
Abstract
Objectives:
Congenital vascular lesions commonly present in the head and neck, and most are managed conservatively. Location and rapid growth, however, may necessitate surgical intervention. Endoscopic endonasal surgery (EES) in the pediatric population has emerged as a viable option in treating sinonasal and skull base lesions. Utilizing these techniques in newborns carries unique challenges. The objective of this report is to describe the successful use of direct intralesional embolization followed by endoscopic endonasal resection of a venous malformation in a postnatal patient.
Methods:
We reviewed the case reported and reviewed the pertinent literature.
Results:
A 6-week-old infant was found to have a large right-sided sinonasal lesion confirmed as a venous malformation. Rapid growth, impending orbital compromise, and potential long-term craniofacial abnormalities demanded the need for urgent surgical intervention. Risk of bleeding was mitigated with direct intralesional embolization. Immediately afterward, the patient underwent endoscopic endonasal resection of the lesion. EES in the very young presents multiple challenges both anatomically and behaviorally. A multidisciplinary approach lead to a successful outcome.
Conclusion:
We report a case of a 6-week-old infant, the youngest reported patient to the authors’ knowledge, who successfully underwent direct intralesional embolization followed by endoscopic endonasal resection of a sinonasal vascular malformation. This report highlights the challenges of this technique in the very young and demonstrates it as a viable treatment strategy for sinonasal vascular anomalies in this population.
Keywords
Introduction
Vascular anomalies are of specific concern to otolaryngologists as 60% of these lesions in children are found in the head and neck region. 1 Venous malformations represent the second most common referral to centers for vascular anomalies. 2 Although certain syndromes are associated with venous malformations, the majority of these lesions develop sporadically, and their inception remains a continued area of research.2,3 The symptomatology of these lesions is primarily based on the location and growth rate of the malformation.
Vascular malformations generally need a multidisciplinary team to plan treatment to account for variable growth rates and potential morbidity for the specific clinical scenario. Treatment options include laser therapy, sclerotherapy, and/or surgical excision. Conservative management is typically reserved for small or asymptomatic lesions. Skin and mucosal lesions are typically treated with laser therapy which may require serial treatments. 3 When lesions are inaccessible to laser therapy, sclerotherapy is a safe and effective option of management.4,5 While less invasive management strategies are preferred due to the associated high risk of bleeding, surgical resection remains a viable and effective treatment option for select cases. In a review of pediatric sinonasal and skull base lesions, Riley et al 6 notes these lesions may require a combination of non-invasive medical, chemo/radiotherapeutic, or surgical strategies. Embolization is often considered in highly vascular head and neck tumors such as juvenile nasal angiofibromas (JNAs) and carotid body tumors, 7 and advances in surgical technique, specifically the advent of the endoscopic endonasal surgery era, have expanded indications for surgery for certain pathologies.
Endoscopic endonasal surgery in very young pediatric patients, defined as children ≤6 years old, carries unique challenges. We report a case of a 6-week-old infant who successfully underwent direct intralesional embolization with n-Butyl Cyanoacrylate (n-BCA) followed by complete endoscopic endonasal surgical resection of a sinonasal mixed venous and capillary vascular malformation. This strategy required careful consideration of the patient’s pathology, anatomy, and resources available to the clinical team. To the authors’ knowledge, this is the youngest reported patient to undergo treatment for a sinonasal vascular malformation with this technique.
Case Report
The Patient
The patient was born after an uncomplicated pregnancy via spontaneous vaginal delivery at 39 weeks. Shortly following delivery, the patient demonstrated stertor and experienced desaturations during feedings and was transferred to the Neonatal ICU (NICU). Right-sided nasal obstruction and epistaxis were noted on examination and an otolaryngology consultation was requested. Flexible endoscopy revealed a smooth violaceous mass completely filling the right nasal cavity.
Computed tomography (CT) and magnetic resonance imaging (MRI) were obtained to further characterize the lesion. Imaging revealed a large right-sided sinonasal lesion measuring 3.1 × 2.2 × 1.7 cm extending from the cribriform plate to the hard palate seen in Figure 1A. Mass effect on the nasal septum caused near complete obstruction of the left nasal passage. Operative biopsy was consistent with a mixed venous and capillary-type malformation.
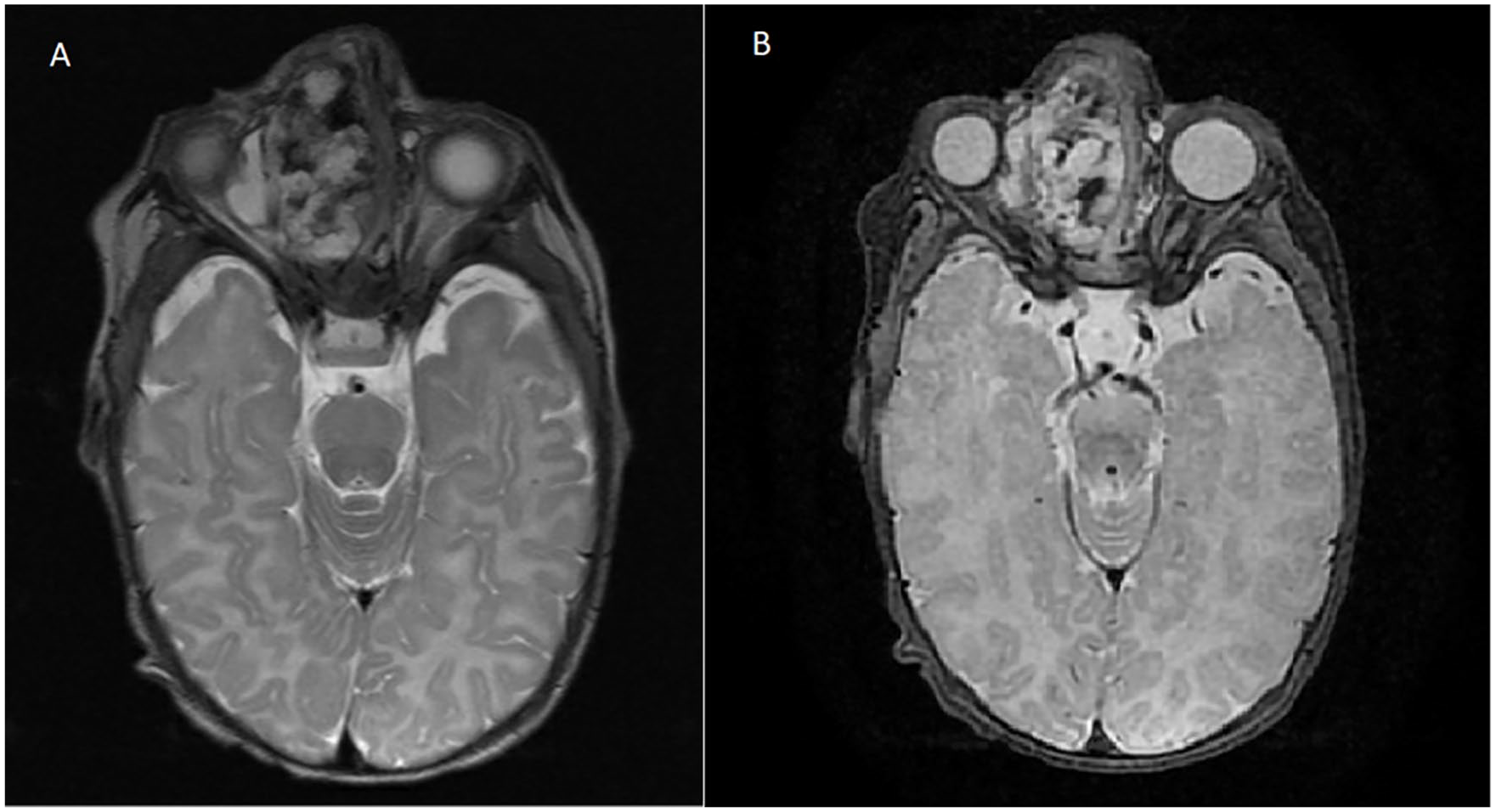
(A) T2 MRI (axial) at initial presentation demonstrating a large right sinonasal mass obstructing the right nasal cavity and nasolacrimal duct without invasion of adjacent structures. (B) T2 MRI (axial) after concern of progression demonstrating an increase in size of the mass by 5 to 6 mm in all planes. Increased fluid along the lateral aspect of the lesion was causing mass effect on the inferior rectus muscle.
Shortly after undergoing biopsy of the lesion, the patient was noted to tolerate feeds without desaturation. Multidisciplinary care planning took into consideration the tendency of vascular malformations to grow at the same rate as the patient and the difficulty of performing a complete surgical resection in a 2-week-old, close outpatient observation with deferred surgical treatment was initially favored.
Within 3 weeks of discharge, however, the patient presented to clinic and was noted to have increasing proptosis and enlargement of the right nasal ala with protrusion of the mass. Additionally, the mother had noticed intermittent bloody oozing from the right nostril. Airway symptoms were absent, and the patient gained weight appropriately. New imaging at 5 weeks of age demonstrated increased mass size with compression of the right orbit, skull base, and hard palate (Figure 1B). A significant increase in proptosis was observed in this short amount of time. Due to the pace of growth, worsening mass effect, and potential for impending orbital compromise and long-term craniofacial abnormalities, embolization and surgical resection were recommended.
Preoperative Embolization
At 6 weeks of age, the patient underwent diagnostic cerebral angiogram and direct intralesional embolization in the Radiology suite. The vascular malformation demonstrated arborization to the ophthalmic vein and cavernous sinus, but no arterial contributions were noted. An intralesional injection of 25% n-BCA/ethiodol/tantalum glue was used to directly embolize the lesion with needle guided navigation under fluoroscopy (Syngo Needle Guidance, Siemens, Forchhiem, Germany). Intraoperative 3-D Dyna-CT was used to confirm successful embolization and absence of embolic phenomenon to adjacent structures. Embolization techniques are further visualized in Figure 2.
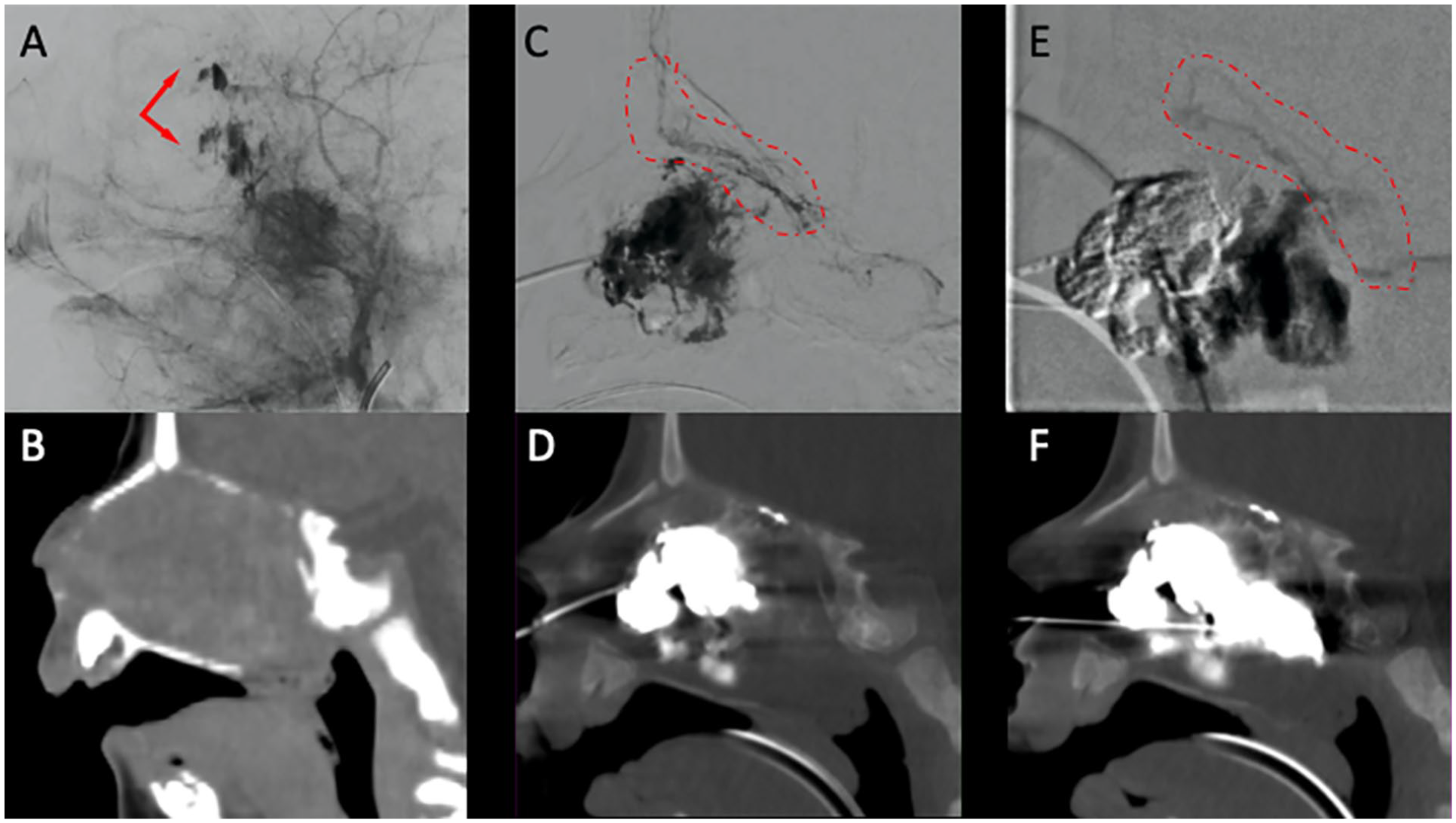
(A) Lateral external carotid artery injection during late arterial phase demonstrating venous pooling within the venous malformation as highlighted by the red arrows. (B) Pre-operative sagittal CT scan. (C) Contrast injection into the venous malformation prior to first acrylic glue injection. (D) The post embolization sagittal dyna CT scan; circled in red is the normal venous plexus without evidence of infiltration by the first acrylic glue injection. (E) Contrast injection into the remaining venous malformation prior to second glue injection, circled is the normal venous plexus which was not infiltrated with the second injection as seen in the post embolization sagittal dyna CT scan (F).
Intraoperative Details
Immediately following embolization, the patient was transported to the operating room for endoscopic endonasal resection of the mass. Stereotactic CT and MRI-guided navigation was utilized throughout the procedure (StealthStation S8, Medtronic Corporation, Minneapolis, MN, USA). The Medtronic S8 Neuronavigation unit was used to denote pertinent bony landmarks and neurovasculature. The lesion was immediately visualized grossly with gentle retraction of the ala and slight dilation of the vestibule. A 4-mm 0° rigid endoscope (Karl Storz, Tuttlingen, Germany) was used for visualization, and a combination of rigid and powered instrumentation were used to resect the mass via an endonasal, transethmoid approach. Coblation was utilized to resect the anterior portion of the mass (EVAC-70 Smith & Nephew, London, UK). The lesion was easily separated from the nasal septum, lateral nasal wall, and lamina papyracea. The lesion was noted to be tethered between the medial and lateral lamella of the cribriform plate, and dissection to the attachment point was performed. To reduce the risk of cerebrospinal fluid (CSF) leak, the lesion was debulked within its capsule at the attachment point, and a small portion of capsule was left adjacent to the anterior cranial base dura (Figure 3). Estimated blood loss was less than 20 ml and there were no intraoperative or immediate post-operative complications. The patient was transferred to the PICU and was discharged 3 days later without complications. The patient was examined 1 month post-operatively and noted to be meeting physical milestones and no longer demonstrating stertorous breathing. Moderate narrowing of the right nasal ala was observed, and the nasal cavity was dilated with urethral sounds in the operating room to improve nasal symmetry. Three months after resection, the patient’s follow-up MRI demonstrated a small focus of tissue adjacent to the cranial base suspicious for residual tumor; however, the patient remained asymptomatic. Expectant management was favored over intralesional embolization after discussion, and the patient remained asymptomatic at their 6 month follow up appointment.
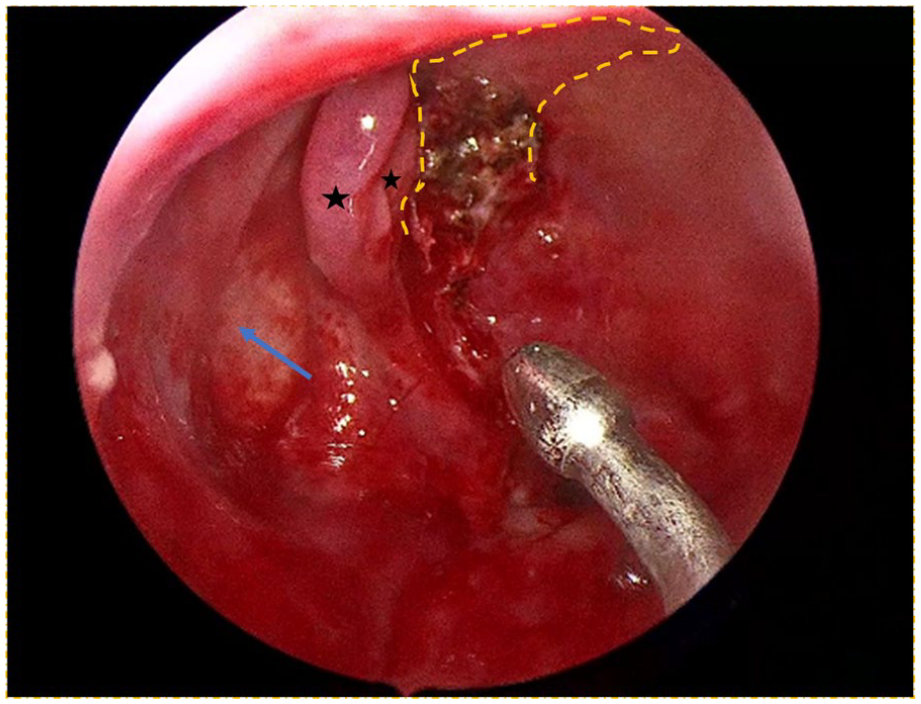
Endoscopic visualization of the post-resection cavity demonstrating the capsular attachment of the lesion to the ethmoid roof/cranial base. The lamina papyracea (blue arrow) is in close proximity to the diminutive middle/superior turbinates (black stars) and the medial cranial base (dashed orange line) due to the small size of the perinatal ethmoid cavity.
Discussion
Management of vascular malformations in the sinonasal cavity of postnatal patients is challenging due to their rarity and a paucity of management guidelines and accepted techniques. Our case represents the successful treatment of a postnatal vascular malformation using direct-intralesional embolization and endoscopic endonasal surgical resection using standard instrumentation and techniques commonly used in adults. The youngest previously reported case of a neoplasm resected with endoscopic techniques was in a 9-month-old, making our patient the youngest known patient to undergo resection using these techniques, to our knowledge.8-10
Vascular malformation resections have high risk for bleeding. A viable, well-described option for mitigating bleeding risk is preoperative embolization. Per Mingming et al 11 and Borota et al, 12 preoperative endovascular embolization prior to JNA resection improved intraoperative visualization, shortened operative time, decreased blood loss, and resulted in improved rate of gross total resection (GTR). These benefits are balanced against the risks of embolization including ischemia, edema, and hemorrhage. 7 In this case, direct intralesional embolization was chosen as sole therapy due to the lack of arterial connection and easy transnasal accessibility. Our center has previously reported our experience with direct intralesional embolization in the treatment of JNA. 13 Other investigators have suggested improved devascularization compared to transarterial embolization.14,15
Traditionally, pediatric skull-base surgical intervention often required craniofacial resection. These open approaches requiring facial incisions and osteotomies placed children at risk of damaging crucial skeletal growth centers resulting in facial asymmetry. 9 EES provides a minimally invasive alternative with less gross manipulation of vital structures. Endoscopic endonasal techniques have been used to resect vascular lesions in the orbit, nasal cavity, and intracranial cavity with excellent rates of disease control with less blood loss, fewer complications, and shorter hospital stays.16,17 Treatment of JNA has been well described and debated but tends to present in pre-teen or adolescent patients with a well-developed and pneumatized sinonasal cavity. The benefits of the endoscopic endonasal approach in neonatal patients can be surmised, but detailed reports and descriptions of techniques to utilize are lacking in the published literature.
Our patient’s lesion was limited to the sinonasal cavity without known invasion of adjacent structures and appeared completely accessible via an endoscopic transethmoid approach. As mentioned by London et al, 8 endoscopic sinonasal and skull base surgery in the very young has a unique set of challenges including limited sphenoid pneumatization, small nasal cavities, and behavioral challenges regarding ability to understand and implement instructions to not Valsalva. Chivukula et al 9 reports success in addressing these challenges in similar cases by incorporating a multidisciplinary team and stereotactic image-guided navigation. Our team included a rhinologist and neurosurgeon with significant experience performing endoscopic endonasal anterior cranial base surgery, a neurovascular interventionalist, and a pediatric otolaryngologist with increased familiarity of the patient demographic and involvement with the institution’s vascular anomalies team. Additionally, image-guided navigation was an integral tool deployed in this case.
Radiofrequency ablation (coblation) techniques in vascular malformation resection have been demonstrated to be safe and effective, specifically in otologic and airway lymphatic malformation resections.18-20 Additionally, coblation has been successfully utilized in JNA resection such as the previously mentioned case at our institution. 13 As coblation continues to gain favor, our case expands on its utility as this is the first mixed venous/capillary malformation and first intranasal vascular malformation treated with coblation reported to the authors’ knowledge.
Postnatal EES has anatomical constraints limiting instrumentation choice and working space. The nasal inlet, piriform aperture, and ethmoid cavity each can restrict visualization and maneuverability of instrumentation. Our patient’s right nasal inlet diameter was 5 mm (medial to lateral) due to expansion by the mass. The standard adult rigid endoscope diameter is 4 mm providing 1 mm of clearance between the endoscope and the nasal inlet. By comparison, the left (normal) side measured 3 mm in diameter, making it difficult to accommodate the standard adult endoscope. The piriform aperture of our patient was 15 × 18 mm. London et al 21 suggests less than 15 mm warrants consideration of alternate approaches as this anatomical window may present poor visualization and instrumentation restriction. Possible options to mitigate this challenge include switching from the 4 mm to the 2.7 mm lens, use of a 4-handed, 2-surgeon approach, or use of otologic microinstruments.21,22 The ethmoid cavity measured 2.4 × 2.3 × 3.9 cm. The position of the neonatal orbit and anterior cranial fossa created a significantly smaller working environment and intraoperative navigation was useful to confirm positioning of instrumentation.
The venous malformation was successfully resected with capsule remaining over exposed dura to reduce the likelihood of intraoperative CSF leak. Given the patient’s age and size of the immature nasal septum, endonasal reconstructive techniques would have been quite difficult. 21 Given the successful embolization and benign pathology, careful surveillance was favored over complete macroscopic resection. Post-operatively, the patient required dilation of right ala stenosis with urethral sounds. Jablon and Hoffman 23 note that nasal vestibular stenosis most frequently occurs secondary to trauma or foreign body extraction. We surmise that introducing surgical instruments into the nasal cavity provides opportunity for minor trauma to the local tissue, resulting in the possibility of contraction and post-operative scar. This complication was managed without further recurrence of stenosis. A minimal lesion recurrence emphasizes the need for close follow-up to monitor for recurrence and to ensure appropriate growth and function of the sinonasal structures manipulated during our procedure.
Conclusion
In this report, we describe a treatment strategy for sinonasal vascular anomalies in very young patients utilizing direct intralesional embolization and endoscopic endonasal resection. Endoscopic endonasal surgery and embolization techniques are common interventions well-documented in adults. However, minimal literature exists on the use of both techniques in pediatrics, specifically the very young patient population. This report highlights the challenges of these techniques in this population and demonstrates the successful implementation of these interventions in a 6-week-old patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.