
Abstract
Objectives:
Lymphoma, categorized as either non-Hodgkin’s lymphoma or Hodgkin’s lymphoma, is the second most common malignancy in the head and neck. Primary tongue lymphoma is exceedingly rare, with only case reports or small case series in the literature. This population-based analysis is the first to report the epidemiology and prognostic factors of survival in patients with primary tongue lymphoma.
Methods:
The Surveillance, Epidemiology, and End Results 18 database from the National Cancer Institute was queried for patients diagnosed between the years 2000 and 2016 with tongue lymphoma. Outcomes of interest were overall and disease-specific survival. Independent variables included age at diagnosis, sex, race, marital status, primary subsite, histologic subtype, stage, and treatment type.
Results and Conclusion:
Seven hundred forty patients met criteria; the male-female ratio was 1.5:1 and the mean age at diagnosis was 67.8 years. The majority of lesions localized to the base of tongue (90.0%), were histologically diffuse large B-cell lymphoma (59.5%), and presented at stage I or II (77.9%). Most early-stage lymphomas were treated with chemotherapy only (40.5%) or a combination of both chemotherapy and radiation (31.3%), while late-stage cancers were primarily treated with chemotherapy alone (68.5%). In multivariate analysis, younger age at diagnosis, female sex, married/partnered marital status, mucosa-associated lymphoid tissue histologic subtype, and earlier cancer stage were found to be associated with improved survival. Chemotherapy treatment with or without radiation was also associated with better survival compared to no treatment or radiation alone, though data regarding immunotherapy was unavailable.
Introduction
Lymphoma, categorized as either non-Hodgkin’s lymphoma (NHL) or Hodgkin’s lymphoma (HL), represents the second most common malignancy in the head and neck after squamous cell carcinoma.1,2 NHL accounts for up to 90% of lymphomas in this region and can be further subdivided into those of nodal or extranodal origin.2,3 While primary extranodal lymphomas typically arise from mucosa-associated lymphoid tissues (MALT) within the gastrointestinal tract,4-6 another common site of involvement is Waldeyer’s ring (WR), a circular band of tissue at the opening of the aerodigestive tract comprised of the adenoids, tubal tonsils, and soft palate superiorly, palatine tonsils laterally, and base of tongue and lingual tonsils inferiorly.7,8 Up to 93% of primary lymphomas of WR localize to the palatine tonsils or nasopharynx, however, with rare involvement of the tongue. 9 Likewise, in the oral cavity, lymphoma tends to preferentially affect the gingiva or hard palate.10,11 Descriptions of tongue lymphoma in the literature are largely limited to case reports and small case series.12-14 To the best of our knowledge, a population-based analysis of primary tongue lymphoma in the United States has not been reported.
Our principal aim in this study is to assess the impact of various patient-, disease-, and treatment-related factors on overall survival (OS) and disease-specific survival (DSS) of patients with primary lymphoma of the tongue. Using the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute, this retrospective cohort study is the first to examine the epidemiologic characteristics of primary tongue lymphoma and the prognostic factors associated with this disease process.
Materials and Methods
Data Source
The SEER 18 database of the National Cancer Institute was utilized for data collection, 15 which includes cancer patients from registries in 18 areas of the United States covering approximately 27.8% of the population from 2000 to 2016. 16 Patient information was retrieved using SEER*Stat 8.3.8 (Surveillance Research Program, National Cancer Institute, Bethesda, MD). Because SEER data are de-identified, this study was exempt from approval by the Saint Louis University Institutional Review Board.
Study Population
Patients diagnosed with microscopically confirmed first/only primary tongue lymphoma from 2000 to 2016 were included. We defined tongue lymphoma as malignancies with International Classification of Diseases for Oncology third edition (ICD-O-3) histologic types 9590 to 9599 (Not otherwise specified (NOS)/diffuse malignant lymphoma), 9650 to 9669 (HL), 9670 to 9699 (mature B-cell NHL subtypes), and 9700 to 9719 (mature T- and natural killer (NK) cell NHL) with an ICD-O-3 primary site of C01.9 (base of tongue, NOS), C02.0 (dorsal surface of tongue, NOS), C02.1 (border of tongue), C02.2 (ventral surface of tongue), C02.3 (anterior two-thirds of tongue), C02.8 (overlapping lesion of tongue), and C02.9 (tongue, NOS). Exclusion criteria included unknown/missing cause of death, lymphoma only mentioned on death certificate/autopsy, and alive with no survival time.
Measures
The outcomes of interest were OS, defined as time from diagnosis to death of any cause, and DSS, defined as time from diagnosis to death due to cancer-related causes. Independent variables in the study included age in years at diagnosis, year of diagnosis, current smoker percentage within county of residence, current median household income within county of residence, sex, race, marital status, primary subsite of involvement, histologic subtype, stage at presentation, and treatment modality (radiation and chemotherapy, radiation only, chemotherapy only, no/unknown for both treatments). SEER does not allow for “no” and “unknown” radiation and chemotherapy to be separated because of concerns that the database does not capture all patients who received these treatments. 17 Surgery was reported but was not included in the statistical analysis, as surgical intervention is typically limited to diagnostic purposes in lymphoma.
Statistical Analysis
Kaplan-Meier survival curves plotted OS for independent variable values, and cumulative incidence curves plotted DSS. For these analyses, continuous variables were grouped into quartiles based on number of subjects. For each variable, survival comparisons to a predetermined reference value of that variable were made using log-rank chi-squared tests for OS and Gray’s chi-squared tests for DSS. The log-rank and Gray’s test results for the overall association of each variable with OS and DSS are also presented.
Multivariable associations of each independent variable with OS while controlling for all other independent variables were made using a Cox proportional hazards regression model, which yielded adjusted hazard ratios (aHRs) and 95% confidence interval (CIs). Similar multivariable associations with DSS were made using a Fine and Gray competing risks proportional hazards model, 18 which yielded sub-distribution hazard ratios (sdHRs) and 95% CIs. In both the univariable and multivariable analyses, patients were censored if they were alive on their last follow-up date, were lost to follow-up, or when they turned 100 years old. In analyses with DSS as the outcome, death from non-lymphoma causes was treated as a competing event. Analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC). All tests were 2-tailed, and results were considered significant if P < .05.
Results
Patient Characteristics
A total of 740 patients met criteria for inclusion in this study. Most patients were male (60.0%), married/partnered (56.1%), and Non-Hispanic White (73.5%) with an average age of 67.8 years (Table 1). The most common tongue lymphoma site was base of tongue (90.0%) and the most common histologic subtype was diffuse large B-cell NHL (59.5%). Patients presented most commonly with stage I (36.4%) or stage II (41.5%) cancers. When analyzed by stage, most early-stage tongue lymphomas were treated with chemotherapy only (40.5%) or a combination of both chemotherapy and radiation (31.3%), while only 10.1% of patients received radiation alone. Late-stage cancers were primarily treated with chemotherapy alone (68.5%). Only 16.4% of patients received surgery of the primary site, of which the majority (76.0%) were diagnostic local excisions and the remainder were of unclear extent.
Demographic and Clinical Information of Patients with Tongue Lymphoma.
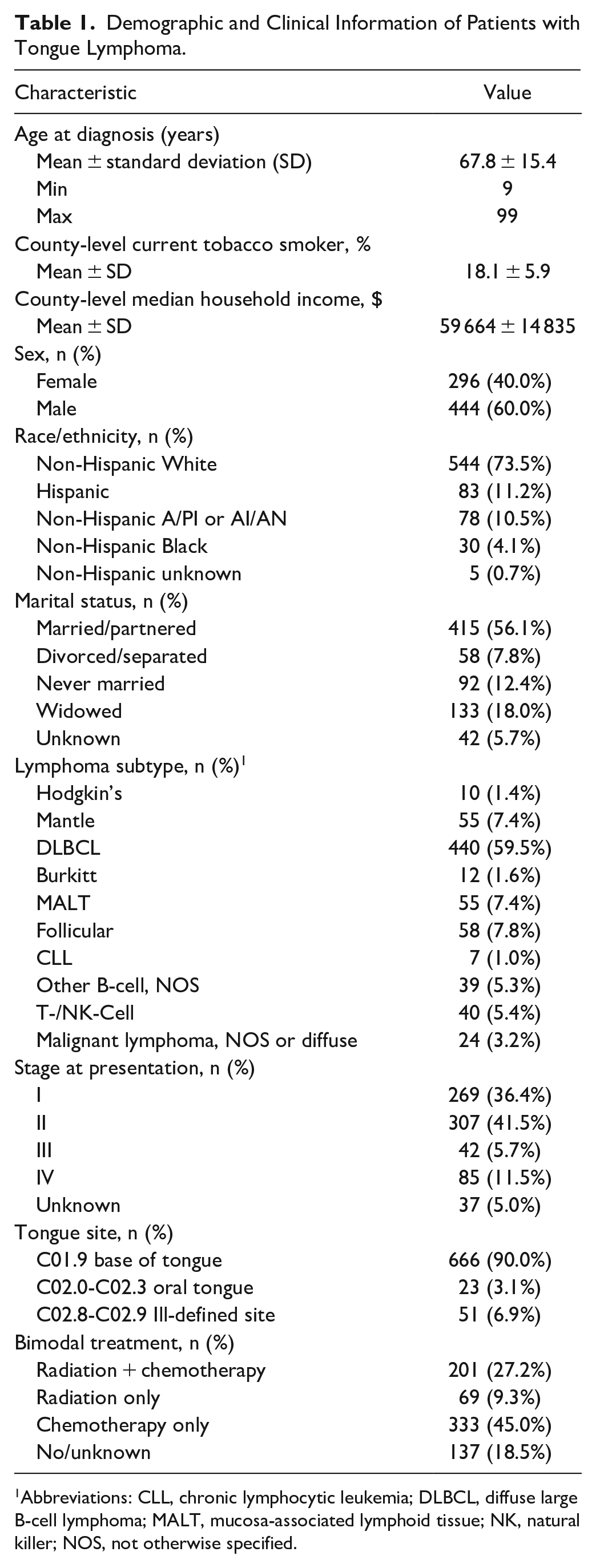
Abbreviations: CLL, chronic lymphocytic leukemia; DLBCL, diffuse large B-cell lymphoma; MALT, mucosa-associated lymphoid tissue; NK, natural killer; NOS, not otherwise specified.
Kaplan-Meier and Cumulative Incidence Curves
The median OS time for tongue lymphoma patients was 110 months; no median DSS time was reportable, as DSS did not fall below 0.50 for the duration of follow-up. Five-year OS and DSS rates were 65% and 77%, respectively.
In univariate analysis, increasing age at diagnosis, divorced/separated or widowed marital statuses, and advanced stage (stage III-IV) were significantly associated with worse median OS and 5-year lymphoma-specific mortality compared to their reference values (log-rank P value < .05) (Table 2). The overall effect of histologic subtype was associated with differences in median OS; however, no individual subtype was significantly different than the predetermined reference group of DLBCL. In terms of lymphoma-specific mortality, MALT histologic subtype was associated with higher DSS than DLBCL.
Median OS and Cumulative Lymphoma-Specific Mortality Statistics for Tongue Lymphoma. 1
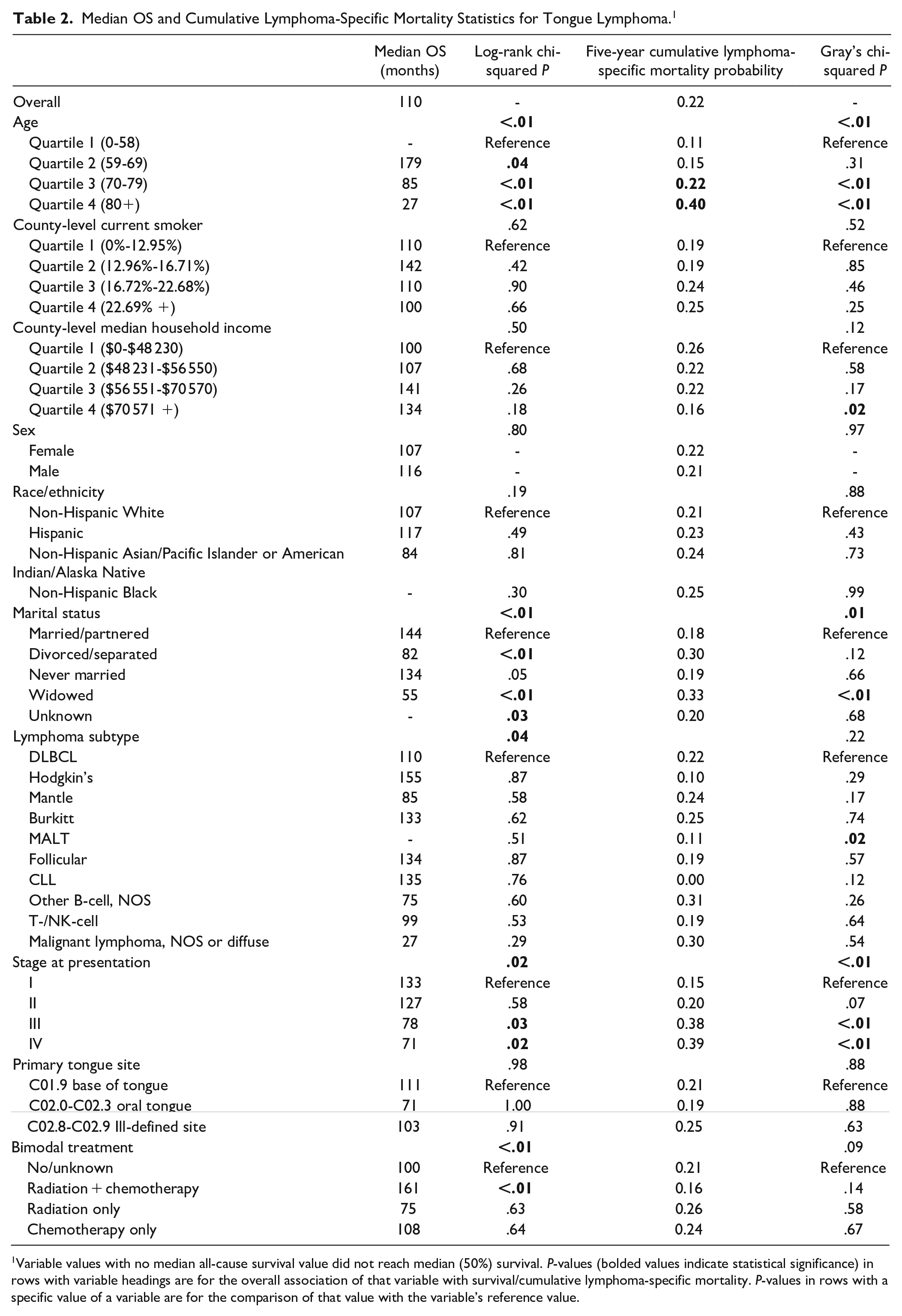
Variable values with no median all-cause survival value did not reach median (50%) survival. P-values (bolded values indicate statistical significance) in rows with variable headings are for the overall association of that variable with survival/cumulative lymphoma-specific mortality. P-values in rows with a specific value of a variable are for the comparison of that value with the variable’s reference value.
Combined chemoradiation treatment was significantly associated with improved OS but not DSS over no/unknown treatment, while neither treatment alone was associated with a survival advantage over no/unknown treatment (Figure 1). The highest quartile of county-level income was associated with favorable lymphoma-specific mortality compared to the lowest quartile. Sex, race/ethnicity, county-level smoking, and primary tongue subsite were not associated with either OS or DSS in univariate analysis, and no value was significantly different from the reference value for those variables.
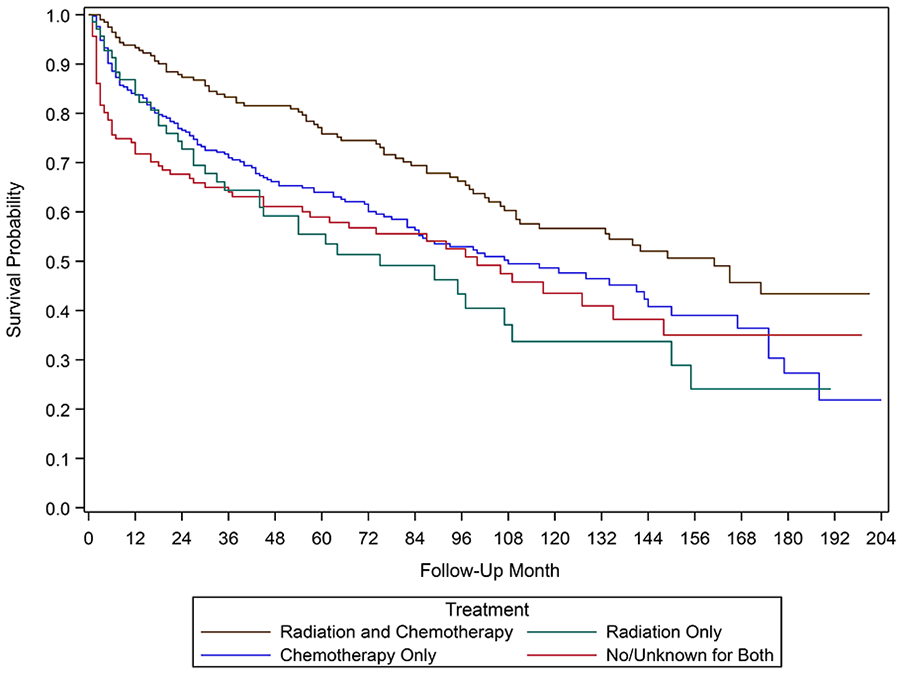
Kaplan-Meier curve depicting overall survival by type of treatment received.
Proportional Hazards Models
When controlling for the effects of all other independent variables in multivariate analysis, significant predictors of worse OS included advanced age, male sex, marital statuses of either divorced/separated and never married, histologic subtypes of Burkitt, T-/NK-cell, and malignant lymphoma NOS/diffuse, and stage IV cancers (Table 3). Treatment with combined chemoradiation or chemotherapy alone was associated with improved OS compared to no treatment.
Multivariable Analysis of the Association of Demographic and Clinical Factors with All-Cause and Lymphoma-Specific Mortality among Tongue Lymphoma Patients. 1
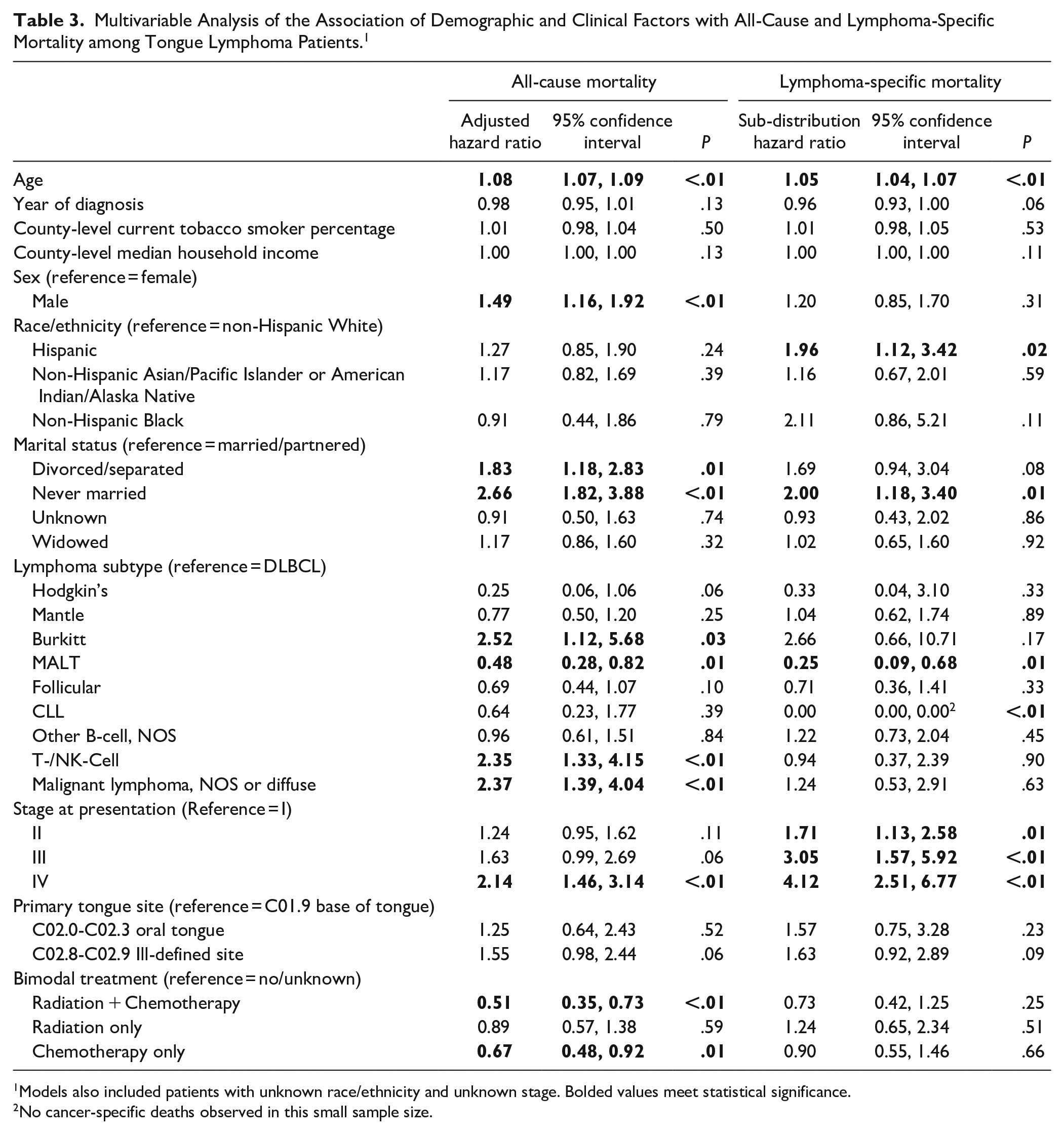
Models also included patients with unknown race/ethnicity and unknown stage. Bolded values meet statistical significance.
No cancer-specific deaths observed in this small sample size.
In terms of lymphoma-specific mortality, only advanced age, Hispanic race, never married status, and stage II or higher cancers were predictors of worse DSS. Notably, treatment was not associated with any significant change in DSS. MALT lymphoma was predictive of improved OS as well as DSS compared to DLBCL. Primary tongue subsite, county-level tobacco smoker percentage, and county-level median household income were not associated with survival in multivariate analysis.
Discussion
This population-based retrospective study represents the first to characterize primary tongue lymphoma on a large scale and examine the factors associated with survival in these patients.
Survival
Median OS time was 110 months, similar to that found within oropharyngeal lymphomas as a whole. 19 Previous reported series found an overall 5-year survival of 47% for lymphoma involving the base of tongue, though case numbers were quite limited 20 ; our population-based analysis reports a much higher 5-year OS rate of 65%, as well as a 5-year DSS of 77%.
Age and Sex
Mean age at diagnosis in our study was 67.8 years with a male to female ratio of 3:2, consistent with previous reports that tongue lymphoma more often affects males in the seventh decade of life.13,21 In comparison, WR and overall head and neck lymphomas were found in multiple prior studies to have a lower mean age at diagnosis ranging from 40 to 58 years.7,9 At least part of this discrepancy could be explained by poor visualization of the tongue base or submucosal tongue lesions on routine physical exam compared to other subsites like the palatine tonsils, as well as a higher propensity for other head and neck subsites to present initially with regional metastasis to the neck.7,22 Lymphomas of the tongue base also typically present with non-specific clinical features including pharyngeal discomfort, globus sensation, odynophagia, dysphagia, and/or referred otalgia, which may lead to initial misdiagnosis as an infectious or benign proliferative lesion.23-25
Increasing age at diagnosis was found to be significantly associated with worsening of both OS and DSS in primary tongue lymphoma patients. Each additional year of age portended an 8% and 5% increase in all-cause and lymphoma-specific mortality rates, respectively. In multivariate analysis, male sex was found to be associated with a 49% higher all-cause mortality compared to females. This is consistent with the sex-associated survival advantage that women have demonstrated across many different types of cancers, including HL and NHL.26,27 Although the reasons for this are not well understood, differences in hormonal levels or environmental exposures have been implicated, as well as a lower likelihood of cancer-related behaviors (smoking, alcohol, etc.) and possibly better treatment compliance in females.28-30 Continued studies are needed to further identify why such sex disparities exist in cancer survivorship.
Marital Status
Marriage and partnership were found to be associated with improved OS and DSS. Those who were divorced or separated were found to have an 83% increase in all-cause mortality compared to married or partnered patients, and patients who were never married had a 166% and 100% increase in overall and disease-specific mortality, respectively. The beneficial effects of marriage on cancer survival have been well-documented in previous studies. Osazuwa-Peters and colleagues recently examined head and neck squamous cell carcinoma (HNSCC) survivors and found that unmarried patients had a 66% increase in hazard of death compared to married patients. 31 Other studies suggest marriage as a significant predictor of survival not only in HNSCC but in other cancers as well.32,33 Many reasons for this have been postulated, including earlier presentation, enhanced initial and post-treatment surveillance, increased social and emotional support, and greater access to care for those who are married.30,31,34 Our study indicates that in tongue lymphoma patients, marriage continues to confer a protective effect on survival and may be an important consideration while caring for these patients.
Histologic Subtype
Overall, B-cell lymphomas comprised the vast majority (89.1%) of tongue lymphomas in our study, with DLBCL as the most common subtype. T-/NK-cell lymphomas made up only 5.4% of our cohort, and HL (1.4%) and CLL (1.0%) were exceedingly rare. The predominance of B-cell lymphomas is consistent with prior case series examining lymphomas of the tongue, which found that DLBCL accounted for more than two-thirds of NHL found in this region.23,35 While there are case reports of T-/NK cell tongue lymphoma in the literature, these tumors tend to affect the sinonasal region more than the oropharynx or oral cavity.10,36,37 Our data also reflects a similar histologic distribution to that of all oropharyngeal lymphomas, where B-cell lymphomas constitute over 82% of morphologies; HL is exceedingly rare given its predilection for cervical lymph nodes over extranodal sites.9,19,38
MALT lymphomas, low-grade neoplasms of B-cell origin often presenting in early stage, were the only subtype associated with a significant improvement in OS as well as DSS compared to DLBCL. 39 This is consistent with existing literature finding MALT lymphomas within the oropharynx to have the highest survival rates compared to other B-cell and T-cell subtypes, perhaps due to its favorable response to radiation therapy.19,40 Not surprisingly, T-/NK-cell and NOS/diffuse malignant lymphomas were associated with significantly lower OS compared to other histologies. T-cell and mixed lymphomas are known to have a poorer prognosis compared to those of B-cell origin due to the former’s often more aggressive behavior,41,42 which our findings confirm. Compared to DLBCL, Burkitt lymphomas were also associated with a significantly worse OS, although the very small sample size of this histologic subtype in our cohort limits meaningful conclusions. Though effects on DSS were not observed for most histologic subtypes, this may be because patients tend to be older at diagnosis and have multiple comorbidities which may contribute to mortality from non-lymphomatous causes.
Stage
Lymphoma is most commonly staged using the Ann Arbor staging system. This is based on the number of lymph nodes or extralymphatic regions affected, location of involvement, and presence of systemic symptoms. 43 The majority of patients (77.8%) in our study presented with early-stage disease (stage I-II). Saul and Kapadia reported on 68 patients with lymphoma of WR and noted all patients with tongue lesions had non-disseminated, early-stage disease. 7 However, we found at least 17.2% patients had advanced stage tongue lymphoma (stage III-IV) at time of diagnosis. Primary tongue lymphomas clearly have the potential to present at late stages with distant spread, perhaps due to the difficulty in diagnosis when localized to the tongue base. The distribution we found is similar to recent reports of lymphomas of the entire oropharynx, which found about 17.6% presented at advanced stage. 19
A compelling association between Ann Arbor staging and survival in primary tongue lymphoma has not been previously demonstrated, likely because of small sample size.7,23 In our study, stage at diagnosis was found to be a significant prognostic indicator of both OS and DSS. Patients with stage IV tongue lymphoma had a 2-fold increase in all-cause mortality compared to those with stage I lymphoma. Advanced disease was associated with an approximately 3 to 4 times higher risk of lymphoma-specific mortality compared to early-stage disease. These findings lend evidence-based support when counseling patients regarding their prognosis.
Treatment
No definitive treatment guidelines are available for primary tongue lymphoma given the paucity of data available. Treatment for head and neck lymphoma traditionally consists of chemotherapy and/or radiation therapy. Surgical excision is typically reserved only for diagnostic or salvage purposes. In the last 3 decades, immunotherapy agents including the monoclonal antibody rituximab have significantly changed treatment paradigms and improved outcomes in patients with B-cell NHL as well.44,45 Unfortunately, SEER does not report on whether patients received immunotherapy as part of their treatment course.
In multivariate analysis, bimodal treatment with chemotherapy plus radiation as well as single modality treatment with chemotherapy alone was significantly associated with an improvement in OS compared to no or unknown treatment (Figure 1), though no association with DSS was seen. Radiation alone was not associated with changes in OS or DSS. Laskar et al previously reported that in patients at their institution with primary nasopharyngeal NHL, the combination of chemotherapy and radiation resulted in a more than 2-fold increase in overall survival rate compared to treatment with chemotherapy alone.8,46 Patients with tonsillar NHL too had a significantly better outcome with chemotherapy plus radiation versus chemotherapy only. 47 While our results show a similar improvement in OS with combined chemoradiation treatment, they also suggest that chemotherapy alone can confer a survival advantage in tongue lymphoma, though potentially to a lesser extent than with combined modalities. Future studies would be needed to examine the additional effect of immunotherapy on survival outcomes. Most case reports and series in the literature have relied on established treatment models for other head and neck sites when treating patients with primary tongue lymphoma, often including a combination of conventional chemotherapy regimens and rituximab, with or without radiation.44,48-51 As multi-institutional prospective trials would be exceedingly difficult given the rarity of tongue lymphoma, this may be the most reasonable approach to treatment currently.
Study Limitations
A significant limitation of our study is the retrospective nature of using SEER, which prevents drawing causal inference between variables and may inherently lead to some degree of selection bias. As data is obtained from regions exclusively within United States, our findings may not be generalizable to the global population. Migration of patients out of geographic SEER catchment areas may also affect long-term follow-up of survival outcomes. 52
Several histologic subtypes including CLL, HL, and Burkitt lymphoma had very small sample sizes making estimates of their survival effect difficult to interpret. Conclusions regarding treatment should be drawn cautiously when utilizing SEER data. The current database does not separate no and unknown statuses for radiation and chemotherapy treatment, which limits the ability to truly characterize treatment effect on outcomes. Additionally, the specific chemotherapy regimens and extent of radiation protocols used were not included and likely differ between individual patients. Information on immunotherapy would make population-based studies on lymphoma even more robust.
With rare tumors like primary tongue lymphoma, reliance on large-scale cancer registries such as SEER are often necessary to obtain enough statistical power for meaningful results. Though these databases have inherent limitations that are difficult to avoid, they continue to be an indispensable tool in examining cancer epidemiology and prognostic indicators of survival.
Conclusion
Primary tongue lymphoma is a rare disease, more commonly diagnosed in males in the seventh decade of life. They are typically localized to the base of tongue, and DLBCL is the most frequently encountered histologic subtype. Younger age at diagnosis, female sex, married/partnered marital status, MALToma, and earlier cancer stage are associated with improved survival. Chemotherapy treatment with or without radiation may portend a better prognosis than no treatment or radiation alone, though data regarding immunotherapy is currently unavailable. Larger population-based analyses or prospective trials would be needed to further elucidate prognostic factors of survival in patients with primary tongue lymphoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.