
Abstract
Objectives:
To determine the influence of major head and neck procedures on readmission and complication rates following tracheostomy.
Methods:
A retrospective cohort study using the 2005 to 2017 National Surgical Quality Improvement Program (NSQIP) database. Current Procedural Terminology codes were used to identify tracheostomy patients and to define the underlying head and neck procedure. Patients under the age of 18 and with unknown pre-operative variables were excluded. Univariate and multivariable analyses were performed.
Results:
A total of 3240 tracheostomy patients undergoing major head and neck surgery were identified in NSQIP. The 30-day mortality rate was 104 (3.2%) and 258 (9.0%) patients were readmitted. 637 (19.7%) patients had an unplanned return to the operating room. There were 1606 (49.6%) non-tracheostomy specific complications, which included 850 (26.2%) medical and 1142 (35.2%) surgical complications. On multivariable analysis, we found that the underlying procedures did not impact the risk of readmission (P > .05 for all). The underlying procedure was also not associated with unplanned return to the operating room except for thyroidectomies, which had a lower risk than free tissue graft reconstruction (OR = 0.53 (95%CI 0.31, 0.88), P = .018).
Conclusion:
While almost 1 in every 2 patients had a complication following major head and neck surgery that included creation of a tracheostomy, the rate of readmission is comparatively low and is not associated with the underlying procedure. These findings should reassure head and neck surgeons that properly managed tracheostomies do not constitute a disproportionate risk of readmission.
Introduction
Tracheostomies can be placed to secure an airway either as an isolated procedure or in conjunction with another surgical procedure. 1 Placement of tracheostomy is common during major head and neck surgery. The procedure offers a stable airway that can be used in complex head and neck cancer resection with reconstruction, mechanical ventilation, and other respiratory problems. Even though tracheostomy is often a lifesaving procedure, tracheostomy placement has been demonstrated to have a median length of stay greater than 3 weeks.2,3 This represents a significant utilization of healthcare, although the average tracheostomy patient has a relatively large number of comorbid conditions that may impact outcomes.
The Agency for Healthcare Research and Quality identified tracheostomies as the fifth highest readmission rate at 23.9%, which underscores the need for reducing readmission rates and utilization of healthcare resources without compromising the quality of care. 4 While the literature has characterized risk factors for readmission and complication rates following tracheostomy for all indications, previous studies have not attempted to understand risk factors in the context of the underlying procedure if the tracheostomy is placed during major head and neck surgery.5-7 Segmental mandibulectomy reconstructed with a fibular free flap is a relatively different procedure compared to total thyroidectomy with concurrent tracheostomy in terms of risk of complications. In this way, understanding tracheostomy outcomes in relationship to the diverse array of underlying procedures is a valuable clinical question.
To provide an in-depth answer to this question, we employed the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, which is a comprehensive resource for analysis of 30-day outcomes. 8 NSQIP comprises more than 150 variables from over 700 hospitals and importantly tracks patients between hospitals to provide the most robust data. The national database also offers the ability to identify uncommon trends that only become apparent with a large multi-institutional cohort. Using the NSQIP database, we sought to understand the impact of the most common head and neck procedures on readmission rates and complications following tracheostomy.
Methods
Data Source and Selection Criteria
This study was deemed exempt by the Cleveland Clinic Institutional Review Board as the NSQIP database is de-identified. The 2005-2017 NSQIP database was queried for CPT code: 31600. Underlying procedures were defined by CPT codes as categorized in CPT Plus. 9 Other procedures were defined as any procedure with n < 10% of the total cohort. Patients with missing data, an American Society of Anesthesiology (ASA) score of 5, and age <18 were excluded as shown in Figure 1.
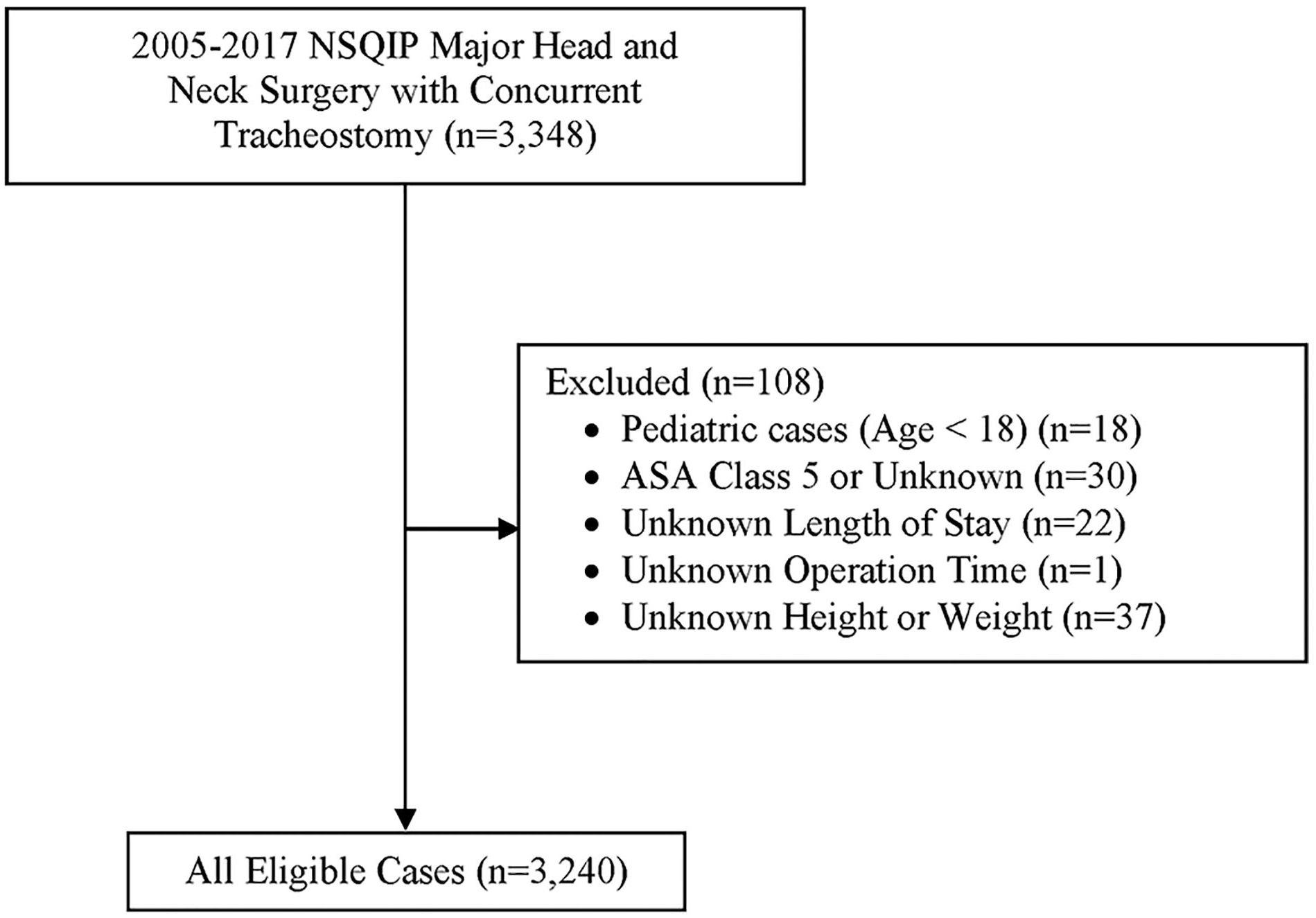
Diagram of patient selection and exclusion.
Statistical Analysis and Definitions of Variables
The NSQIP Data Dictionary defines all pre-operative and post-operative variables. 8 All post-operative variables are documented for 30 days. The readmission variable was only available for cases starting in 2011. Height and weight were used to calculate body mass index (BMI) and groups were classified using Center for Disease Control definitions. 10 Pre-operative characteristics and post-operative complications were analyzed with chi-squared tests except for categories with n < 5, which were compared with the Fisher’s exact test.
Multivariable logistic regression models were adjusted for pre-operative variables and used to analyze the association between outcomes of interest and underlying procedures. Length of operation and hospital stay were analyzed using non-parametric tests and reported as the median with the range. Statistical analysis was conducted in R version 4.0.2 and P < .05 was considered significant.
Results
Analysis Comparing Concurrent Tracheostomy with and without Complications
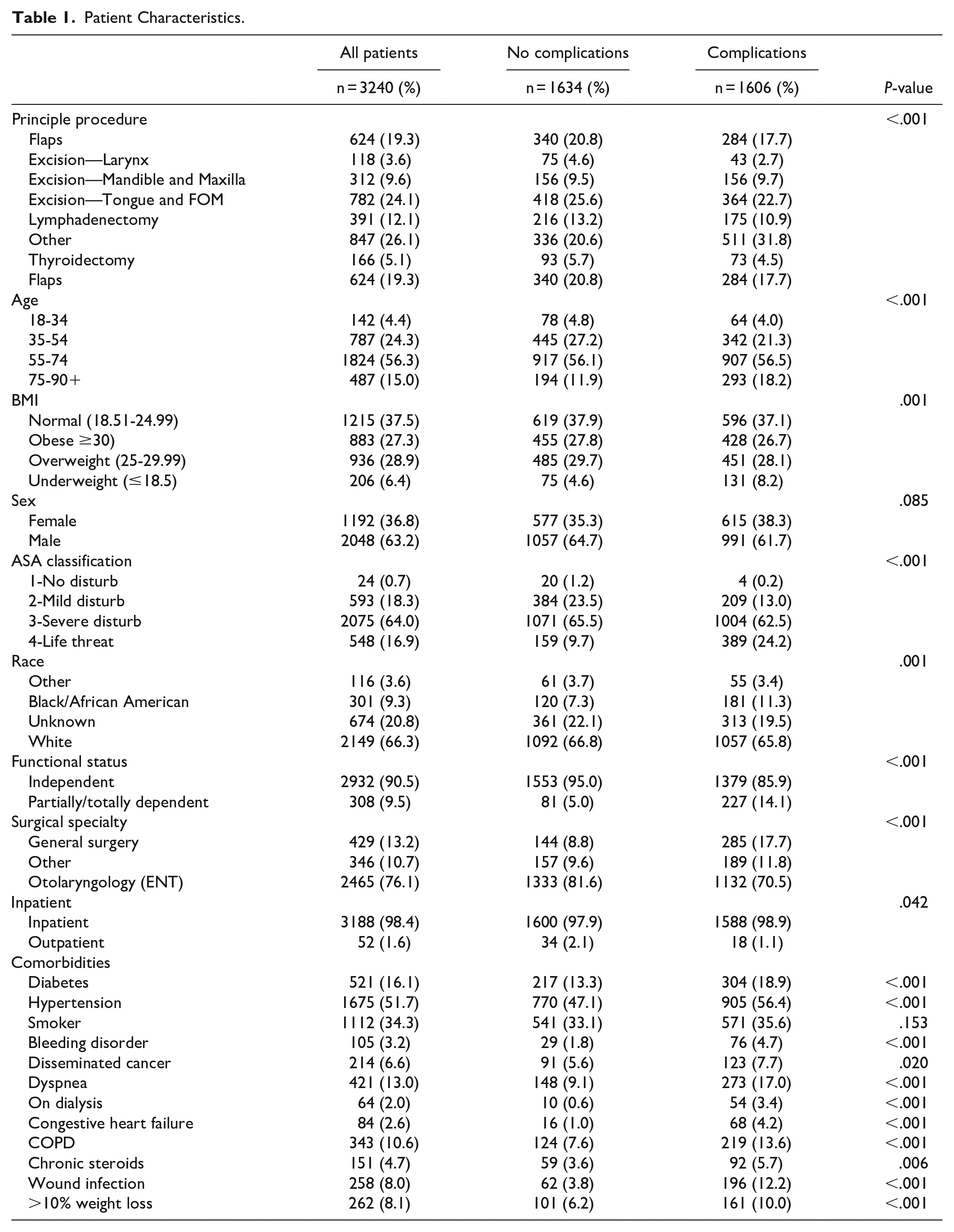
A multi-institution cohort of 3240 (2859 between 2011 and 2017) tracheostomy patients undergoing major head and neck surgery were identified in NSQIP (Figure 1). After major head and neck surgery with tracheostomy, there were 1606 (49.6%) non-tracheostomy specific complications. Complications were significantly more common in BMI ≤ 18.5 (8.2% vs 4.6%, P < .001), ASA Class 4 (24.2% vs 9.7%, P < .001), pre-operative wound infections (12.2% vs 3.8%, P < .001), and COPD (13.6% vs 7.6%, P < .001) as shown in Table 1.
Patient Characteristics.
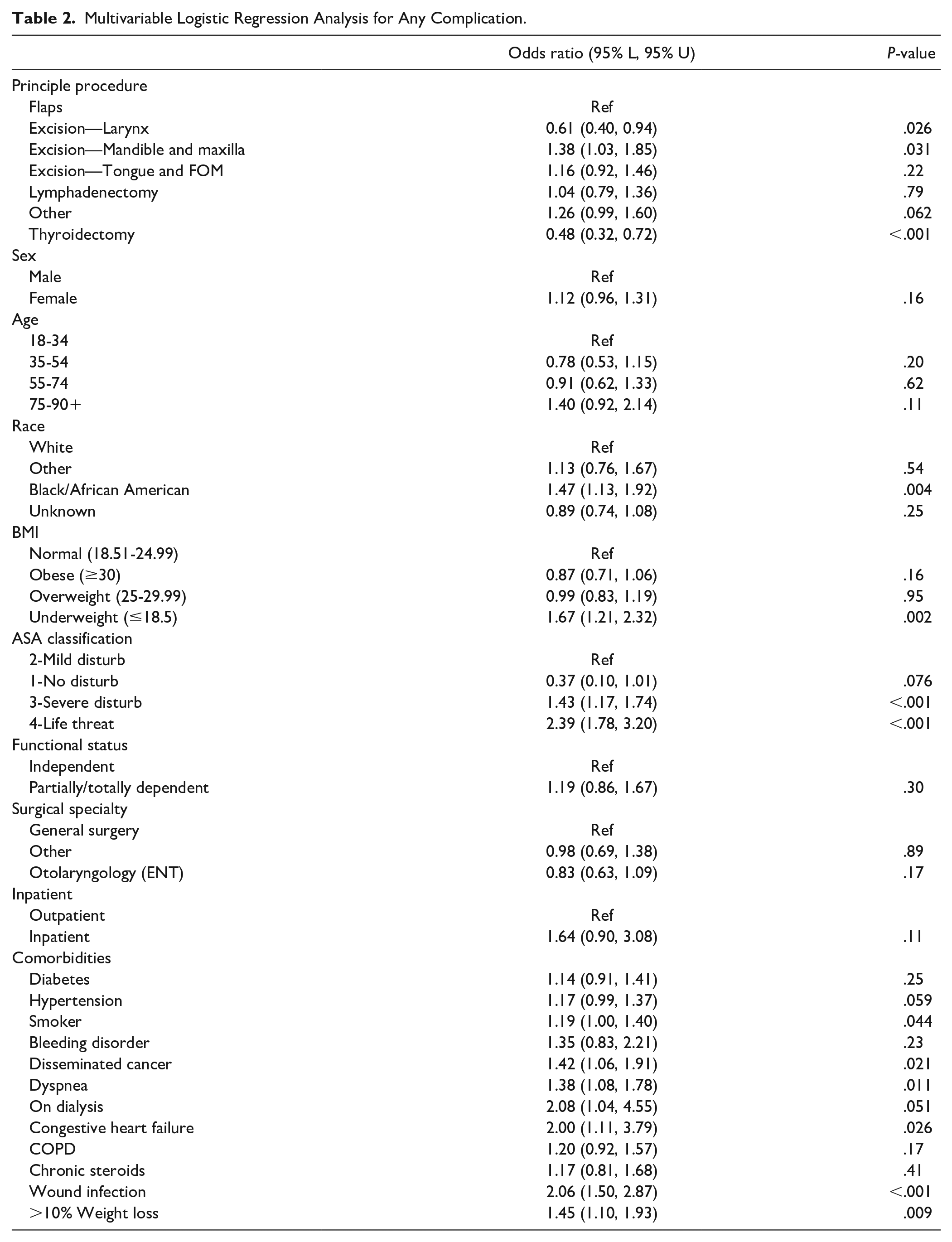
Using a multivariable model, the risk of any complication after performance of a tracheostomy with major head and neck surgery was less likely after thyroidectomy (OR = 0.48 (95%CI 0.32, 0.72), P < .001) and excisions of the larynx (OR = 0.61 (95%CI 0.40, 0.94), P < .001) relative to reconstructive flaps. The risk of any complication after surgery with concurrent tracheostomy was greater in BMI ≤ 18.5 (OR = 1.67 (95%CI 1.21, 2.32), P = .002), African American or Black patients (OR = 1.47 (95%CI 1.13, 1.92), P = .004), smokers (OR = 1.19 (95%CI 1.00, 1.40), P = .044), comorbid congestive heart failure (OR = 2.00 (95%CI 1.11, 3.79), P = .026), and pre-existing wounds (OR = 2.06 (95%CI 1.50, 2.87), P < .001). The complete model can be found in Table 2.
Multivariable Logistic Regression Analysis for Any Complication.
Post-Operative Complications in Tracheostomy Concurrent With Major Head and Neck Surgery
There were 1606 (49.6%) non-tracheostomy specific complications in patients undergoing major head and neck surgery with concurrent tracheostomy, which included 850 (26.2%) medical and 1142 (35.2%) surgical complications (Table 3). Surgical complications comprised 211 (6.5%) superficial surgical site infections, 162 (5.0%) wound dehiscence, and 806 (24.9%) intra/post-operative transfusions. Medical complications included 171 (5.3%) sepsis cases, 449 (13.9%) patients with ventilator dependence >48 hours, and 347 (10.7%) pneumonia cases. The 30-day mortality rate was 104 (3.2%), 258 (9.0%) patients were readmitted, and 637 (19.7%) had an unplanned return to the operating room.
Post-Operative Complications in Patients Undergoing Tracheostomy Concurrent With Major Head and Neck Surgery.
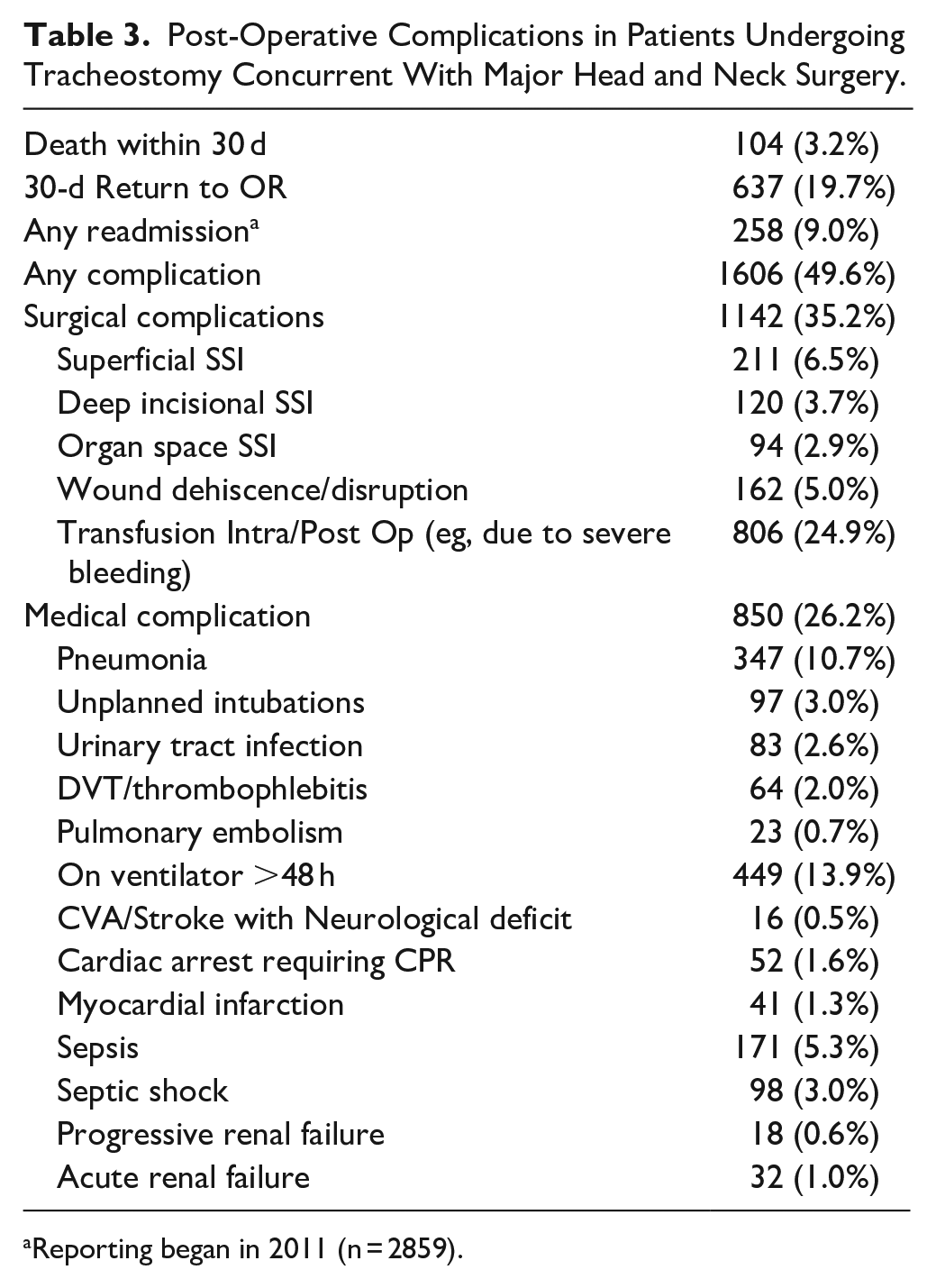
Reporting began in 2011 (n = 2859).
On multivariable analysis, we found that after performance of a tracheostomy with major head and neck surgery, the underlying procedures did not impact the risk of readmission (P > .05 for all) (Table 4). The underlying procedure was also not associated with unplanned return to the operating room except for in thyroidectomies, which had a lower risk than free flap reconstruction (OR = 0.53 (0.31, 0.88), P = .018). In terms of non-tracheostomy specific complications, compared to free tissue transfer, excisions of the larynx and thyroidectomy had a significantly lower complication rate (OR = 0.61 (0.40, 0.94), P = .026), OR = 0.48 (0.32, 0.72), P < .001, respectively), whereas maxillectomy was associated with a higher complication rate (OR = 1.38 (1.03, 1.85), P = .031).
Adjusted Odds Ratios for Readmission, Return to OR, and Complications in Major Head and Neck Procedures with Tracheostomy.
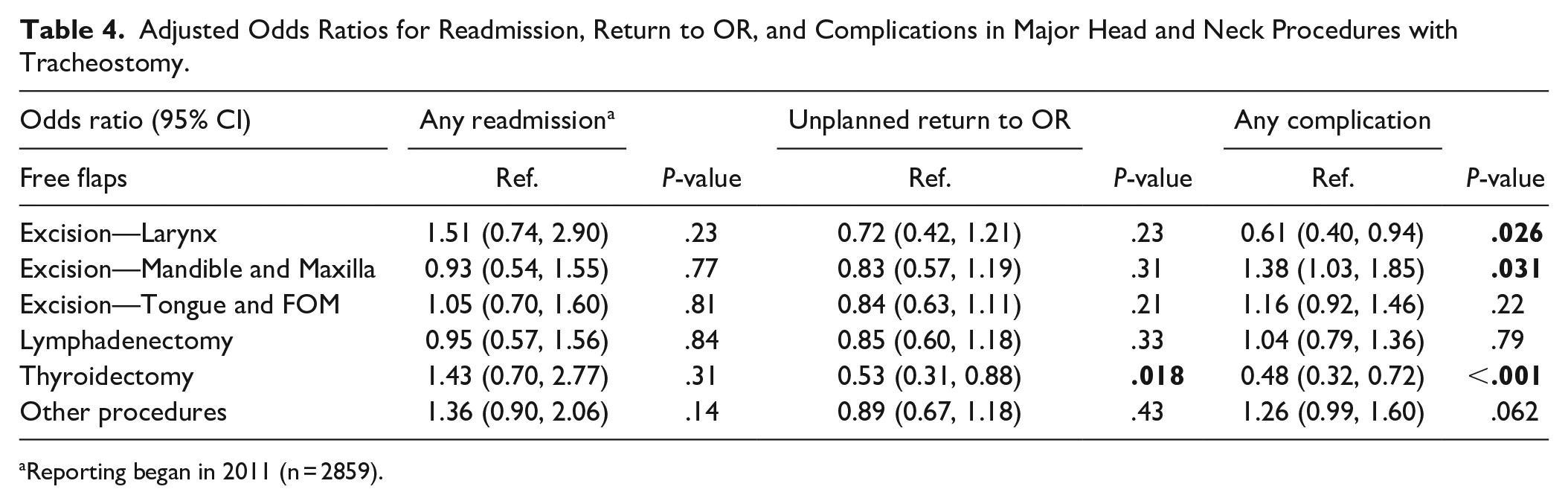
Reporting began in 2011 (n = 2859).
Discussion
Tracheostomy is a routine procedure in major head and neck surgery that is critical to preventing respiratory compromise. However, tracheostomy has the fifth highest readmission rate according to the Agency for Healthcare Research and Quality. Few studies have addressed the variation in underlying procedure during which the tracheostomy is place, which may directly impact the risk of readmission. Better understanding the factors that influence readmission rates is the basis for reducing rates, which can improve outcomes for tracheostomy patients in addition to lessening expenditure of healthcare resources. The objective of this study was to determine the influence of underlying head and neck procedures on readmission and complication rates following tracheostomy placement.
Readmission Rates Following Tracheostomy Concurrent With Major Head and Neck Surgery
In our study, readmission within 30-days following tracheostomy was relatively low at 9.0% in patients undergoing head and neck surgery. This finding was surprising compared to previous literature and especially given that our cohort included all major head and neck surgeries. 4 A recent single-institutional tertiary care center study of tracheostomies, only excluding patients with total laryngectomies, found an all-cause 30-day readmission rate of 33%. 5 It should be noted that the database used in our study tracks patients at the original hospital and at other hospitals in order to document every readmission and therefore has a low risk of underestimating readmissions. 8 We hypothesize that readmission rates in our cohort are lower due to the quality of follow up care provided to oncologic patients. One survey-based study of otolaryngologists estimated that less than 1 in 3 tracheostomy patients are asked to follow up for surveillance; far less than would be expected for head and neck cancer patients based on the National Comprehensive Care Network guidelines.11,12 However, it is also important to consider the comorbidities of the patients. In our study, the average head and neck patient was ASA Class 3, which is associated with a higher rate of readmission in a number of otolaryngology studies.13,14 Future prospective studies will be required to elucidate the relationship between readmission rates and tracheostomy concurrent with major head and neck surgery.
Adjusted Analysis of Outcomes in Tracheostomy Patients With Head and Neck Procedures
The overall low rates of readmission after tracheostomy for major head and neck surgery may indicate that the concern for readmission should not influence the decision to perform tracheostomy with head and neck surgery. As expected, non-tracheostomy specific complications were common in patients undergoing tracheostomy and major head and neck surgery.5-7 However, differences in the rate of complications between underlying head and neck surgeries did not correlate with a significant change in unplanned return to the operation room (except for in thyroidectomy) or readmission. These findings should reassure the head and neck surgeon that addition of tracheostomy does not significantly influence outcomes in the context of major head and neck surgery, especially given the high rate of documented complications.5,7 Furthermore, these data show that even in medically complex head and neck surgery patients, readmission rates after tracheostomy are lower than the global group of patients with tracheostomy. 4 This finding supports the notion that a lack of follow up care may play a major role in the disparate rates of readmission between tracheostomy patients as a whole and those with concurrent major head and neck surgery.
Complications and Associated Factors in Head and Neck Surgery With Tracheostomy
In an adjusted analysis, we found that there was a decreased risk of complications when thyroidectomy was the underlying procedure. It is well established that thyroidectomy is a relatively safe procedure with a low rate of complications.15-17 Additionally, we found that patients with pre-existing wound infection as a comorbidity and Black/African American patients had a substantially higher odds of having a complication, which are supported in the context of previous literature.18,19 In this way, these findings provide external validation for the results of our study. Our study also demonstrated that only specific comorbidities had a significant influence on the risk of complications. In particular, wound infections, congestive heart failure, and >10% weight loss increased the risk of complications, but diabetes, hypertension, and chronic steroids did not impact complication rates. We can only speculate on why comorbidities as a whole do not increase the risk of complications; however, these findings can be valuable for head and neck surgeons assessing patients for tracheostomy. Although tracheostomy is most often performed as a lifesaving procedure, a number of studies have noted the importance of proper patient selection for tracheostomy.1,20
Limitations
Limitations of this study include its retrospective nature and the lack of specificity in tracheostomy complications. Outcomes are also limited by the 30-day follow-up period for recording complications. NSQIP does not provide variables for tumor staging as well as for facility type, which may be important factors to adjust for in future analyses. Even with limitations, NSIQP benefits from being a multi-institutional database that allows for analysis of previously unidentified nationwide trends in readmission.
Conclusion
While there is a high rate of complications following head and neck surgery that includes creation of a tracheostomy, the rate of readmission is comparatively low and is not associated with the underlying procedure in patients undergoing major head and neck surgery. These findings should reassure head and neck surgeons that properly managed tracheostomies do not constitute a disproportionate risk of readmission.
Footnotes
Author Contributions
Philip R. Brauer: design, conducting, drafting manuscript, final approval, accountable for all aspects. Paul C. Bryson: design, conducting, drafting manuscript, final approval. William S. Tierney: design, conducting, drafting manuscript, final approval. Shannon S. Wu: design, conducting, drafting manuscript, final approval. Xuefei Jia: design, conducting, drafting manuscript, final approval. Eric D. Lamarre: design, conducting, drafting manuscript, final approval.
NSQIP Disclosure
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.