
Abstract
Objectives:
To determine whether 2 different methods of post-operative head and neck free flap monitoring affect flap failure and complication rates.
Methods:
A retrospective chart review of 803 free flaps performed for head and neck reconstruction by the same microvascular surgeon between July 2013 and July 2020 at 2 separate hospitals within the same healthcare system. Four-hundred ten free flaps (51%) were performed at Hospital A, a medical center where flap checks were performed at frequent, scheduled intervals by in-house resident physicians and nurses; 393 free flaps (49%) were performed at Hospital B, a medical center where flap checks were performed regularly by nursing staff with resident physician evaluation as needed. Total free flap failure, partial free flap failure, and complications (consisting of wound infection, fistula, and reoperation within 1 month) were assessed.
Results:
There were no significant differences between Hospitals A and B when comparing rates of total free flap failure, partial free flap failure, complication, or re-operation (P = .27, P = .66, P = .65, P = .29, respectively). There were no significant differences in urgent re-operation rates for flap compromise secondary to thrombosis and hematoma (P = .54).
Conclusions:
In our series, free flap outcomes did not vary based on the degree of flap monitoring by resident physicians. This data supports the ability of a high-volume, well-trained, nursing-led flap monitoring program to detect flap compromise in an efficient fashion while limiting resident physician obligations in the age of resident duty hour restrictions.
Keywords
Introduction
Within the head and neck, free flap failure occurs at a rate of 1% to 8%.1-5 Vascular compromise is a cause of failure that most commonly occurs 24 to 48 hours post-operatively,2,6-8 necessitating a surgical revision in 10% to 60% of cases.2,3,9-11 Early identification and revision of a compromised flap results in a higher rate of salvage and thus a higher rate of free flap success when compared to no intervention.2,6-8,11 With the wide range of salvage rates and morbidity associated with flap failure, investigation regarding optimal post-operative free flap monitoring is an active area of research.
In order to identify free flap compromise early in its course, the patient must be thoroughly examined at frequent intervals. Physical examination of the free flap recipient site is primarily aimed at identifying venous congestion or ischemia consistent with thrombosis of the pedicle vein or artery, respectively. Patients are closely surveilled for hematoma or infection which may result in anastomotic compromise. Adjunctive measures, such as an implantable doppler to monitor blood flow at the arterial or venous anastomosis, can supplement but not replace the free flap examination. Therefore, it is important to train resident housestaff, advanced practice providers, and nurses to look for signs of vascular compromise.
Since 2013, the lead author has developed a high volume microvascular reconstructive surgery practice that is evenly divided between 2 separate hospitals within the same tertiary care health system. Based upon limitations of resident physician on-call responsibilities, 1 hospital has relied primarily on flap checks performed by registered nurses while the other hospital heavily utilizes around the clock in-house resident physician flap monitoring in addition to nurse monitoring. This retrospective review of 2 academic hospitals within the same health system provides a unique opportunity to compare 2 separate flap monitoring protocols while keeping other variables constant.
Materials and Methods
A retrospective review was performed for all patients undergoing microvascular reconstructive surgery of the head and neck by a single reconstructive surgeon (S.B.C.) from July 2013 to July 2020. Patient information was obtained under a University of Pennsylvania Hospitals Internal Review Board approved study (IRB#818595). Eight-hundred and three free flaps were performed during this time period at the same academic health system. Four-hundred and ten (51%) free flaps were performed at Hospital A, while 393 (49%) free flaps were performed at Hospital B. Both hospitals utilized the same complement of otolaryngology residents and head and neck fellows for patient management; however, frequency of physician-led post-operative free flap monitoring differed between the 2 hospitals as shown in Figure 1. The attending surgeon’s preference at both hospitals was to round routinely once per week on his free flap patients, usually on post-operative day one. The attending surgeon also evaluated any patient with potential flap compromise prior to taking them to the operating room, time permitting.
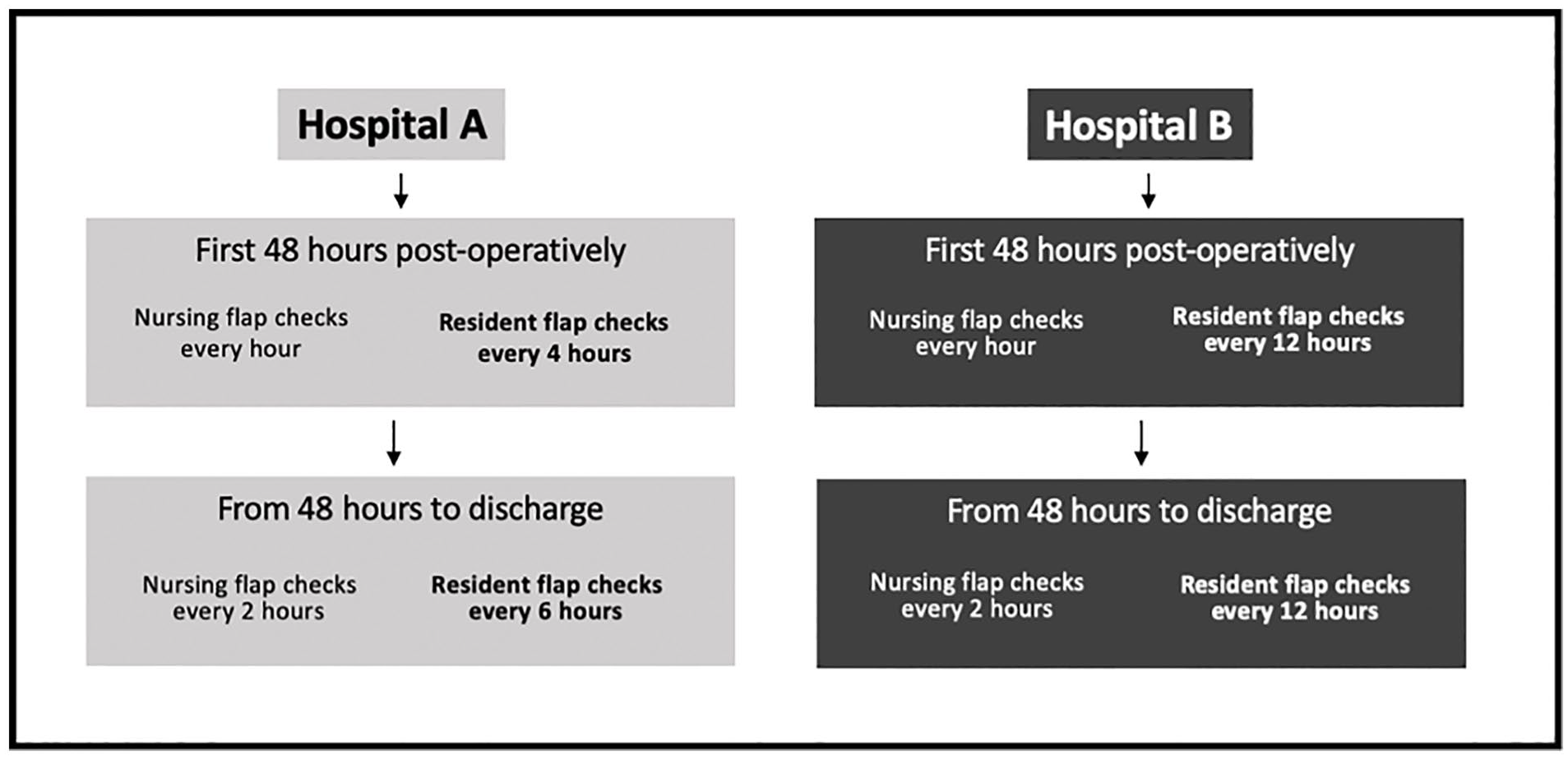
Post-operative flap monitoring protocol at Hospital A and Hospital B during the study period, July 2013 to July 2020.
At both hospitals, the post-operative flap monitoring by nursing staff was the same and consisted of flap checks every hour for the first 48 hours post-operatively, followed by every 2 hours until discharge. Hospital A had in-house otolaryngology resident(s) at all times that performed flap checks every 4 hours for the first 48 hours post-operatively, followed by every 6 hours until discharge. In contrast, Hospital B did not have in-house resident(s) at night and thus routine in-person flap checks were performed by a resident approximately every 12 hours at the beginning and end of the day shift. At both hospitals, concerning flap findings identified by nurses could be conveyed to the resident who then triaged based on medical judgment, sometimes including additional in-person evaluation. The nursing staff at the 2 hospitals was different, but all nurses had similar experience and training in free flap monitoring, and utilized clinical examination supplemented with external and implantable Doppler checks when available. Unit acuity and nursing coverage ratios (no more than 2 free flap patients under the direct care of any given nurse) were also identical between Hospital A and Hospital B.
Free flaps with an external component were monitored with physical examination of the external paddle to assess for warmth, turgor, and color. Pin-prick or scratch of the external paddle was used when deemed necessary by the physician team to assess for adequate venous drainage or arterial perfusion. Arterial patency was monitored in all microvascular free flaps at both hospitals using an implantable Doppler overlying the arterial supply distal to the microvascular anastomosis. All free flap patients were prescribed a 325 milligram aspirin tablet daily for the first 30 days post-operatively unless there was a previous allergy noted.
Patient-level data abstracted from the electronic medical record (EMR) included sex, indication for reconstruction, tumor stage, donor site, history of radiotherapy (XRT) or chemotherapy (CRT), and history of prior head and neck ablative or free flap surgery. Total free flap failure, partial free flap failure, and complication rates were the primary outcomes of interest. Complication rates included the occurrence of any surgical complications occurring prior to post-operative day 30 (including surgical site infection, fistula, wound dehiscence, hematoma, seroma, gross tumor recurrence, chyle leak, cellulitis, hemorrhage, tracheostomy decannulation, and vocal cord paralysis) or medical complications that prolonged hospital stay or required peri-operative readmission (including bowel ischemia, malnutrition, tracheitis, cardiac arrest, pulmonary embolus, ascites, hyperkalemia, colitis, diverticulitis, deep venous thrombosis, pneumonia, delirium, stroke, and small bowel obstruction.) Total free flap failure was defined as a failure that required explanation of the entire flap while partial free flap failure included cases where a component of the free flap underwent necrosis and required subsequent debridement. Reoperation rates and urgent reoperation rates were evaluated as secondary outcome measures. Time to reoperation could not be gathered precisely due to constraints of our chart review.
Statistical analysis between categorical variables was performed using a Chi-squared analysis with the Fisher exact test for all contingency tables that included an event rate less than 10. P-value <.05 was considered statistically significant. Statistical analysis was performed using Stata statistical software (Statta Corp LLC, College Station, TX, USA).
Results
Patient characteristics at hospitals A and B are summarized in Table 1 and their correlations with the primary outcome of total free flap failure are listed in Table 2. The majority of free flaps performed at both hospitals were soft tissue flaps (85% for Hospital A and 75% for Hospital B) with the anterolateral thigh (ALT) and radial forearm free flaps (RFFF) used most commonly. No free flaps were performed in the setting of trauma, but there were 35 cases (4.4%) for osteoradionecrosis of the mandible, accounting for 30 of the cases at Hospital B (7.6%) and 5 cases at Hospital A (1.2%). The remaining free flaps (768, 95.6%) were performed in the setting of either tumor resection or chronic non-healing wound. There was a significant difference noted in the donor site distribution between the 2 hospitals (Table 1). Hospital B also had a greater proportion of patients who had previously undergone head and neck ablative surgery, free flap surgery, and radiotherapy or chemoradiotherapy for head and neck cancer.
Patient Characteristics in a Series of 803 Free Flap Patients at Hospital A and Hospital B within the Same Academic Health System.
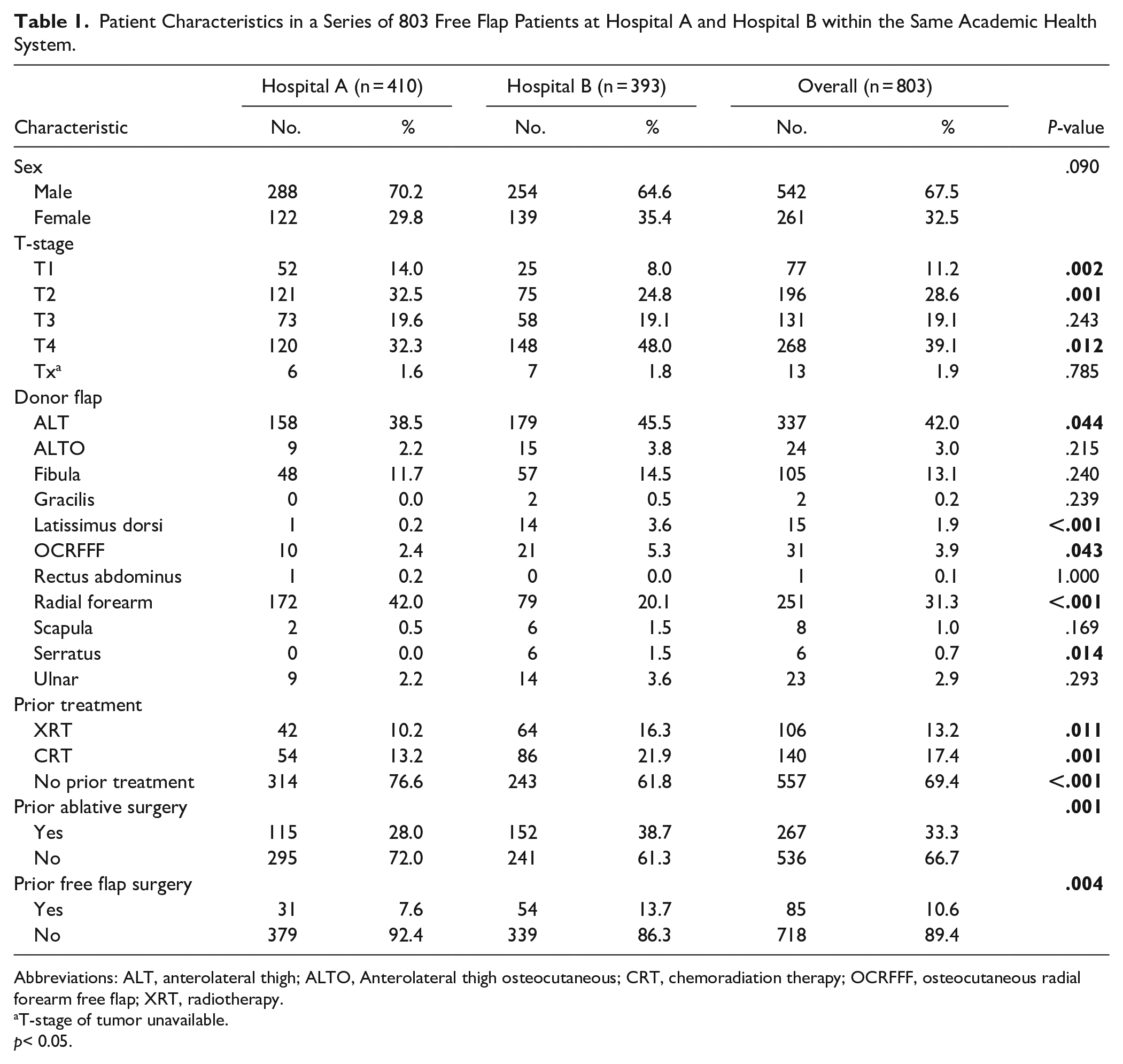
Abbreviations: ALT, anterolateral thigh; ALTO, Anterolateral thigh osteocutaneous; CRT, chemoradiation therapy; OCRFFF, osteocutaneous radial forearm free flap; XRT, radiotherapy.
T-stage of tumor unavailable.
p< 0.05.
Patient Characteristics in Relation to Total Flap Failure. Odds Ratios Compare Flap Failure Rate in Each Group to Expected Flap Failure Rate If Flap Failure and Patient Characteristics Are Independent Variables.
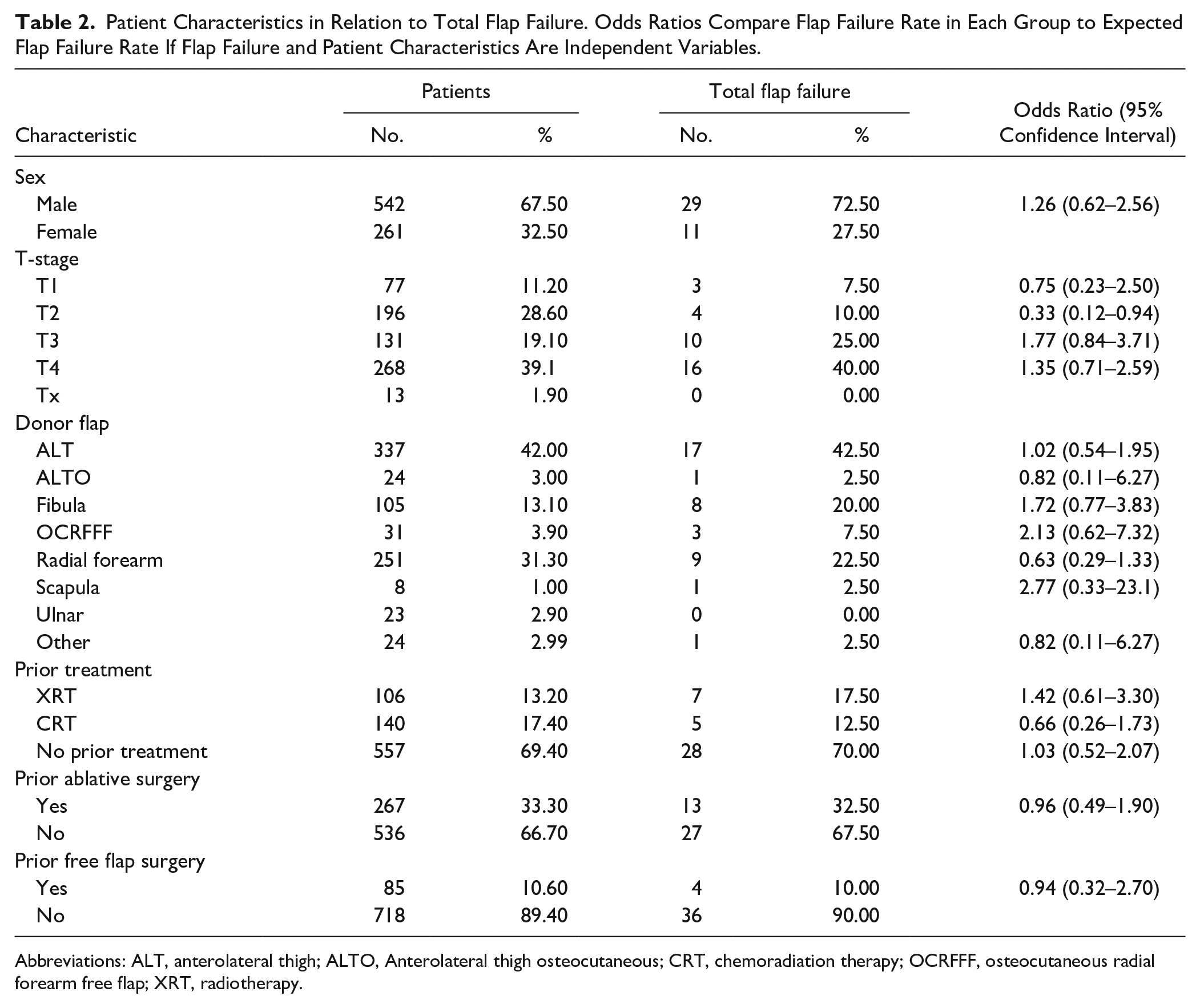
Abbreviations: ALT, anterolateral thigh; ALTO, Anterolateral thigh osteocutaneous; CRT, chemoradiation therapy; OCRFFF, osteocutaneous radial forearm free flap; XRT, radiotherapy.
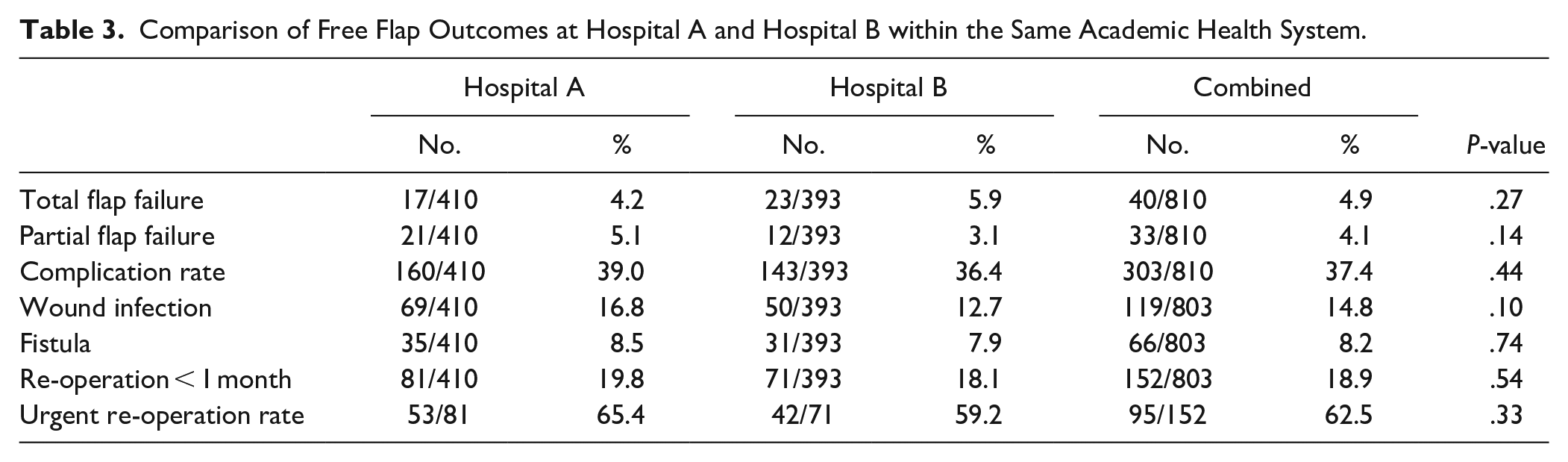
For each primary and secondary endpoint which included total free flap failure, partial free flap failure, complication rate, and re-operation rate, there was no significant difference in outcomes between hospitals A and B (4.2 vs 5.9%, P = .27; 5.1 vs 3.1%, P = .66; 39.0 vs 36.4%, P = .65; 19.8 vs 18.1%, P = .29, respectively; Table 2).
Successful salvage rates for compromised flaps were nearly identical between the 2 hospitals—urgent reoperation salvaged 37 of 49 (75.5%) compromised flaps at Hospital A and 29 of 39 (74.4%) such flaps at Hospital B. Flap compromise secondary to vascular complications occurred at a similar rate between the 2 hospitals, with 19 flaps from Hospital A and 16 flaps from Hospital B requiring urgent return to operating room for presumed vascular compromise. Of these flaps with vascular compromise, 68.4% (13 of 19) and 75.0% (12 of 16) were successfully salvaged at hospitals A and B, respectively.
Discussion
The need for post-operative monitoring after free flap reconstruction is well accepted within the microvascular surgery community, however the methods by which microvascular surgeons monitor their patients post-operatively varies across the country. Many surgeons rely heavily on pinprick while others utilize various combinations of implantable and external Doppler signals from the pedicle artery, vein, or both vessels.1,10 The frequency of physician-led free flap monitoring reported in the literature ranges from every 2 hours to every 12 hours in the first 24 to 72 hours, followed by a de-escalation of frequency.8,10-12 Despite these varying post-operative free flap monitoring methods, multiple studies report similar overall success rates.1-10,12 It is difficult to compare these studies directly however, given the nuanced differences that occur between various surgeon and institutional practices.
While the role of free tissue transfer in head and neck reconstruction has expanded over the past 2 decades, the regulation and restriction of house staff duty hours have also increased. In 2003, duty-hour standards were enacted for all accredited residency programs by the Accreditation Council for Graduate Medical Education (ACGME), limiting the duration of shifts and total hours per week that residents can work. 13 The aim of these regulations was to promote high quality learning and safe patient care in teaching institutions. 14 Maintaining compliance with resident duty hour mandates while providing appropriate post-operative monitoring of complex head and neck cancer patients has proven to be challenging within otolaryngology and plastic surgery residency programs across the country.
This study is unique in that it includes 2 nearly identical cohorts undergoing post-operative free flap monitoring protocols that differ only in frequency of resident-led free flap monitoring. The implications of this study are important in the context of resident duty hour restrictions, as it has become important to place necessary limitations on resident physician work hours without sacrificing patient care and outcomes. Our results show that there is no difference in total flap failure, partial flap failure, re-operation within 1 month, urgent re-operation rate, or complications consisting of fistula or wound infection when resident physicians use a less demanding monitoring schedule and rely on a standardized nursing protocol.
Although no significant differences were noted in free flap outcomes between Hospital A and Hospital B, the patient populations did vary between hospitals. These patient differences are almost entirely due to the difference in referral patterns for the senior author between the 2 hospitals in this study. For instance, Hospital A included a larger number of patients (140 patients, 34.1%) who underwent RFFF reconstructions for ablative defects of the oropharynx compared to Hospital B (30 patients, 7.6%). This flap is the senior author’s preferred donor site to repair soft palate, tonsil, and base of tongue defects which were more prevalent at Hospital A, largely due to a higher volume of primary surgical therapy for oropharyngeal cancer requiring free flap reconstruction. Multiple studies have shown higher overall success rates when a RFFF is used relative to other free flaps.12,15,16 Our study hinted at an association with RFFF utilization and decreased total free flap failure, but failed to reach statistical significance (Table 2).
Hospital B included a higher proportion of patients who had undergone prior head and neck ablative surgery, free flap surgery, radiotherapy, and chemoradiotherapy for head and neck cancer. Multiple previous studies have shown lower rates of free flap survival in the setting of previous head and neck surgery and chemoradiation therapy,17,18 however in our study none of these patient factors were correlated with a statistically significant difference in total free flap failure (Table 2).
In general, Hospital B had a more complex reconstructive population given that these patients had a higher rate of T4 tumors, bony free flap reconstruction, previous ablative surgery, previous free flap surgery, previous radiation, and previous chemoradiation. Also, of the 35 free flaps performed in the setting of osteoradionecrosis, 30 were performed at Hospital B (85.7%). This was likely due to the higher rate of previously radiated patients seen at Hospital B. As these patients also had decreased physician-led free flap monitoring, it is encouraging that there was no significant difference in the measured outcomes for these patients compared to Hospital A (Table 3).
Comparison of Free Flap Outcomes at Hospital A and Hospital B within the Same Academic Health System.
One drawback of restricting patient data analysis to a single reconstructive surgeon was that it limited the potential sample size of our study. It is possible that our study of 803 patients, although large for a single surgeon’s experience, was underpowered to detect a significant difference in desired outcomes listed in Table 3. Using estimates from the aforementioned published data on patients who underwent head and neck free flap reconstruction, total flap failure rates have ranged from 1% to 8%.1-5 Post hoc calculations to compare a flap failure rate of 1% to 8% with a power of 0.8 and an α of .05 showed the sample size needed to detect a significant difference was 137 patients in each group (or 274 patients total), which was far exceeded in our study of 803 total patients. A 7% difference in free flap failure rates is admittedly rather conservative, so we performed a retrospective power calculation assuming a more stringent flap failure rate difference of 4%. With this 4% difference noted between a 2% and 6% flap failure rate, subsequent calculations using the 803 patient sample size from our study with an α of .05 produced a power of 83%. These post hoc calculations will always be inferior to a direct comparison in a randomized clinical trial, however they do validate the significance of the results shown in our retrospective study.
Given the findings of this study, mandates for around the clock resident flap monitoring at Hospital A were lifted and physician-led flap checks are now encouraged only if there is no risk of violating resident duty hour restrictions. In the future, it will be important to standardize protocols across hospitals within the same healthcare system in order to provide uniform care. In addition to multicenter studies, the continued consolidation of hospitals into larger systems affords many unique opportunities to evaluate which pathways of care provide optimal outcomes for our patients.
Conclusions
Within high-volume centers, the implementation of nursing-led free flap monitoring can result in high quality post-operative care for patients who have undergone microvascular reconstruction. With proper training and communication practices, nursing-led free flap monitoring can be utilized to decrease the burden placed upon resident physicians who must comply with duty hour restrictions. These findings are also encouraging for head and neck microvascular surgeons who wish to build a high-volume practice in clinical settings with limited resident physician coverage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.