
Abstract
Objectives:
To report a case of a morbidly obese 17-year-old boy who presented 4 days post-tonsillectomy with acute deep venous thromboses and a massive pulmonary embolism. To describe a protocol and decision-making tree for providing anticoagulation in the immediate post-tonsillectomy period.
Methods:
A chart review and review of the literature.
Results:
The patient ultimately did well and had no bleeding from the tonsil beds or further thromboembolic complications. A review of the literature revealed no available data regarding the safety of anticoagulation in the immediate post-tonsillectomy period.
Conclusions:
We propose that if anticoagulation is needed within 14 days of tonsillectomy, submaximal anticoagulation with a reversible and titratable anticoagulant may be optimal. A multidisciplinary team approach is needed for these complex cases. Future reporting and investigation of anticoagulation post-tonsillectomy is needed.
Keywords
Introduction
Bilateral tonsillectomy with adenoidectomy (T&A) is one of the most frequently performed surgeries in Otolaryngology. The most significant risk following tonsillectomy is bleeding that can be severe and difficult to control. Post-tonsillectomy hemorrhage (PTH) is unpredictable and can occur even in patients with normal preoperative coagulation studies. 1 PTH is most common during the first 5 to 10 days following the procedure with the highest risk at day 6. 2 This risk correlates with the time when fibrin clots slough in the tonsillar fosse, revealing underlying vascular stroma. The vascular stroma subsequently involutes, coinciding with a decline in bleeding risk throughout the second week following surgery. 3 The bleeding risk remains elevated at least 2 weeks post operatively with bleeding episodes reported as far out as 21 days. 4 Most Otolaryngologists therefore instruct their patients to limit their physical activity for at least 2 weeks following a tonsillectomy.3-5
While the risk of PTH in patients receiving NSAIDS has been well studied, there is no literature describing the safety or strategy of anticoagulant use when necessary in these patients.6-8 We present a unique case in which a teen developed a post-tonsillectomy massive pulmonary embolism (PE) necessitating urgent anticoagulation. The lack of data and literature guiding our treatment in this case prompted an investigation of anticoagulant safety in the immediate post-tonsillectomy period and led us to develop a treatment algorithm for these rare but life-threatening cases.
Case Report
A 17-year-old morbidly obese male (body mass index 52.25 kg/m2) with hypertension, obstructive sleep apnea (OSA), asthma, and family history of PE underwent T&A at an outside hospital for management of severe OSA. There were no intraoperative complications and he was observed overnight in a pediatric step-down unit and discharged the following day. On postoperative day (POD) 4, he presented to our Emergency Department (ED) after a syncopal episode followed by persistent chest pain, dyspnea, abdominal pain, nausea, and vomiting. On admission, his hemoglobin (Hgb) and platelet count were 12.7 g/dl and 245,000 k/ul, respectively. Workup, including spiral computed tomography (CT) scan with contrast of the chest, revealed a saddle PE with substantial proximal bilateral thrombotic burden, along with involvement of multiple segmental and subsegmental arteries (Figure 1). An echocardiogram demonstrated right heart strain and significantly compromised right ventricular systolic function, along with an increased right ventricle/left ventricle (RV/LV) diameter ratio of 1.6 (Normal = 0.8) (Figure 2). There was evidence of RV ischemia with elevated troponin and brain natriuretic peptide. Duplex ultrasonography demonstrated multiple left lower extremity deep venous thromboses (DVT).
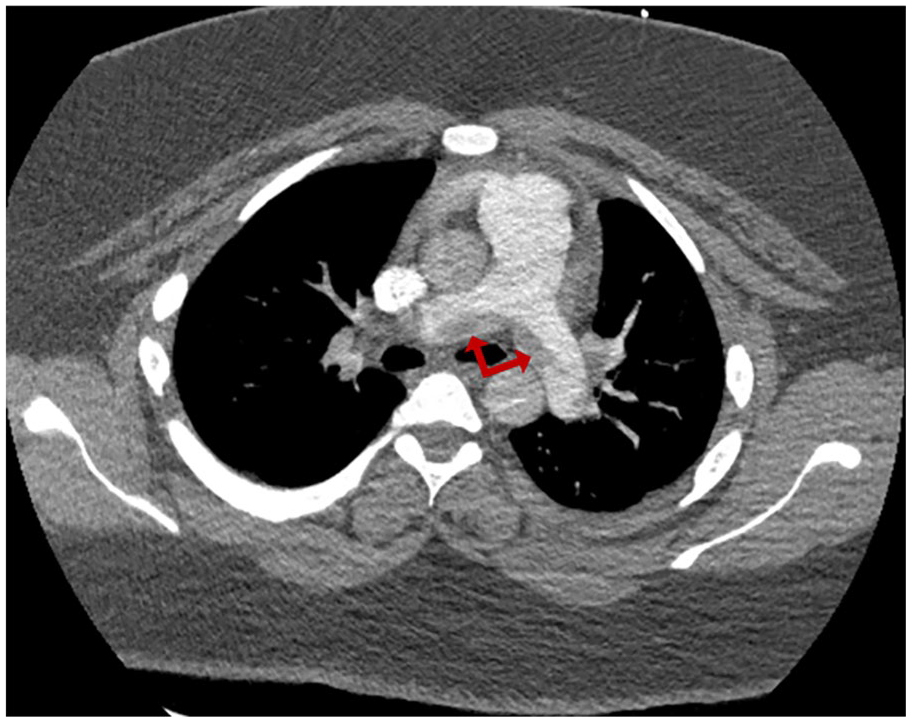
Axial spiral computed tomography scan of the chest with intravenous contrast demonstrating a massive saddle embolus at the bifurcation of the main pulmonary artery (red double arrow).
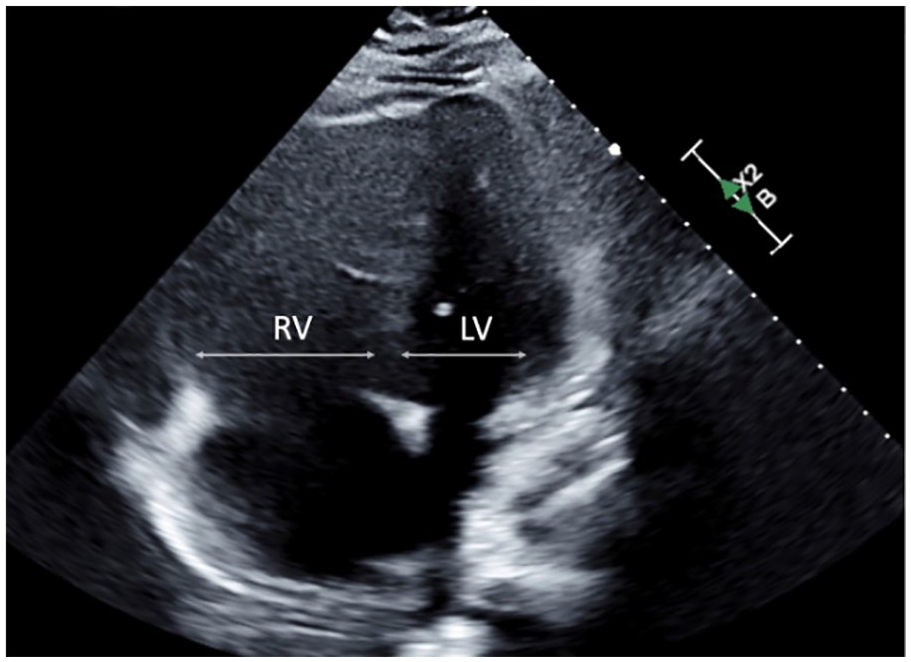
Echocardiogram demonstrating significant enlargement of the right ventricle (RV) secondary to massive PE. There is increase in the RV to left ventricular ratio (LV) at 1.6 (normal 0.8).
The hospital’s PE Response Team (PERT) was activated and considered this to represent a massive PE given the patient’s syncopal episode and multiple risk factors for cardiovascular decompensation and death.9,10 The Pediatrics team, after consulting with PERT and Hematology, wished to begin therapeutic-level anticoagulation to minimize the risk of clot propagation and re-embolization, per protocol. The Otolaryngology service was consulted to advise on the bleeding risk if anticoagulation were to be initiated just 4 days following surgery. Complicating the picture, PERT was concerned about the patient’s high risk of catastrophic cardiovascular decompensation if general anesthesia was required to control a tonsil bed hemorrhage.
Per our Otolaryngology team’s exam, the patient’s tonsil beds contained well-seated healthy-appearing fibrin clots and showed no signs of imminent bleeding. The Pediatrics team was advised that while there is no definitive evidence to guide the anticoagulation strategy in this situation, at 4 days postoperatively, the patient fell well within the high-risk bleeding period following a tonsillectomy. After a multidisciplinary discussion, and given the risk of cardiovascular decompensation and death, a decision was ultimately made to initiate therapeutic anticoagulation, accepting the risk of severe bleeding which could require management under general anesthesia. This strategy was felt to be safer than aspiration thrombectomy and inferior vena cava (IVC) filter placement given PERT’s concern that the stresses of a long procedure could precipitate acute cardiovascular decompensation in this patient.
A continuous unfractionated heparin (UFH) infusion was selected given its ability to be rapidly reversed with protamine sulfate. In an acute PE, UFH use with an activated partial thromboplastin time (aPTT) 1.5 to 2.5 times the upper limit of normal is considered to be therapeutic.11,12 Our hospital’s normal reference aPTT range is 25.1 to 36.5 seconds, making the suggested therapeutic anticoagulation range approximately 55 to 90 seconds. After much discussion, a more conservative aPTT goal of 55 to 65 seconds was chosen in an attempt to mitigate bleeding risk. The patient was monitored closely in the pediatric step-down unit and given humidified air via blow-by to prevent dessication of the tonsil beds.
A hypercoagulability workup revealed an elevated cardiolipin IgM of 22.4 MPL and low protein S at 52%, which were suggestive, yet not diagnostic for, anti-phospholipid syndrome. 13 All other coagulation studies, including homocysteine, B2 glycoprotein, cardiolipin IgG, factor V Leiden, lupus anticoagulant, and protein C serum levels were within normal range. There were no bleeding or further thromboembolic events during his hospital stay. On POD 13, he was transitioned from UFH to rivaroxaban, a novel oral anticoagulant (NOAC), and was discharged home in good condition on POD 18.
On POD 20, he presented to an outside hospital’s ED after multiple bouts of emesis containing clotted blood, along with headache, chest pain, and abdominal pain. He was found to have normal vital signs, a slightly low Hgb concentration (11.9 g/dL), and normal CT head. Upon transfer to our hospital, rivaroxaban was held and he was placed on an intravenous antihistamine for a presumed gastrointestinal bleed. Rivaroxaban was resumed the following day and he was discharged on POD 23.
From this point forward, his clinical status continued to improve. Repeat CT of his chest 6 months following initial hospitalization showed significant improvement in overall clot burden. To this day, he has not experienced any new thromboembolic or bleeding events. Due to his ongoing risk factor of morbid obesity, the decision to place him on lifelong rivaroxaban therapy was made by the Hematology team.
Discussion
This case highlights the lack of a therapeutic anticoagulation protocol when the need arises in the immediate post-tonsillectomy period and the importance of a multidisciplinary approach in the management of these complex scenarios. The concern for post-operative bleeding is not unique to tonsillectomy. The relative risk of bleeding has been described for elective orthopedic and cardiovascular procedures with similar bleeding risks as tonsillectomy.14,15 Unlike many cardiac or orthopedic patients, however, tonsillectomy patients are often young and very rarely require anticoagulation for any reason, which explains the lack of data on this topic.
The decision to anticoagulate must be tailored to the patient and clinical situation. In this patient’s case, management required input from Pediatric, Hematology, Cardiology, and Otolaryngology specialists. In acute DVT/PE, a critical factor in determining the importance of immediate anticoagulation therapy is a patient’s risk for acute cardiovascular decompensation. According to a recent systematic review and meta-analysis, patients with a PE-related syncope are at an increased risk of short-term death (11.2%) compared to patients who do not experience syncope (7%). In addition, PE patients who experience syncope are more likely to show RV strain on echocardiogram compared to those without syncope. 16 Our patient had both a syncopal episode and echocardiogram-confirmed RV strain, prompting strong consideration of immediate anticoagulation to help prevent clot propagation and/or re-embolization with potentially catastrophic decompensation.
There are no published data quantifying the additional risk of bleeding conferred by initiation of therapeutic anticoagulation in a treatment naïve patient, within a week of tonsillectomy. We would, however, suggest several logical measures if considering anticoagulating in the immediate post-tonsillectomy period, which we define as within 14 days of surgery. Figure 3 details these measures and lists considerations that should factor into the decision of whether to anticoagulate. Ultimately, the risk and consequence of a bleed must be weighed against the risk of cardiovascular decompensation. We propose that this decision should involve input from an Otolaryngologist, Cardiologist, and Hematologist at the very least.
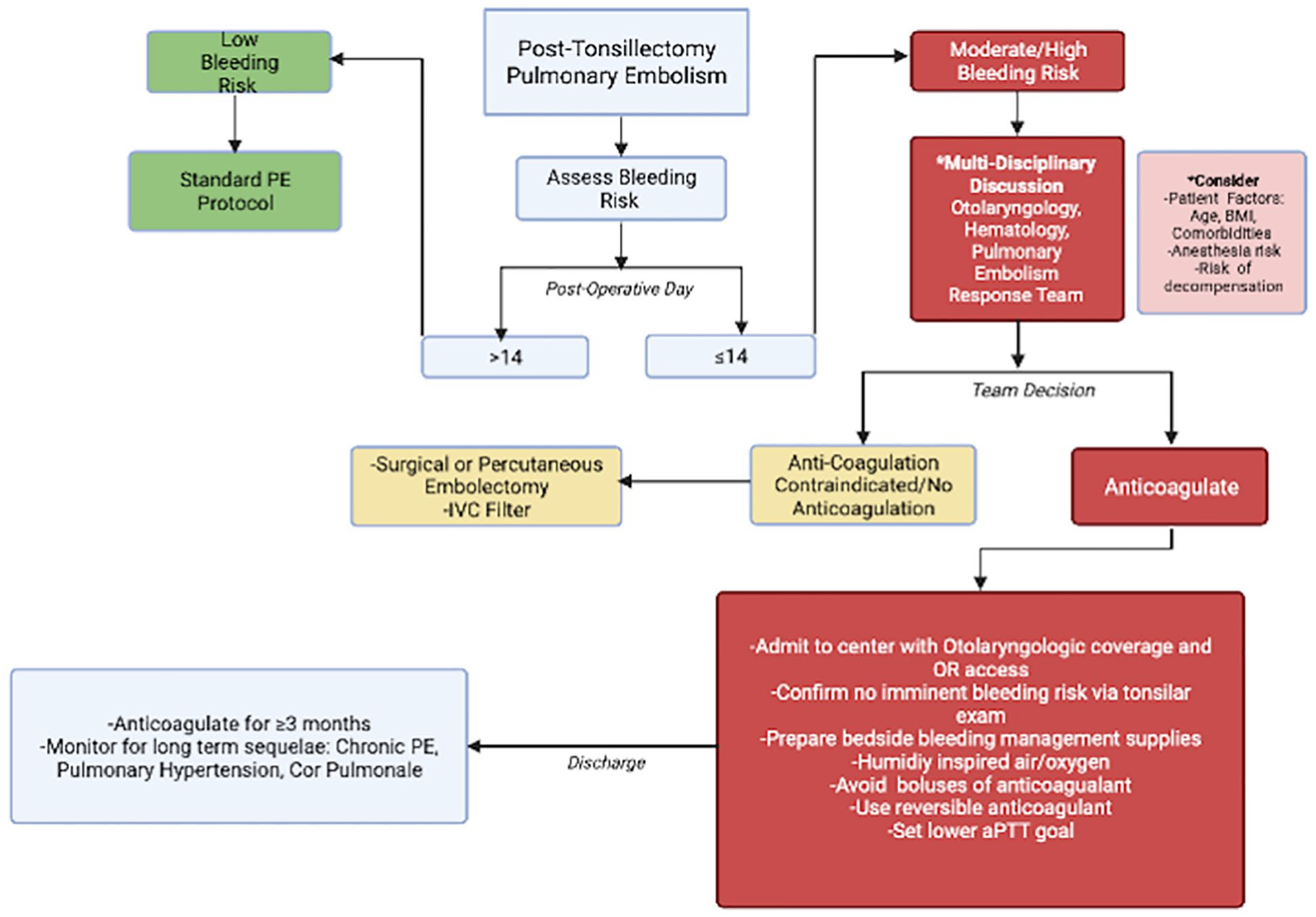
Suggested decision-making tree for the management of post-tonsillectomy pulmonary embolism (created with BioRender.com).
An initial examination of the tonsil beds by an Otolarynogologist is imperative. Ideally, one would find well-seated mature fibrin clots with no evidence of a new clotted blood or recent bleeding. If this is not the case, an increased risk of hemorrhage with the initiation of anticoagulation should be assumed. The postoperative timing should also be considered, keeping in mind that most tonsil bleeds occur between POD 5 and 10, which is the approximate time when the fibrin clots slough. 4 One should also take into account the increased risk of postoperative hemorrhage relative to age, with adolescents and adults showing greater risk of bleeding compared to younger children.17,18 Given that our patient was 17 years old and the size of a grown adult, he was considered to be at higher risk for a bleed compared to most pediatric patients.
Assessing the the patient’s fitness for surgery under general anesthesia is mandatory. According to one multi-institutional prospective study, the rate of PTH requiring surgical intervention ranges from 16% to 25%, depending on the age group. 17 In our patient’s case, there was concern about his cardiovascular fitness for general anesthesia in the event that surgical intervention to control hemorrhage was required. In addition, a percutaneous thrombectomy or inferior vena cava (IVC) filter placement, which would typically be a viable option for a patient with high bleeding risk, would also have carried an unacceptably large risk of acute decompensation. This was due to PERT’s concern about his cardiovascular ability to tolerate a 30 to 90 minutes procedure, along with the possibility of not being able to lay flat due to his morbid obesity. The risks associated with endovascular intervention were therefore weighed heavily into the management discussion, and ultimately both percutaneous thrombectomy and IVC filter placement were decided against.
The initial anticoagulants classically used in the acute management of DVT/PE include UFH and low molecular weight heparin (LMWH) given their short-acting nature. 19 We propose that the selected anticoagulant should be both short-acting and readily reversible to allow the option of scaling back the anticoagulation in the event of difficult-to-control hemorrhage. In addition, we would advise avoiding boluses of anticoagulation, given that this can increase the risk of bleeding due to an unintentional overshoot of the goal aPTT. 20 UFH is reversible with protamine sulfate and easily titratable to a specific aPTT goal in the inpatient setting. The use of UFH also allows tailoring the aPTT goals based on bleeding risk and fitness for operative management if the need arises. A case report by Cole et al discussed the management of a patient on long-term anticoagulation in the tonsillectomy perioperative period. The authors similarly used UFH as bridge therapy immediately following the procedure, with an aPTT goal of 1.5 to 2.3 times the control. They justified their decision of using UFH due to its greater evidence of complete neutralization with protamine, compared to that of LMWH. 21 It should be noted that UFH does carry risks in addition to bleeding, the most significant being a 0.1% to 5% risk of immunologically mediated heparin-induced thrombocytopenia. 22 NOACs can be considered in certain situations given their rapid onset of action, but would not have been ideal in our situation given that they can be difficult to titrate and their reversal agents are expensive. 23
If a patient begins anticoagulation within 14 days of tonsillectomy, we recommend admission to a hospital with 24-hour Otolaryngology coverage and operating room availability so that bleeding episodes can be dealt with swiftly. Basic measures may include humidified face mask/face tent to prevent dessication of the tonsil beds and a soft diet. Supplies should be kept on hand for bedside management of tonsil bleeding; these may include a Yankauer suction, headlamp, tongue depressors, cotton tonsil balls, oxymetazoline or phenylephrine nasal spray, and silver nitrate applicators. Fortunately, this patient’s outcome was positive despite a rare but severe complication of pediatric tonsillectomy.
Conclusion
While there is no literature guiding the approach to anticoagulation when necessary in the immediate post-tonsillectomy period, we were able to achieve a favorable outcome for our patient with a post-tonsillectomy massive PE through a multidisciplinary approach. If beginning anticoagulation within 14 days of tonsillectomy, the patient should be admitted to a hospital with Otolaryngology coverage and prophylactic steps should be taken, namely providing humidified air and a soft diet. A reversible and titratable anticoagulant should be used if possible, and consideration should be given to a sub-maximal anticoagulation goal depending on the specific circumstances. Ultimately, decisions need to be made on a case-by-case basis with input from the appropriate specialists to provide timely care in these unique and clinically challenging scenarios.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.