
Abstract
Rhinoplasty makes use of a combination of surgical techniques selected to address the specific requirements of each individual nose. Several different surgical techniques may be used for addressing each section of the nose, with possible different functional effects.
Objective:
The purpose of this investigation is to compare the functional effect of the different surgical techniques used for addressing each section of the nose.
Methods:
Prospective study of 57 consecutive rhinoplasty patients. Patients were evaluated with peak nasal inspiratory flow (PNIF), Nasal Obstruction Symptom Evaluation (NOSE), and Visual Analog Scale (VAS) for nasal obstruction before and 1 year after rhinoplasty. Additionally, esthetic evaluation of the nose was obtained with Rhinoplasty Outcomes Evaluation (ROE). According to the surgical technique used to address each portion of the nose, groups of patients were created and the functional improvement of these groups was compared.
Results:
Using the TukeyHSD multiple pairwise-comparison test, the estimated difference of the increase of PNIF between using spreader grafts and using spreader flaps was 94.9 (95% CI 24.3, 165.5, P = .004) between spreader grafts and neither grafts or flaps was 79.2 (95% CI 5.8, 152.6, P = .03), between spreader grafts and bilateral spreader flaps plus a unilateral spreader graft was 90.2 (95% CI 22.1, 158.2, P = .005). In all other portions of the nose, no significant difference was found in the functional improvement between different surgical techniques.
Conclusions:
Spreader grafts increase PNIF more significantly than other surgical techniques used for dorsal mid-vault reconstruction. Spreader grafts should be preferred over other techniques whenever an improvement of nasal airflow is required. No significant differences were found between the functional effect of alternative techniques used in other sections of the nose. Additional cohort studies will be necessary to further confirm data from this investigation.
Introduction
Rhinoplasty is a tailor-made procedure, as the surgical planning is individually designed to address each deformity of each section of the nose. From the armamentarium of available surgical techniques, the surgeon chooses the combination of techniques that better address the specific requirements of each individual nose. For every section of the nose there are several different surgical options that the surgeon may choose from. Though possibly achieving the same esthetic purpose or reinforcing the nasal section in a similar way, these alternative surgical techniques may have different effects to nasal breathing. The purpose of this investigation was to compare the functional effect of different surgical techniques used for addressing each portion of the nose. Specifically, this study investigated differences in the functional outcome of surgical techniques used for dorsal mid-vault reconstruction, for reinforcing tip support, for addressing the lateral crura and for reinforcing the alar contour. Surgical techniques used for dorsal mid-vault reconstruction may have different impact on the internal nasal valve (INV), therefore producing different functional outcomes. Likewise, techniques used for modifying the lateral crura or the alar contour as well as techniques reinforcing the tip support may have different effects on the external nasal valve (ENV), thereby having different functional outcomes. Knowledge of the functional effect of each specific surgical technique when compared to alternative techniques may be important for surgical planning.
Methods
Prospective study for evaluating the functional outcome of several rhinoplasty surgical techniques. The study design, data collection, and data treatment were approved by the Institutional Ethics Committee. Every patient included was made fully aware of the purpose and contents of the study and signed an Informed Consent.
This study included all patients submitted to rhinoplasty from January 1st of 2018 to December 31st of 2019 at a single institution and operated by a single surgeon (RX). Patients submitted to rhinoplasty during the same period but in whom additional nasal procedures were performed (such as turbinate reduction) were excluded. Patients under 16 years old were deferred from surgery and were not included.
Patients were evaluated before rhinoplasty and 1 year after surgery. This assessment included measurement of peak nasal inspiratory flow (PNIF), evaluation of nasal breathing through Nasal Obstruction Symptom Evaluation (NOSE) score, and Visual Analog Scale (VAS) score for nasal airway obstruction (NAO). Additionally, esthetic evaluation of the nose was obtained through Rhinoplasty Outcomes Evaluation (ROE) score.
NOSE is a disease-specific instrument for evaluating NAO. 1 A version validated for the Portuguese language 2 was used. VAS was obtained after asking the patient to score NAO at the moment of the consultation considering both sides of the nose together on a visual scale with 5 different marks. No NAO corresponds to 0 VAS score and total NAO to 100 VAS score. PNIF was measured according to its protocol. 3 A version of ROE4,5 validated for the Portuguese language 6 was used.
Statistical analysis evaluated differences between the pre-operative and the 1-year post-operative value in each scale. Separated analysis was done in patients with and without NAO and with and without septoplasty. Groups of patients were created based on the surgical technique used in each section of the nose. Based on the dorsal mid-vault reconstruction technique, 4 groups were created: patients with spreader flaps, with bilateral spreader grafts, with a combination of spreader flaps plus a unilateral spreader graft, and with none of the anterior. Spreader flaps were the primary option whenever a composite dorsal resection was done. Spreader flaps were used together with a unilateral spreader graft in cases of frontal asymmetry or deviation of the nasal pyramid for better alignment of the nasal pyramid. Bilateral spreader grafts were selected for straightening a deviated dorsal septum or for stabilization of an end-to-end SEG.
Based on the technique used for tip support, 4 groups were created: patients with septal extension graft (SEG), with tongue-in-groove suture (TIG), with columellar strut (CS), or with none of the prior. The selection of the surgical technique used for reinforcement of the nasal tip support was mainly based on esthetic evaluation of the facial balance, of the nasal length-projection ratio, of the ala-columella proportion, and of the height of the upper lip.
According to the surgical technique used on the lateral crura, 4 groups were created: patients with conservative cephalic trim, with cephalic turn-in, with lateral crural strut graft, and with lateral crural overlay. The functional role of caudal repositioning of lateral crura was also compared to patients in whom it was not used. Finally, the role of articulated alar rim grafts (AARG), as described by Ballin et al, 7 was also analyzed.
The selection of these surgical technique was decided in order to flatten the lateral crura and to improve the angle of both the short and long axis of the lateral crura as well as to provide a smooth alar-lobule transition.
Statistical analysis was made comparing functional improvements of the groups created for each section of the nose. Mean, standard deviations, quartiles, and maximum and minimum values were obtained for continuous data. Absolute frequencies were presented for categorical data. To check for differences between the various values measured on the baseline and after 1-year paired t-tests were employed. For 2 independent samples t-tests were used. ANOVA and non-parametric Kruskal-Wallis tests were used for comparisons between more than 2 independent samples. When differences were detected the Tukey multiple comparisons of means method was employed. The relative change percentage was obtained for PNIF, NOSE, and VAS values according to the following equation:

A significance level of α = .05 was used throughout the analysis. The R software package (2020) 8 was employed for all statistical analysis.
Results
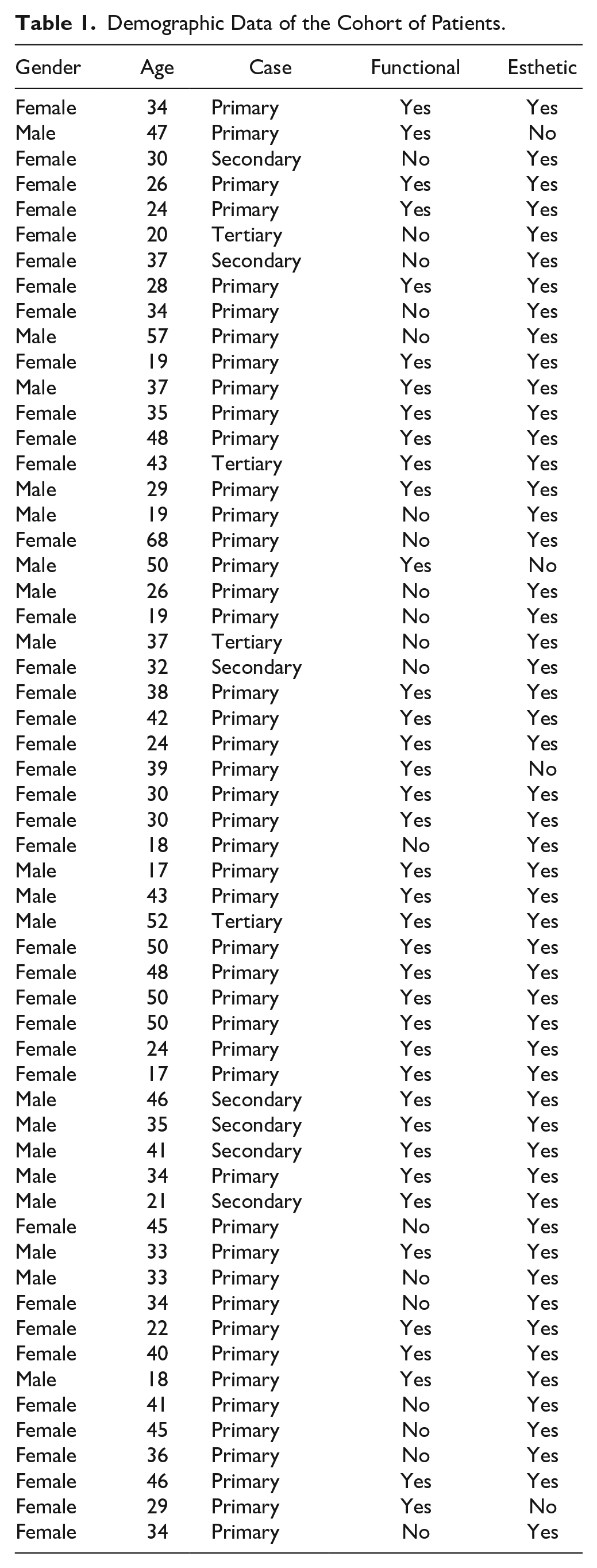
Fifty-seven Caucasian patients were studied. This series consisted of 38 women and 19 men, aged between 17 and 68 years old (mean 35.1 years old). Forty-six patients were primary rhinoplasty cases, 7 were secondary cases and 4 were tertiary rhinoplasty cases. Fifty-three patients were looking for an esthetic improvement of the nose, while 4 (all primary cases) only complained of NAO. In these 4 patients a functional rhinoplasty was performed after nasal valve obstruction was diagnosed. This diagnosis was clinically made after careful inspection of INV and ENV walls motion during normal and forced inspiration, together with a modified Cottle maneuver.
Of the 53 patients looking for esthetic improvement, 34 referred some impairment of nasal breathing (4 secondary and 2 tertiary cases). All revision cases wanted an esthetic improvement of the nose, with 4 secondary cases and 2 tertiary cases also seeking functional improvement. The complete demographic data of the cohort of patients is presented in Table 1.
Demographic Data of the Cohort of Patients.
All patients, primary or revision, were operated by using an open approach. Septal cartilage was the primary option for creating the required nasal grafts for each case. No auricular cartilage was used but autologous costal cartilage was harvested and used in 3 patients (2 secondary and 1 tertiary case).
Septoplasty was performed in 41 patients (extra-corporal in 3 patients): 27 patients with both functional and esthetic complaints, 4 with NAO only, and 10 patients with purely esthetic motivation but in whom a significant septal deviation was found. No septal correction was done in 16 patients, although the septum may have been approached for cartilage harvesting.
Composite dorsal resection (split-hump reduction) was done in 46 patients. Spreader flaps were used in 16 patients, bilateral spreader grafts in 5 patients, a combination of spreader flaps plus a unilateral spreader graft in 24 patients while in 12 patients no spreaders were used. A SEG was used in 25 patients, TIG in 23 patients, and CS in 5 patients. As to the lateral crura, a turn-in flap was done in 12 patients, strut graft was used in 7 patients, overlay in 11 patients, and cephalic trim in 27 patients. Caudal repositioning of the lateral crura was performed in 8 patients and an AARG was used in 5 patients.
Data from nasal breathing evaluation (NOSE, VAS, and PNIF) and esthetic evaluation (ROE) before surgery and 1 year after rhinoplasty are given in Table 2. There was a statistically significant improvement in NOSE (−34.9, 95% CI −42.2, −27.6, P < .001), VAS (−44.1, 95% CI −53.2, −35.0, P < .001), and PNIF (36.6, 95% CI 28.7, 44.5, P < .001) after rhinoplasty. A significant improvement was verified in the groups of patients with and without NAO before surgery (Table 2).
Mean and Standard Deviation of NOSE, VAS, PNIF, and ROE Values on the Baseline and After 1 year by the Presence/Absence of Functional Symptoms.
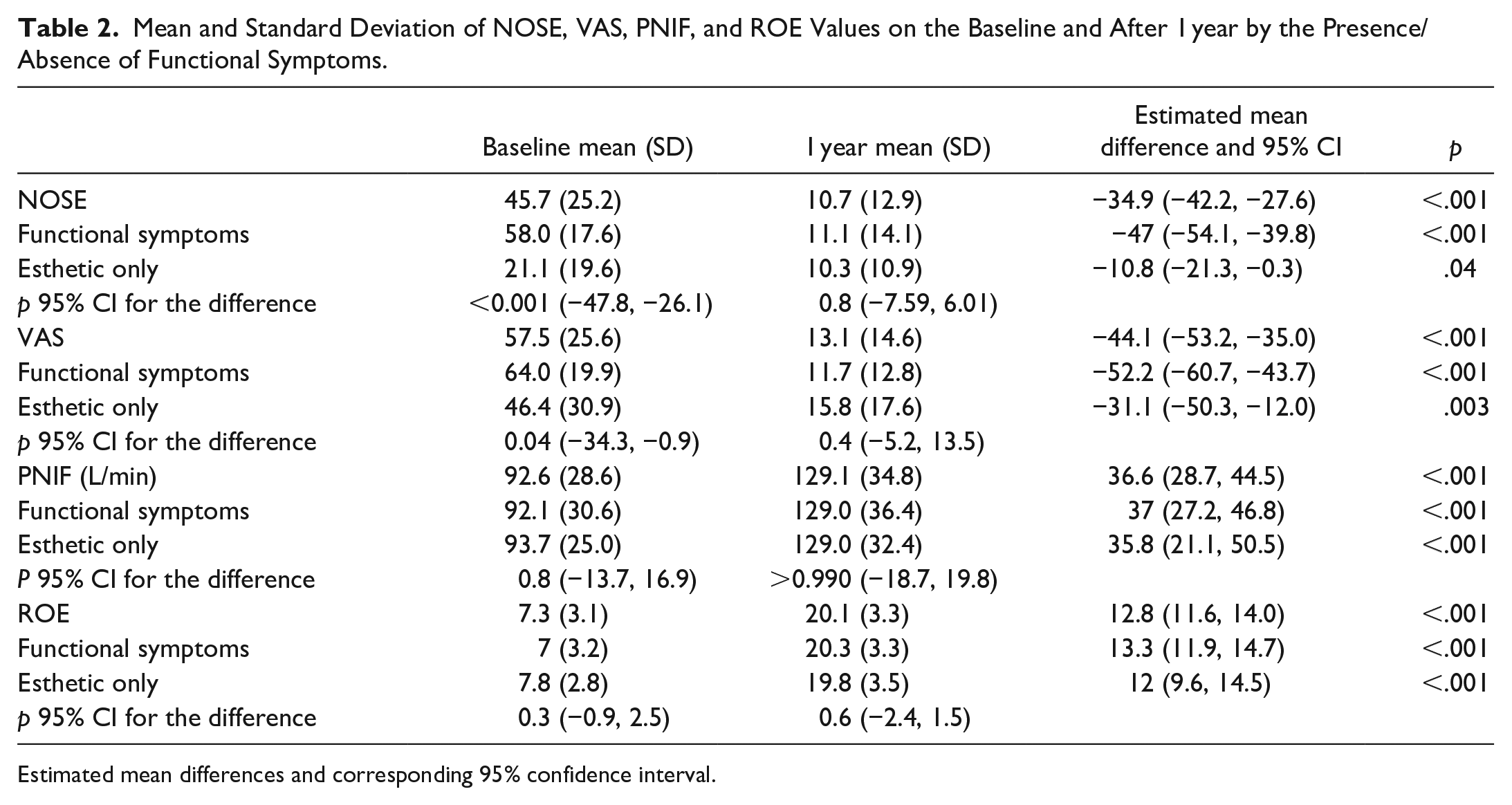
Estimated mean differences and corresponding 95% confidence interval.
Data from patient-reported esthetic appreciation of the nose (ROE) are given in Table 2. There was a significant improvement in ROE score after rhinoplasty (12.8, 95% CI 11.6, 14.0, P < .001).
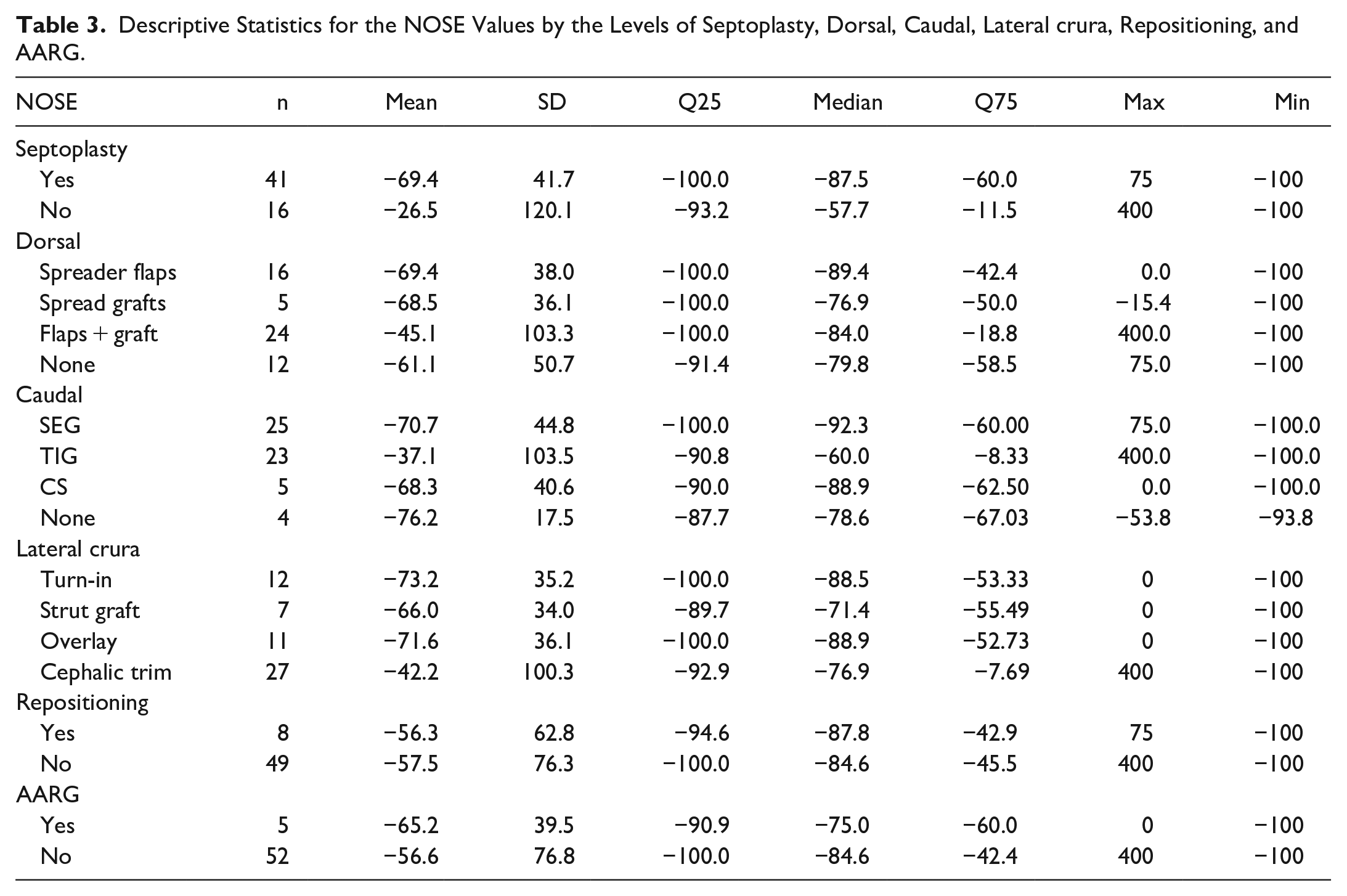
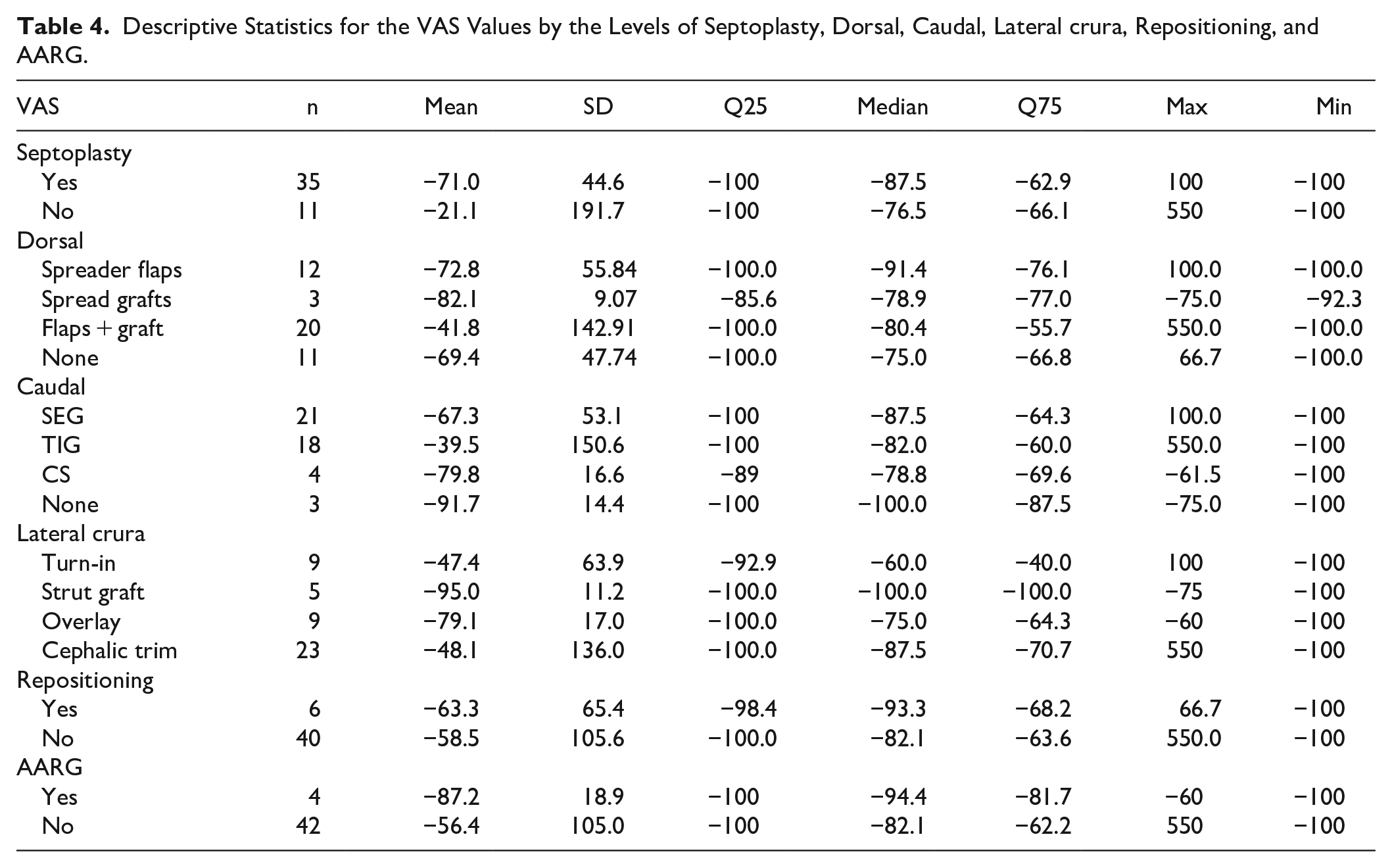
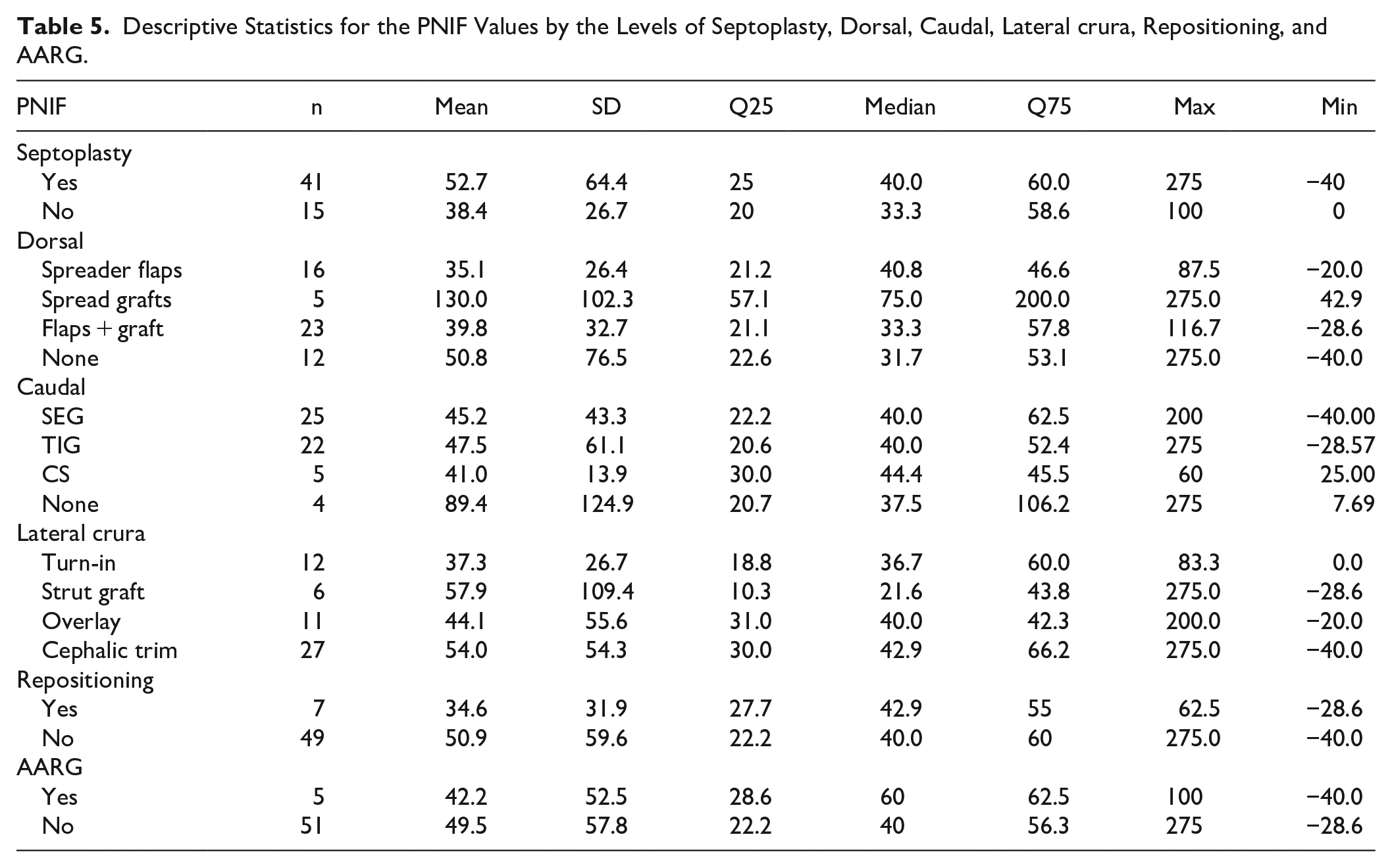
Data of the analysis made for the difference of improvement verified after rhinoplasty for the different surgical techniques used in each section of the nose are given in Tables 3 to 5. A significant difference was found in PNIF improvement between the group with bilateral spreader grafts and groups with other techniques for dorsal mid-vault reconstruction (Figure 1). Using the TukeyHSD multiple pairwise-comparison test, the estimated difference of relative change of PNIF between spreader grafts and neither grafts or flaps was 79.2 (95% CI 5.8, 152.6, P = .03), between spreader grafts and spreader flaps the estimated difference was 94.9 (95% CI 24.3, 165.5, P = .004), and between spreader grafts and the combination of spreader flaps plus a unilateral spreader graft the estimated difference was 90.2 (95% CI 22.1, 158.2, P = .005). For all other portions of the nose there was no significant difference in the functional improvement between groups (Tables 3-5).
Descriptive Statistics for the NOSE Values by the Levels of Septoplasty, Dorsal, Caudal, Lateral crura, Repositioning, and AARG.
Descriptive Statistics for the VAS Values by the Levels of Septoplasty, Dorsal, Caudal, Lateral crura, Repositioning, and AARG.
Descriptive Statistics for the PNIF Values by the Levels of Septoplasty, Dorsal, Caudal, Lateral crura, Repositioning, and AARG.
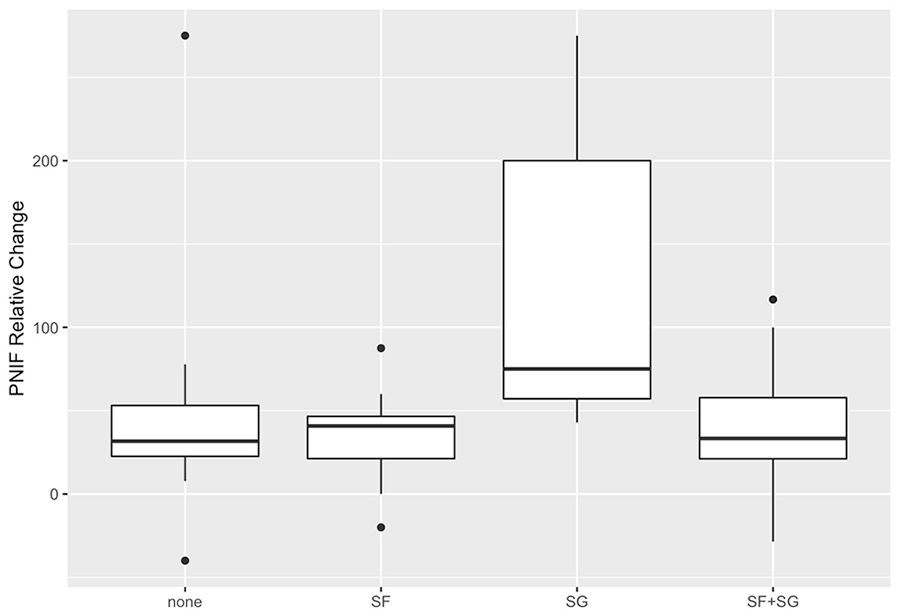
PNIF relative change of alternative techniques used for dorsal mid-vault reconstruction (P = .006).
Discussion
The purpose of rhinoplasty is to improve nasal esthetics and nasal breathing. Though not every patient undergoing surgery has both esthetic and functional complaints, rhinoplasty should be able to refine the esthetic look of the nose and to improve nasal breathing. This study demonstrates that rhinoplasty leads to a significant improvement of both nasal esthetics and nasal breathing. All patient-reported scores used in this study for assessing nasal appearance and nasal breathing as well as PNIF significantly increased after rhinoplasty.
Nasal appearance was perceived by patients as substantially improved by surgery, as the significant increase verified in ROE indicates (Table 2). A ROE score of 12 has been defined by Izu et al 9 as the minimum normality limit, with sensitivity and specificity of 95%. In the present study, the mean ROE score changed from 7.3 before surgery to 20.1 after rhinoplasty. The improvement of nasal appearance achieved by rhinoplasty found by our study has also been demonstrated by other studies.10-14
Nasal breathing sensation and PNIF value were also significantly improved by rhinoplasty. This improvement was verified in patients with NAO and in patients with an esthetic-only motivation for rhinoplasty (Table 2).
Both the preoperative NOSE and VAS scores were significantly different in the groups of patients with functional complaints and with a purely esthetic motivation for undergoing rhinoplasty (Table 2), corroborating the value of these evaluation instruments on identifying patients with NAO. Interestingly, these scores were significantly improved by rhinoplasty in both groups of patients. Moreover, after surgery the difference in NOSE and VAS scores between patients with and without pre-operative functional complaints is no longer statistically significant (Table 2). These findings are in line with other studies which demonstrated an improvement in nasal breathing following functional rhinoplasty15,16 or rhinoplasty.17-20
In this study PNIF significantly increased after rhinoplasty both in patients with and without NAO. Interestingly, there was no significant difference in the pre-operative PNIF value between these 2 groups (Table 2). This finding confirms the lack of relevant correlation between nasal airflow and patient-reported assessment of nasal breathing demonstrated by several studies21-29 and is probably related to the multifactorial nature of nasal breathing sensation, which is related to but not solely dependent on nasal airflow. It has been demonstrated that low airflow prevents the sensation of suitable nasal breathing, 27 but patients with and without sensation of suitable nasal breathing may have similar levels of airflow.
The results of this study demonstrate that rhinoplasty improves nasal breathing in patients not requiring septal correction. Functional improvement was higher in patients with septoplasty when compared to patients with no septal correction, but the difference was not significant in any of the instruments (NOSE, VAS, or PNIF) used (Tables 3-5). This suggests that techniques used in rhinoplasty other than septoplasty may improve nasal breathing, as also found by other studies.9,15-20 In fact, surgical planning in rhinoplasty is individually tailored in order to address the specific requirements of each patient, and not every patient requires septal correction. Surgical techniques that augment the patency or increase the resilience of INV and of ENV are commonly used in rhinoplasty, either for a functional purpose or for achieving an esthetic improvement of the nasal contour, in any case with a likely functional effect.
For addressing each section of the nose several different surgical techniques are available for the surgeon to choose from. Often, these different surgical techniques achieve similar esthetic outcomes or provide identical reinforcement of the nasal section. The functional effect of these various techniques, however, may be different. Knowledge of the comparative functional effect of these techniques may assist the surgeon in surgical planning, particularly when functional improvement is required. The present study specifically investigated the functional role of various techniques used for dorsal reconstruction, which, despite producing similar stabilization of the mid nasal dorsum, may have different impacts on INV functioning. Likewise, this study compared the functional role of surgical techniques used for reinforcing nasal tip support, for dealing with the lateral crura of the lower lateral cartilages, and for reinforcing the alar contour. These techniques may allow similar esthetic outcomes, yet may produce different changes in the ENV, thereby leading to different functional outcomes of rhinoplasty.
This investigation demonstrated that bilateral spreader grafts produce a significantly higher increase of PNIF when compared to spreader flaps, to a combination of spreader flaps plus a unilateral spreader graft or to none of these (Figure 1). Though being expected from their effect on nasal valve widening, the functional role of spreader grafts has not consensus, with some studies demonstrating an improvement of nasal breathing30-32 while other studies could not demonstrate consistent functional benefits.20,33-36 Modifications of spreader grafts have been proposed to improve their functional effect37,38 and additional techniques, such as the flaring suture 39 or the splay graft 40 have been suggested for the same purpose.
Zeid et al 41 compared nasal airway resistance before and after rhinoplasty using spreader flaps or spreader grafts and concluded that both techniques decreased nasal airway resistance without significant difference between the 2 techniques. Sowder et al 42 and Bilgin et al 31 also compared the functional effect of spreader flaps and spreader grafts using NOSE score and found no significant difference between the 2 techniques. The results of our investigation do not corroborate these studies, as the functional effect of spreader grafts was significantly higher than the effect of spreader flaps. Though both techniques will provide support to the mid-nasal vault and prevent long-term esthetic deformities, spreader grafts will probably widen the nasal valve more significantly than spreader flaps due to the difference in thickness between flaps and grafts. Using acoustic rhinometry, Saedi et al 43 studied the effect of spreader flaps on the minimal cross-section area of the nasal airway after reduction rhinoplasty and concluded that there was no significant difference to patients in whom spreader flaps had not been used. Furthermore, it was also found that patient-reported assessment of nasal breathing with VAS was not significantly different to when no flaps had been used. 43 In a previous study our group investigated possible correlations between several nasal airway dimensions and nasal airflow and have found nasal valve area to statistically correlate with PNIF value. 44 Interestingly, the results of the present investigation further corroborate the findings of that study and reinforce existing data supporting the functional role of spreader grafts. Therefore, the current trend for using spreader flaps instead of grafts in primary rhinoplasty may not be advised when a functional improvement is required. It must be acknowledged, though, that in this study spreader grafts were used for fixating an end-to-end SEG and for straightening a deviated dorsal septum; a deviated dorsal septum could cause impairment of the INV on the side of deviation, therefore possibly introducing a bias in the comparison of the functional effect between spreader flaps and grafts.
Reinforcing nasal tip support may prevent long-term modifications of the nasal tip. Both SEG and TIG are believed to provide stronger support to the nasal tip than CS. Erol et al 45 calculated the tip support provided by TIG and concluded that it was significantly more marked than the support provided by CS. Sawh-Martinez et al 46 demonstrated that SEG provided maintenance of tip rotation more efficiently than a CS, though with no differences in tip projection. A solid tip support is presumed to be important also for ENV functions and, therefore, SEG and TIG would be expected to have a more marked functional effect than CS. Nevertheless, the results of our study could find no significant difference in the functional improvement provided by SEG, TIG, or CS. These results agree with a recent study by Patel et al, 47 that did not find any functional effect of SEG when assessed through NOSE, VAS or Standardized Cosmesis and Health Nasal Outcomes Survey obstruction score (SCHNOS-O). This lack of functional effect was verified both in esthetic rhinoplasty and in combined functional and esthetic rhinoplasty. 47
Studying on cadaver specimens, Vachhani et al 48 found lateral crura stiffness to be higher after lateral crural strut graft than after cephalic turn-in and higher after cephalic turn-in than after cephalic resection. Another study, by Tellioglu and Cimen, 49 found lateral crural turn-in to be esthetically as effective as cephalic resection but providing reinforcement of the functional properties of the lateral crus. Recker and Hamilton 50 stated that reinforcing weak lateral crura or straightening concave or convex lateral crura with lateral crural strut grafts corrects ENV impairment and leads to functional improvement of the nose. The findings of these studies are coherent, as both strut grafts and turn-in flaps create double-layered cartilages throughout the extent of the lateral crura, though strut grafts, usually made from thicker septal cartilage, will probably increase resilience to a further extent. Also studying on cadaver cartilages, Insalaco et al 51 found lateral crural overlay to increase strength and resilience of lateral crura, which should account for a better ENV function. Lateral crural overlay doubles cartilage thickness, but only on a limited extent of the crura. A recent study by Abdelwahab et al has found that both lateral crural strut graft and overlay improve ENV patency, which was not verified with cephalic turn-in or trimming. 52 The results of our study, though, could not find significant difference between the functional effect of lateral crural turn-in, strut graft, overlay or cephalic trim.
Cephalic malposition of lateral crura is a frequent finding in the Caucasian population. 53 This cephalic malposition has been demonstrated to cause ENV insufficiency. 54 Ilhan et al, 55 studying the long-term effects of caudal repositioning of the lateral crura, found both an esthetic and functional improvement, as assessed by ROE and by NOSE. Consequences of cephalic malposition were also discussed by Hamilton 56 and by Yeh and Williams EF, 57 who underlined the propensity of patients with cephalic malposition to NAO due to ENV impairment. According to Silva, 54 the alar contour void created by cephalic malposition should be addressed by structuring ENV walls. It would, thus, be expected that AARG or caudal repositioning of the lateral crura would have functional effect, by correcting this void. However, the findings of our investigation did not validate this assumption as no significant functional benefit was noted with either technique.
Previous investigations have focused on functional and esthetic results of rhinoplasty. The present study provides a detailed comparative analysis of the functional effect of surgical techniques available for each section of the nose. In addition, this study was able to incorporate multiple subjective and objective outcome measures.
Limitations of the Study
This is a single-surgeon study with a limited number of patients and, therefore, more studies are warranted to further confirm the results obtained. Comparing functional results achieved with different surgical techniques is tricky, as the selection of the surgical technique is dictated by the deformity. Several surgical techniques were used in combination in each patient, hampering assignment of functional changes to each technique. Nevertheless, proper selection of statistical tests, including the TukeyHSD multiple pairwise-comparison test, allowed significant differences to be found in the data obtained from this investigation.
Conclusions
Spreader grafts increase PNIF more significantly than other surgical techniques used for dorsal mid-vault reconstruction. Spreader grafts should be preferred over other techniques whenever an improvement of nasal airflow is required. No significant differences were found between the functional effect of alternative techniques used in other sections of the nose. Additional cohort studies will be necessary to further confirm data from this investigation.
Footnotes
Authors’ Note
▪ All procedures performed were in accordance with the ethical standards of the Institutional Research Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
▪ For this study a signed informed consent was obtained from every patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.