2 and shows enhancement on administration of contrast.
The patient underwent a right segmental mandibulectomy, ipsilateral selective neck dissection and primary reconstruction with a fibular osteocutaneous free flap (Figure 1). Final pathological evaluation reported a 4.2 cm high-grade ACC of the gingiva, solid pattern, with destruction of the mandibular cortex and perineural invasion (Figure 4). Despite having clear margins on frozen section intraoperatively, the right ramus of the mandible margin was deemed positive for ACC on final pathology. A total of 25 lymph nodes were identified in the neck dissection, and no nodal metastases were identified. The final pathological stage was T4aN0M0.
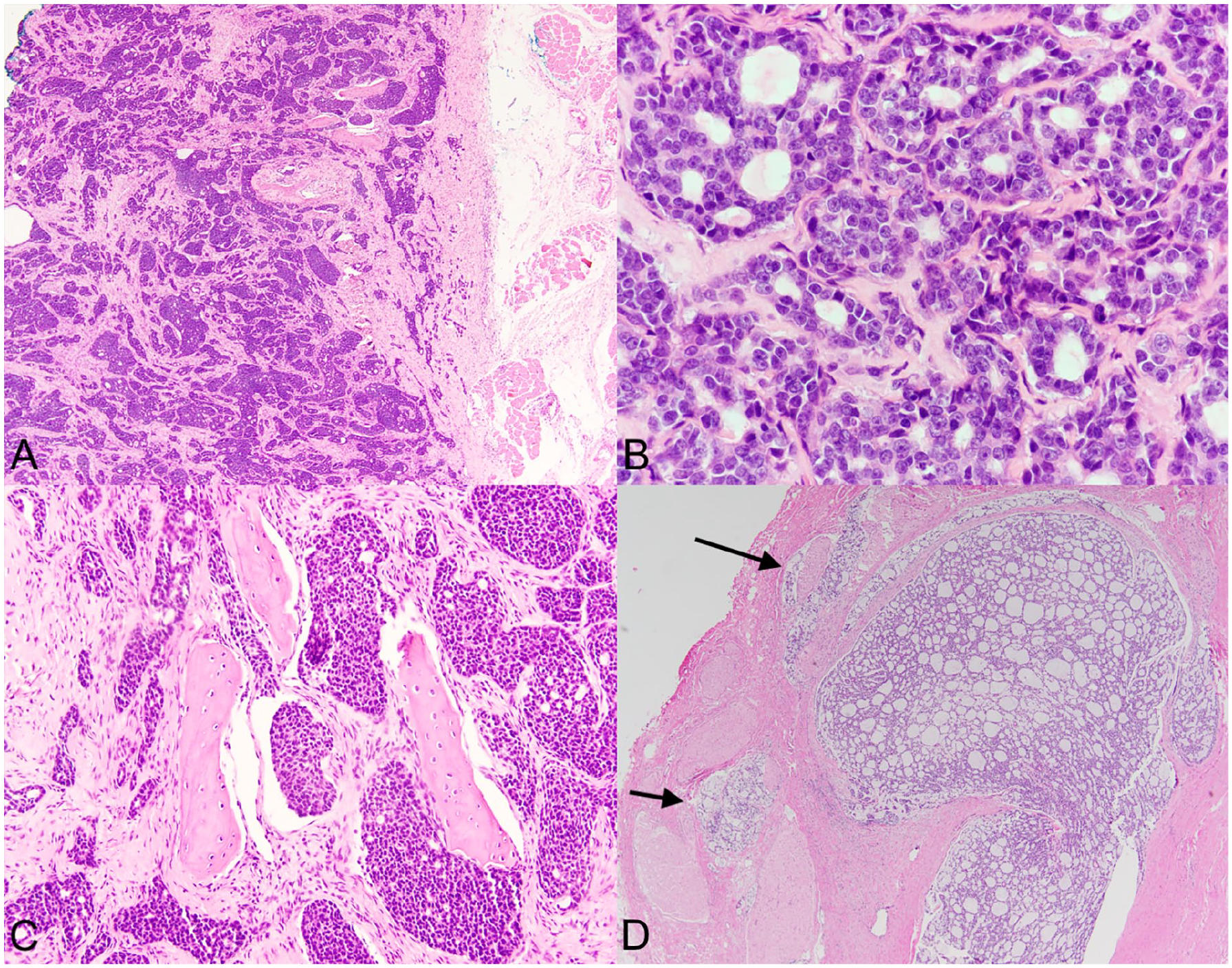
Photomicrograph of adenoid cystic carcinoma. (A) Nesting of large tumor cells in the solid pattern of adenoid cystic carcinoma with bony destruction of the mandible (H&E stain: original magnification, 40×). (B) Higher magnification tumor cells show a cribriform pattern with stromal clefting (H&E stain: original magnification, 200×). (C) The cells of adenoid cystic carcinoma have invaded the bone of the mandible with destructive growth (original magnification, 100×). (D) A characteristic feature for adenoid cystic carcinoma is invasion and encirclement of nerves (H&E stain: original magnification, 100×).
The patient tolerated the procedure well and the following month underwent a right completion mandibulectomy to address the positive bone margin aforementioned. Reconstruction was performed with a prosthetic condylar extension to the reconstruction plate. There was no tumor identified in the mandibulectomy specimen. Four osseointegrated implants as well as a condylar prosthesis were placed. The patient was scheduled to undergo adjuvant radiation therapy but treatment was delayed due to social issues.
Three months later, the patient developed left jaw pain. FDG PET/CT imaging demonstrated a hypermetabolic focus in the gingiva adjacent to the left mandibular body near the symphysis, with extension along the left inferior alveolar nerve and destruction of the mandibular body (Figure 5). MRI demonstrated extension to the proximal left ramus (Figure 6). The patient underwent an examination under anesthesia and several bone biopsies from the area of concern identified on imaging. These biopsies demonstrated ACC. The patient then underwent a total left hemi-mandibulectomy, ipsilateral selective neck dissection and reconstruction with a fibular osteocutaneous free flap. All surgical margins were clear including the proximal margins of the lingual and inferior alveolar nerves. Due to complete disruption of the masticator slings on both sides of the mandible, tensor fascia lata slings were placed to support the mandible and to help to prevent an anticipated open mouth deformity. The patient was temporarily placed in maxillomandibular fixation with a wire located at the symphysis. The patient is scheduled to undergo adjuvant radiation.

Single frontal Panorex image demonstrates new progressive osteolysis of the native body of the mandible at the medial edge of the prior segmental mandibulectomy.
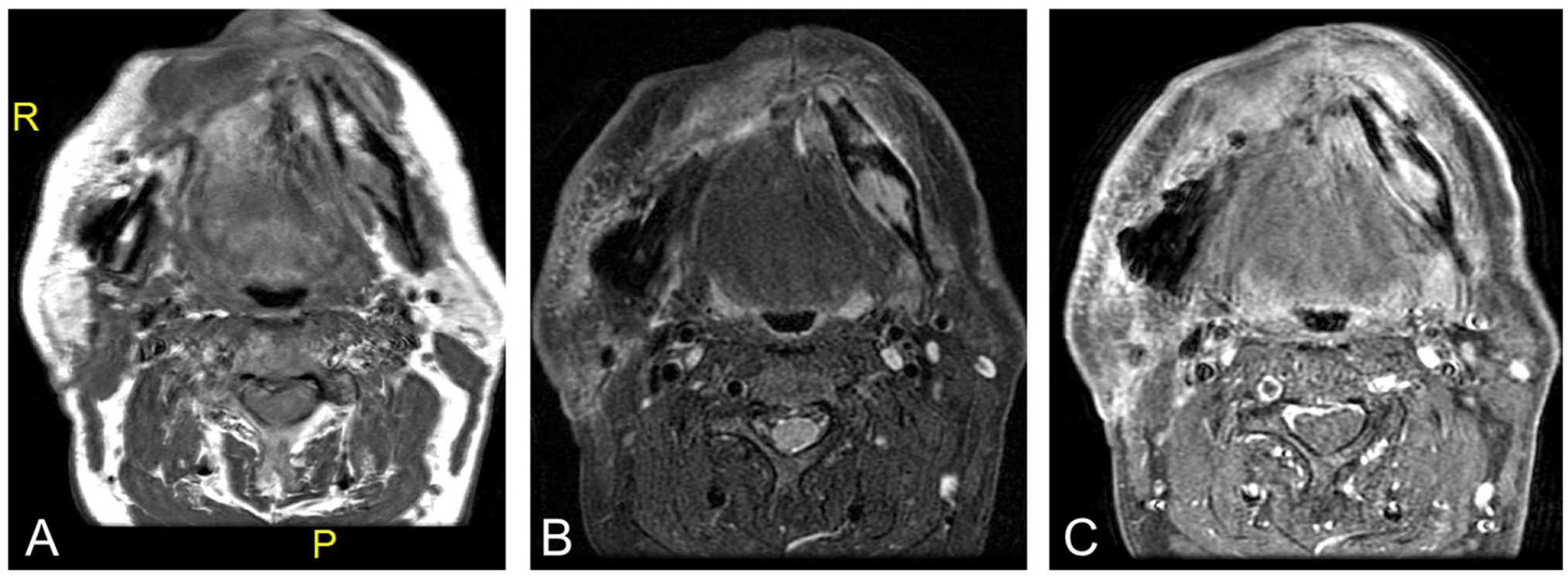
(A) Axial T1, (B) STIR, and (C) postcontrast axial FSPGR demonstrate abnormal linear signal involving the left posterior body of the mandible with extension to the proximal left ramus. There is involvement of the trabecular and the adjacent lingual cortical surface. This area is hypointense on T1, hyperintense on STIR and shows enhancement on administration of contrast.
Discussion
Adenoid cystic carcinoma (ACC) is a slow-growing secretory gland tumor typically found in the salivary glands of the head and neck.1,4 Despite its indolent growth pattern, ACC demonstrates a predilection for perineural invasion and loco-regional recurrence after treatment. 2 Given that disease-free periods of 2 or more decades prior to recurrence have been reported, it is critical to identify ACC for early diagnosis and comprehensive long-term surveillance.5,6 Distant metastases, which occur in up to 60% of patients, are mainly found in the lung and bone. Bone metastases are almost always fatal as systemic treatment options for ACC are limited.1,2,5,7,8
While ACC is uncommon in comparison with other head and neck malignancies, it is frequent among salivary gland malignancies, accounting for over 40% of those in the minor salivary glands. 7 It is well-described in the palate but rarely appears in the gingiva due to a relative scarcity of salivary glands in that location.1,9
A comprehensive PubMed and Google Scholar literature search, however, revealed 50 cases of gingival ACC published since 1972 (Table 1). Fifteen cases lacked clinical information and were excluded from further analysis.3,10-12 Among the remaining 35 cases, demographic data were reported for 10 patients, including 6 females and 4 males with an average age of 51 years (range from 27 to 65 years of age). About 7 cases described disease recurrence, 6 of which were distant, with the most common site being the lung.6,8,13 Metastasis also occurred in the brain, bone, and cervical lymph nodes.6,8,13 The earliest recurrence appeared 5 years after initial presentation, and the latest was discovered after a disease-free interval of over 30 years.6,7
Summary of Reported Cases of Gingival ACC.
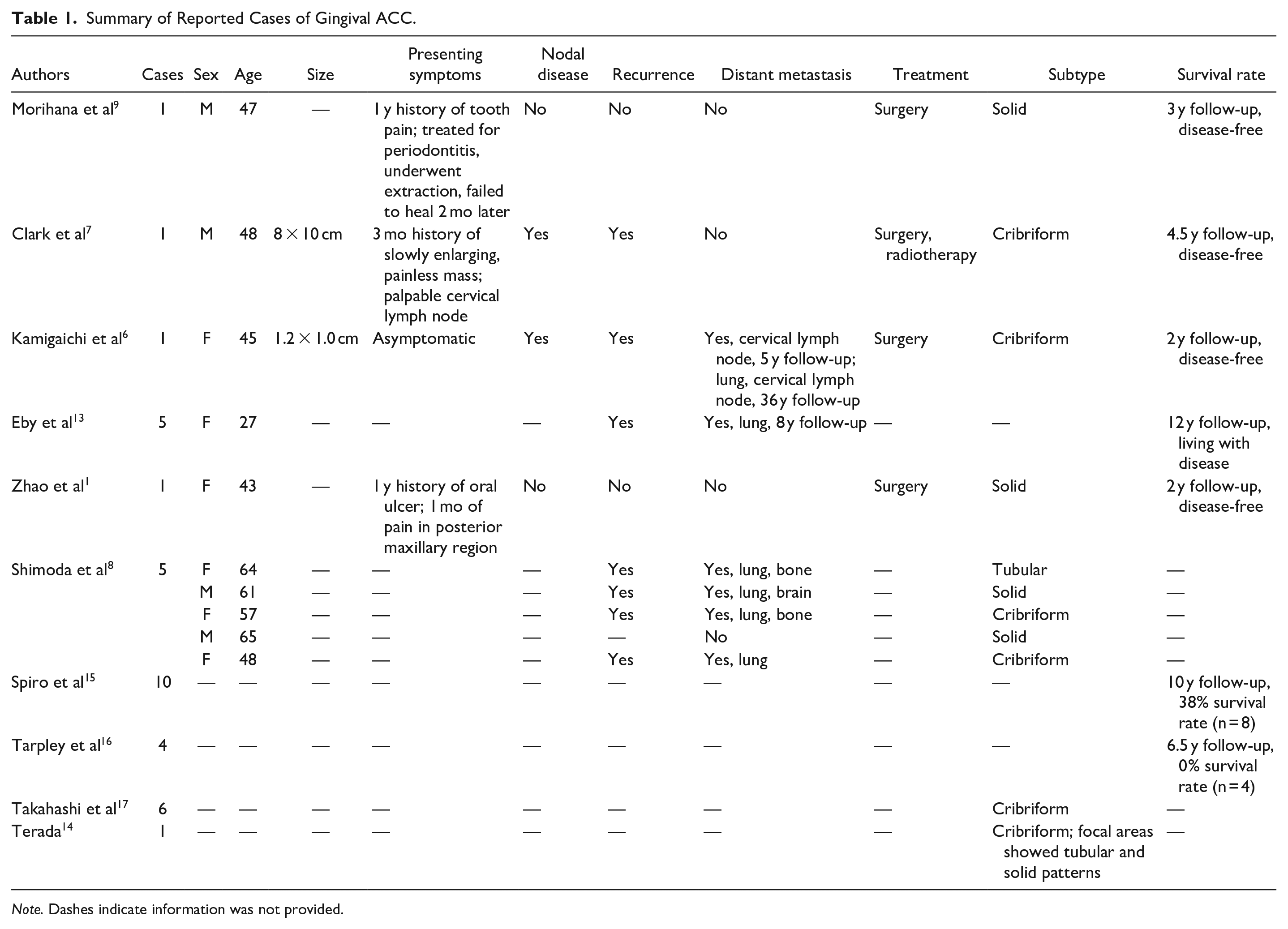
Note. Dashes indicate information was not provided.
Of the 3 histological subtypes of ACC—cribriform, solid, and tubular—cribriform is most common.7,14 The solid subtype confers the worst prognosis, recurring earlier and following a more aggressive clinical course.1,7 In our review, 10 cases of gingival ACC with pathological data included 6 cribriform, 3 solid, and 1 tubular pattern, but there was no apparent association of subtype with advanced disease or survival. Four patients were disease-free at 2, 3, and 4.5 years follow-up.1,6,7,9 One patient was alive with multiple pulmonary metastases at 12 years. 13 Two studies from the 1970s reported survival rates of 38% (n = 8) and 0% (n = 4) at 10 and 6.5 years follow-up, respectively.15,16
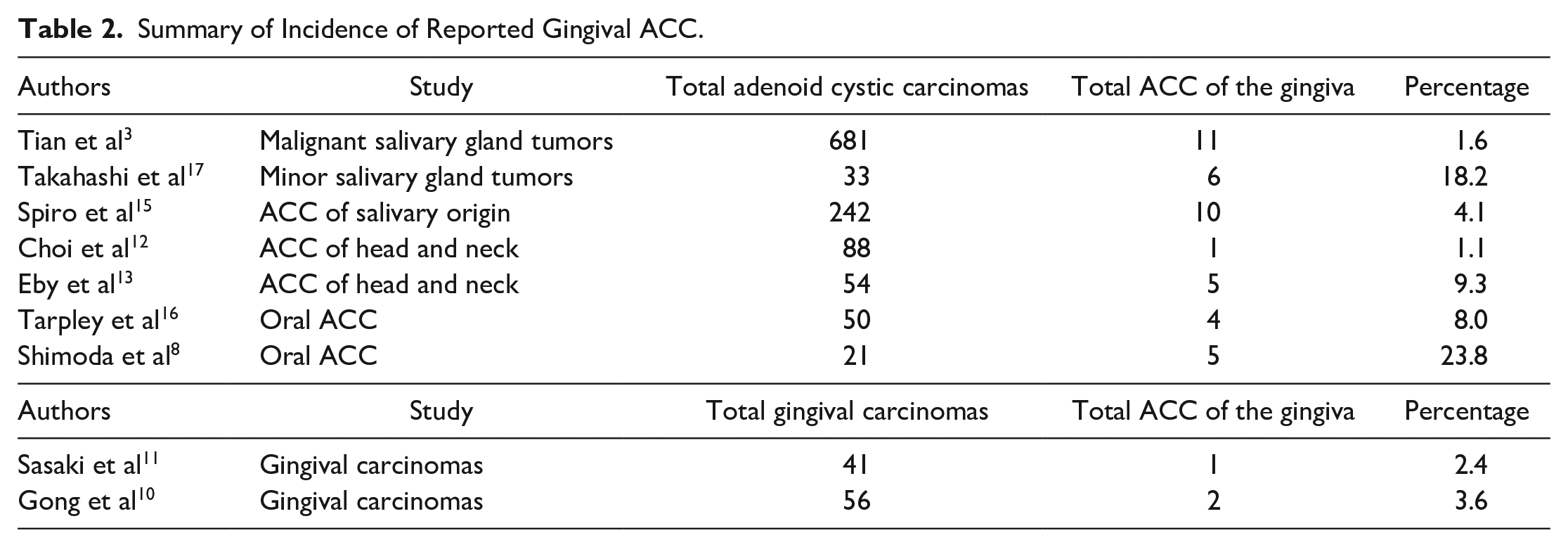
Our review showed a variable incidence of gingival ACC (Table 2). In 1 retrospective study, among 681 cases of oral ACC, only 11 cases (1.6%) occurred in the gingiva. 3 A separate study of 200 minor salivary gland tumors identified 33 cases of ACC, 6 of which were gingival (18.2%). 17 Other studies of oral ACC report between 8% and 24% of tumors occurring in the gingiva, while studies of head and neck ACC report between 1% and 9% of tumors occurring in the gingiva.8,12,13,15,16
Summary of Incidence of Reported Gingival ACC.
Our case of ACC of the gingiva highlights archetypal features of the malignancy. ACC of the gingiva typically presents, as in our case, in patients in the fifth and sixth decades of life with many months of persistent pain. Patients often have advanced disease by the time they are diagnosed, and our case similarly presented with stage T4a disease. 2 Histopathological analysis confirmed our case of ACC was solid pattern predominant, unlike the majority of cases in the literature which were cribriform pattern. Additionally, the tumor in our case demonstrated perineural invasion; both features are associated with advanced disease and worse prognosis. 2 Our patient underwent surgical treatment and will undergo adjuvant radiation therapy, which corresponds with reported treatment modalities (Table 1). Notably, several of the cases in our literature search demonstrated recurrence and/or distant metastasis, reported at 5 years follow-up or later (Table 1). It is evident that in the current case, the early appearance of adenoid cystic carcinoma in the contralateral hemimandible represented a skip lesion that eluded initial pathological detection at the anterior margin of the initial pathologic analysis. In addition, the disease was not evident on initial imaging of the mandible. The rapid growth of the disease on the contralateral side of the mandible is indicative of the potential virulent nature of this more commonly indolent disease biology. As such, our patient will undergo close monitoring and long-term surveillance following treatment.
Although ACC of the gingiva is uncommon, our literature review demonstrates its indolent behavior, high proclivity for late recurrence and metastasis, and overall infrequency. ACC of the gingiva represents a rare pathology that requires early diagnosis and comprehensive long-term surveillance. Although patients generally respond well to treatment in the short-term, it is difficult to predict their long-term outcomes. Those who develop late recurrences often have poor clinical outcomes due to the limited systemic therapies available. Further research is required to better characterize gingival ACC in order to identify whether it is biologically distinct from ACC of other sites, and if it is associated with a distinct clinical course.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.