
Abstract
Objective:
To determine in-hospital costs associated with performing an EEA to anterior skull base pathology and to identify drivers of cost variability for patients undergoing endoscopic anterior skull base surgery.
Methods:
All endoscopic anterior skull base surgeries performed over a period from January 1st, 2015 to October 24th, 2017 were evaluated. The electronic medical record was reviewed for patient factors, tumor characteristics, and cost variables associated with each hospital stay and univariate analysis was performed using Stata software.
Results:
An EEA was associated with an average total in-hospital cost of $44 545. Compared to patients undergoing a transsphenoidal approach to pituitary tumor resection, EEA patients incurred higher in-hospital costs across all variables including a total cost increase of $15 921 (95% confidence interval $5720-26 122, P = .002). Univariate analysis of all endoscopic anterior skull base surgery patients showed a cost increase of $30 616 associated with post-operative cerebrospinal fluid (CSF) leak ($10 420-50 811, P = .004), $14 610 with post-operative diabetes insipidus (DI) ($4610-24 609, P = .004), and $11 522 with African-American patients relative to Caucasian patients ($3049-19 995, P = .008).
Conclusions:
Patients who undergo endoscopic EEA for resection of anterior skull base tumors typically incur greater in-hospital costs than patients undergoing a standard TSA. Post-operative complications such as CSF leak and DI, as well as ethnicity, are significant drivers of cost-variability.
Keywords
Introduction
The United States dedicates considerably more resources to health care relative to other developed countries despite comparatively poorer outcomes across key measures including life expectancy and infant mortality.1,2 As a result, over recent years there has been a concerted effort toward understanding the drivers of health care costs in order to provide more cost-effective services.3-5
Efforts within the United States to reign in health care spending include the passage of the Affordable Care Act (ACA) in 2010 and the Medicare Access and CHIP Reauthorization Act (MACRA) in 2015, which have dramatically altered the landscape for health care delivery and reimbursement.6-9 As a result of these and similar initiatives, there has been a shift toward value-based care with hospitals and providers carrying greater responsibility for cost-containment through measures such as Accountable Care Organizations (ACOs) and bundled payments.3,6,7,9
More recently, the emphasis on value-based care has extended from the primary care setting to increasingly influence surgical subspecialties, particularly through bundled payments, an episode-based reimbursement model, that are often based on providing a fixed reimbursement for all care associated with a given surgical procedure.7,10-12 Episode-based care initiatives, such as the implementation of a bundled payment system for tonsillectomy and adenoidectomy in Arkansas, provide opportunities for effective care at lower costs. 7 However, knowledge of the relevant costs and cost drivers for each procedure is necessary for value-based care initiatives.6,7,10
Over recent years, an expanded endonasal approach (EEA) to the anterior skull base has been more frequently employed in the resection of a variety of anterior skull base tumors requiring additional access beyond the standard transsphenoidal approach (TSA). 13 While numerous studies have investigated the cost-effectiveness of the TSA, there has been considerably less research regarding the EEA.14-24
Our study aims to quantify the component in-hospital costs of the EEA with relevant comparisons to the TSA population, as well as identify drivers of cost-variability among the pooled anterior skull base pathology population. By gaining a greater understanding of the health care costs associated with this procedure, crucial data can be provided to help enable future value-based care initiatives.
Methods
This is a retrospective review of patients undergoing endoscopic anterior skull base surgery at our institution. Institutional review board approval was obtained for this study.
Patient Population
All patients undergoing endoscopic anterior skull base surgery at a tertiary care institution from January 1st, 2015 to October 24th, 2017 were identified using a Current Procedure Terminology code search.
Patients in the TSA group underwent a standard endoscopic approach for pituitary adenoma resection, 25 whereas patients in the endoscopic EEA group underwent an extended approach to anterior skull base pathology tailored to the specific tumor location. 26 The endoscopic EEA was utilized to access pathologies located primarily in the tuberculum sellae, planum sphenoidale, and clivus as well as sellar tumors with suprasellar extension.
Data Collection
The electronic medical record was reviewed for clinical and demographic patient characteristics. Cost information for each patient was obtained through hospital records and included total cost, total direct cost, fixed direct cost, variable direct labor cost, variable direct supply cost, and fixed indirect cost for each patient’s hospital visit.
Cost Variables
Direct costs were defined as all costs accrued within a revenue-producing department (ie, nursing services, laboratory testing, medical supplies) whereas indirect costs refer to costs in other departments (ie, administration costs, facility expenses). Fixed direct costs were defined as costs that do not vary with volume (ie, supervisory labor). Variable direct labor costs (ie, nursing staff) and variable direct supply (ie, medical supplies) costs refer to labor and supply costs, respectively, that vary with volume.
Statistical Analysis
Univariate analysis for cost variables was performed using Stata software (12.0) on the pooled population of all patients undergoing either an EEA or TSA to anterior skull base pathology. Multivariate regression was not performed given sample size necessary for a meaningful analysis including the number of necessary variables. Factors included analysis included age, gender, ethnicity, insurance status, secretory tumor status, body mass index (BMI), Charlson Comorbidity Index (CCI), maximum tumor diameter, suprasellar extension, Knosp score, resection extent, presence of intra-operative CSF leak, post-operative diabetes insipidus (DI), and post-operative CSF leak. The same Neurosurgeon determined radiological features including tumor location, tumor diameter, suprasellar extension, and Knosp score. Subtotal resection was defined as a resection of greater than 90% of tumor mass but not a gross total resection, while a partial resection was defined as any resection less than a subtotal resection. Comparisons for continuous variables were made with unpaired t-tests using Prism version 9.0.2 (Graphpad Software Inc., La Jolla, CA). Statistical significance was set prospectively at P < .05.
Results
Patient Characteristics
A total of 216 patients who underwent endoscopic anterior skull base surgery during our study period with available cost data were identified and included in analysis. About 190 patients underwent a standard TSA to pituitary adenoma resection, while 26 patients underwent an EEA for anterior skull base pathology. The average age of a patient undergoing an EEA was 58.6 years compared to 52.8 years in the TSA group (P = .081). There was significantly higher percentage of male patients in the TSA group (50.5%) compared to the EEA group (19.2%, P = .003). There was no significant difference in ethnicity, insurance status, CCI, or BMI between groups. Complete patient demographics are shown in Table 1.
Patient Factors and Outcomes.
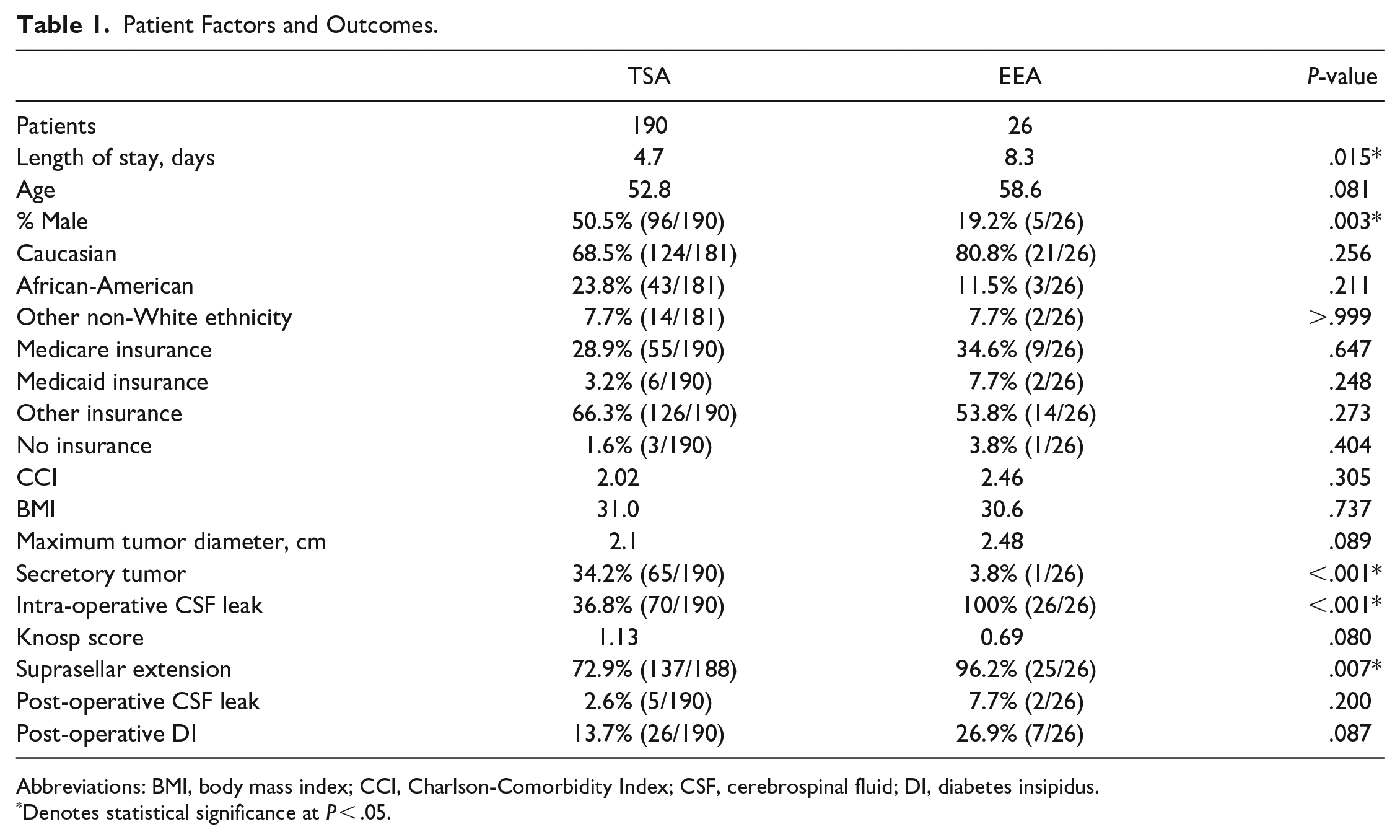
Abbreviations: BMI, body mass index; CCI, Charlson-Comorbidity Index; CSF, cerebrospinal fluid; DI, diabetes insipidus.
Denotes statistical significance at P < .05.
Clinical Features
All patients in the TSA group had pituitary adenoma on final pathology. Within the EEA group, pathology included 11 cases of meningioma, 6 craniopharyngioma, 4 Rathke’s cleft cyst, 2 chordoma, and 1 each of metastasis, pituicytoma, and a suprasellar lesion of indeterminate pathology. Twenty-five EEA patients (96.2%) had suprasellar extension and the average Knosp score was 0.69 (range 0-4). Primary tumor locations included the sella (n = 14, 53.8%), tuberculum sellae (5, 19.2%), planum sphenoidale (5, 19.2%), and clivus (2, 7.7%). Gross total resection was achieved in 13 patients (50%), with subtotal resection in 10 patients (38.5%), and partial resection in 3 patients (11.5%). Of patients undergoing an EEA, 7 (26.9%) experienced post-operative DI and 2 (7.7%) had a post-operative CSF leak. Complete radiographic and surgical characteristics of patients undergoing an EEA are shown in Table 2.
Radiographic and Surgical Characteristics of Patients Undergoing an Expanded Endonasal Approach to Anterior Skull Base Pathology.
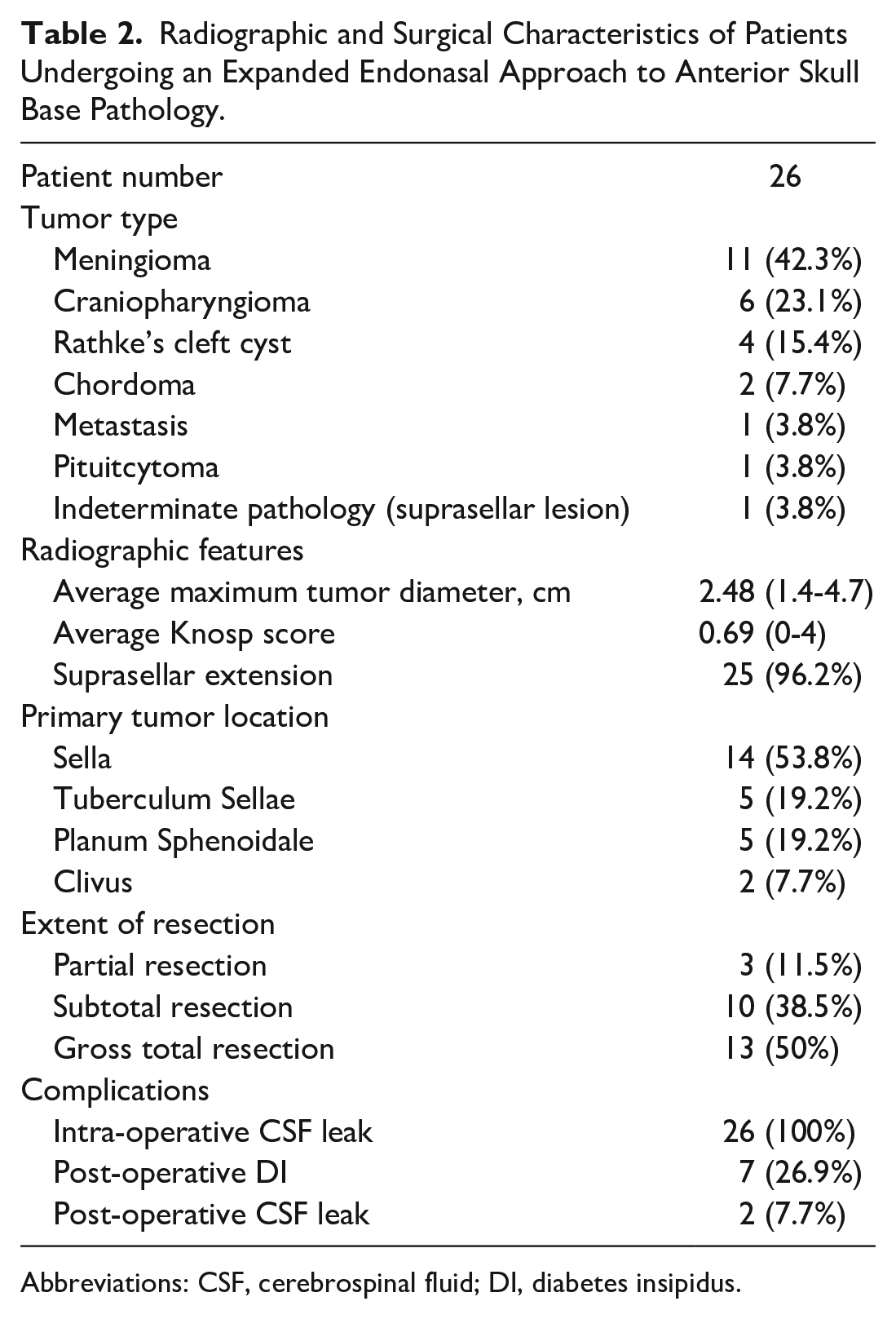
Abbreviations: CSF, cerebrospinal fluid; DI, diabetes insipidus.
Average length of stay was significantly longer for EEA patients than TSA patients (8.31 vs 4.69 days, P = .015). All patients in the EEA group had intra-operative CSF leak compared to 37.0% in the TSA group (P < .001). There was a higher rate of post-operative DI in the EEA group compared to the TSA group, although this difference was not statistically significant (26.9% vs 13.7%, P = .087). Patients with post-operative DI had a significantly longer length of stay (9.6 vs 4.3 days, P < .001). Similarly, there was a higher rate of post-operative CSF leak in the EEA group compared to the TSA group, although this finding was not statistically significant (7.7% vs 2.6%, P = .200). Patients with a post-operative CSF leak had an average length of stay of 14.1 days compared to 4.7 days for patients without a post-operative CSF leak (P < .001). African-American ethnicity was associated with a significantly increased length of stay relative to Caucasian ethnicity (7.8 vs 4.3 days, P = .003). Complete patient demographics and outcomes are shown in Table 1.
Within the EEA group, 5 patients required a return to the operating room during the post-operative stay. Two patients each underwent repair of post-operative CSF leak and optic nerve decompression. One patient returned to the operating room for evacuation of a right thigh hematoma at a tensor fascia lata graft donor site. Within the TSA group, 5 patients required a return to the operating room including 3 post-operative CSF leak repairs, 1 right thigh donor site hematoma evacuation, and 1 craniotomy after an intracranial hemorrhage.
Cost Variables
The average total in-hospital cost of a patient undergoing an EEA to anterior skull base tumor resection was $44 545, compared to $28 624 among patients undergoing TSA for pituitary adenoma resection (P = .001). On univariate analysis, an EEA was associated with an additional total cost of $15 921 (95% confidence interval $5720-26 122, P = .002) relative to a TSA. An EEA was associated with increased costs across all cost variables.
Increased post-operative CSF leak was associated with an increased total cost of $30 616 ($10 420-50 811, P = .004) while post-operative DI was associated with an increased total cost of $14 610 ($4610-24 609, P = .004) across all patients. Both post-operative CSF leak and post-operative DI were associated with significantly increased costs across all variables except variable direct supply cost. African-American ethnicity was associated with increased costs across all cost variables relative to Caucasian ethnicity, including a total increased cost of $11 522 ($3049-19 995, P = .008). Complete cost variable analysis for post-operative CSF leak, post-operative DI, and African-American Ethnicity are in Tables 3 to 5, respectively.
Post-Operative CSF Leak Costs on Univariate Regression Analysis.
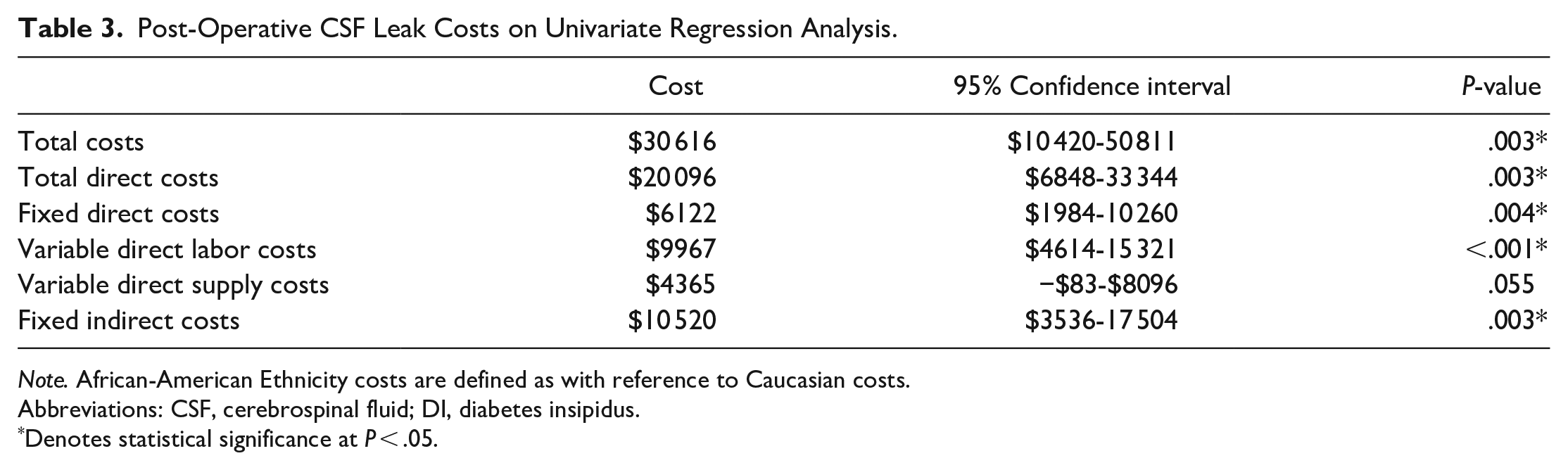
Note. African-American Ethnicity costs are defined as with reference to Caucasian costs.
Abbreviations: CSF, cerebrospinal fluid; DI, diabetes insipidus.
Denotes statistical significance at P < .05.
Post-Operative DI Leak Costs on Univariate Regression Analysis.
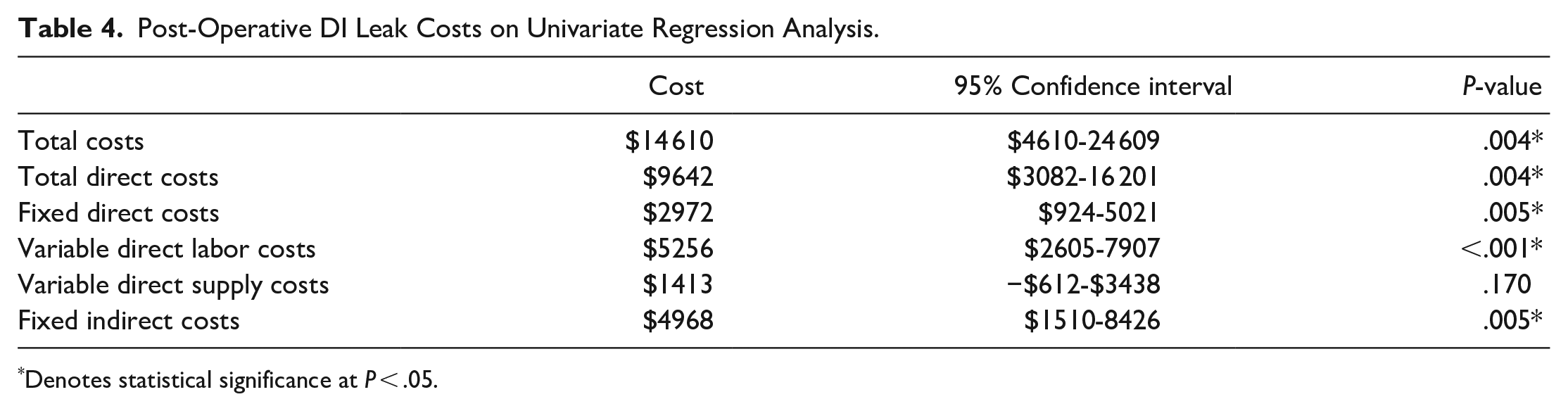
Denotes statistical significance at P < .05.
Post-Operative Costs Associated With African-American Ethnicity on Univariate Regression Analysis.
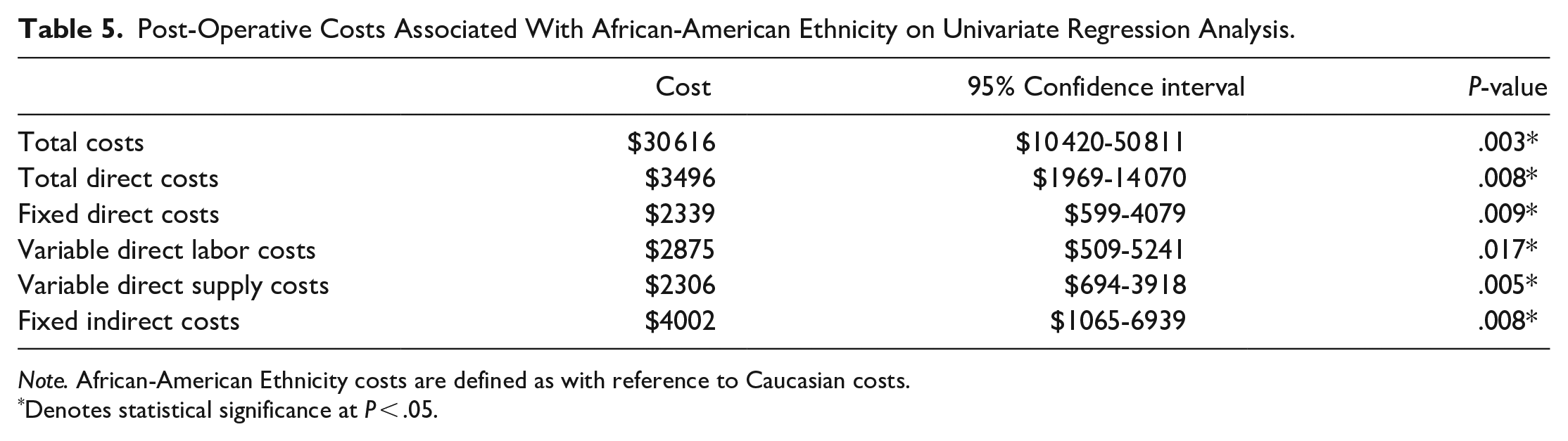
Note. African-American Ethnicity costs are defined as with reference to Caucasian costs.
Denotes statistical significance at P < .05.
There was no significant difference across all cost variables for patient age, gender, insurance status, BMI, CCI, secretory tumor status, intra-operative CSF leak, Knosp score, presence of suprasellar extension, or maximum tumor dimension.
Discussion
Over recent years, the EEA has become frequently utilized in the treatment of a variety of complex anterior skull base pathology including meningioma, craniopharyngioma, and Rathke’s cleft cysts.13,27,28 Prior research has explored the costs of the EEA for sinonasal malignancy in adults as well as endoscopic skull base surgery in the pediatric population.22,23 In addition, our previous work examined drivers of in-hospital costs among patients undergoing a standard TSA for pituitary pathology alone. 24 However, costs associated with an endoscopic EEA to anterior skull base pathology in adults have not been previously quantified and drivers of cost variability have not been explored in this population.
In our study, all endoscopic anterior skull base surgeries over a three-year period were reviewed and univariate analysis was performed using a number of patient- and clinical-factors across 6 cost variables. Our study included 190 transphenoidal approaches to pituitary adenoma resection and 26 EEAs to anterior skull base pathologies including most commonly meningioma and craniopharyngioma. The EEA crucially allowed for resection of sellar tumors with suprasellar extension as well as lesions located primarily in the tuberculum sellae, planum sphenoidale, and the clivus.
In-hospital costs were significantly greater for patients undergoing EEA across all cost-variables, including an average total cost of $44 545 for an EEA compared to $28 624 for a TSA. These increased costs reflect the more resource-intensive post-operative in-hospital care for patients undergoing EEA compared to a standard TSA.
Within our analysis, post-operative CSF leak was the single greatest driver of in-hospital costs and was associated with an increased total cost of $30 616 across both EEA and TSA patients. This result is consistent with our previous analysis on TSA patients alone, in which post-operative CSF leak was associated with a more than 2-fold in-hospital cost increase. 24 These findings likely reflect a number of factors, including operating room costs of CSF leak repair, increased length of stay, and a higher level of care.
Additionally, we identified post-operative DI as a significant driver of in-hospital costs with an increased total cost of $14 610. This finding is in contrast to our previous study of TSA patients in which post-operative DI was associated with higher costs but the analysis did not reach statistical significance. 24 The increased expenditures associated with post-operative DI are likely attributable to the more than 2-fold associated increase in length of stay as well as higher level of care. Rudmik et al 20 study analyzing costs of complications associated with pituitary surgery produced an estimate of $114.98 for the treatment of temporary post-operative DI based on a 30-day course of intranasal desmopressin sprays. However, it is clear from our analysis that the immediate post-operative costs associated with DI in the inpatient setting far overshadow the cost of medication administration in the outpatient setting. These findings suggest that effective identification and treatment of post-operative DI following EEA using standardized endocrine protocols may represent an opportunity for significant in-hospital cost savings by reducing the financial burden of inpatient DI treatment.
African-American ethnicity was associated with increased length of stay as well as increased costs across all variables relative to Caucasian ethnicity, including an increased total cost of $11 522. This finding is consistent with, but larger than magnitude to our previous study on TSA patients alone. 24 Although a Goljo et al 29 study has previously linked non-Caucasian ethnicity to post-operative complications after pituitary surgery, there was no association between ethnicity and post-operative complications in our analysis. Racial disparities in health care costs have already been identified within the endoscopic transphenoidal pituitary surgery population and likely reflect broader socioeconomic disparities.29-31 However, it is noteworthy that African-American ethnicity is associated with a total cost increase on the same order of magnitude as post-operative DI or an EEA relative to the standard TSA.
Our study is limited by its retrospective and single-institution nature, and lack of bed assignment data that may provide further insight into the variability of in-hospital costs. We were unable to perform a meaningful multivariate regression given the quantity of factors necessary coupled with the relatively small number of patients undergoing an EEA. As a result our study utilized univariate analysis, which limits our ability to discern the relative contribution of factors that may track together. Analysis of a much larger sample size of only EEA patients would be necessary to derive meaningful conclusions using multivariable analysis from the EEA population alone. Despite these limitations, we were able to compare hospital-level cost data between patients undergoing an endoscopic TSA or EEA as well as identify significant drivers of cost variability.
Value-based care initiatives such as bundled payments are increasingly utilized means of reimbursement for hospitals and providers. As these measures extend into surgical subspecialties such as Otolaryngology, understanding of the costs and drivers of cost variability for a given surgical procedure is crucial for successful implementation. This study quantifies the total and component costs for hospitalization following an EEA to anterior skull base pathology with a comparison to the standard TSA. Additionally, we performed univariate analysis of a number of clinical and demographic factors within the pooled population to highlight significant cost drivers.
In our analysis, we identified post-operative CSF leak and post-operative DI as major drivers of cost variability among patients undergoing anterior skull base surgery. Furthermore, African-American ethnicity is associated with substantial cost increases across all variables relative to Caucasian ethnicity. Examining opportunities to reduce length of stay for these populations will be a potential source of significant hospital savings. Based on our findings, reducing length of stay associated with post-operative DI represents a potential source of significant cost savings. To our knowledge, this represents the first attempt to analyze in-hospital costs associated with an EEA to anterior skull base pathology. Characterization of these costs and identification of contributing factors will guide future research and cost-savings initiatives.
Footnotes
Authors’ Note
Presented at the 20th Annual Meeting of the North American Skull Base Society, February 15 to 16, 2019 in Orlando, FL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.