
Abstract
Objectives:
To evaluate clinical characteristics and outcomes of patients diagnosed with anterior (ASB) or lateral skull base (LSB) spontaneous cerebrospinal fluid (sCSF) leak.
Methods:
Single center retrospective review of patients diagnosed with sCSF leaks of ASB or LSB between 1/1/2009 and 11/1/2019 (n = 69). Body mass index (BMI), gender, age at diagnosis, origin of CSF leak (ASB vs LSB), surgical approach, lumbar drain use, recurrence, pre-operative diagnosis of diabetes mellitus (DM), and obstructive sleep apnea (OSA) were collected.
Results:
69 patients included in this study met criteria for sCSF leak without a traumatic or iatrogenic cause (Female: 51 (74%); average BMI: 37.0 ± 7.9). Forty-eight (70.0%) presented with sCSF leaks of the lateral skull base. All ASB leaks were treated with an endoscopic transnasal approach. Eleven (22.9%) LSB leak patients were treated using transmastoid approaches and 35 (72.9%) patients with a middle cranial fossa approach. Eleven patients (15.9%) reported sCSF leak recurrence. Two patients (9.5%) with anterior skull base and 9 patients (18.8%) with lateral skull base leaks had recurrence. LSB sCSF leaks had a relative risk of 2.192 of recurrence compared to ASB leaks (95% CI: 0.431-11.157, P = .483). A 5.017 times increased risk (95% CI: 1.285-19.583, P = .020) was reported for patients with OSA, while the risks for DM and BMI were 1.351 (95% CI: 0.67-9.105, P = .177) and 1.026 (95% CI: 0.963-1.094, P = .426) respectively. Patients with sCSF leak recurrence had significantly lower lumbar drain use (33.3%) than those without recurrence (72.7%) (P = .049).
Conclusion:
Spontaneous CSF leak recurrence is complex and multifactorial, and while patients with both DM and OSA had the higher risk of recurrence, OSA is likely an independent clinical risk factor for sCSF leak recurrence in this patient population.
Introduction
A cerebrospinal fluid (CSF) leakage results from a skull base dural defect that permits CSF communication between the cranial vault and sinonasal or tympanomastoid cavities. 1 CSF leaks from the skull base most often result from trauma, infection, or skull base surgery as well as congenital encephaloceles or intracranial tumors.2,3 However, spontaneous CSF (sCSF) leaks are a consequence of defects in the dura and skull base that are currently believed to be idiopathic in nature.
Spontaneous CSF leaks have been associated with obesity. Studies demonstrate an increased prevalence of sCSF leaks in accordance with the rising rates of obesity in the United States, and that females are more frequently affected than males.4-6 Hypotheses suggest that intracranial hypertension results in the skull base erosion through persistent, pulsatile, high-pressure CSF. 7 Spontaneous CSF leaks, obesity, obstructive sleep apnea (OSA), and intracranial hypertension have been shown to be interrelated. Longitudinal studies have demonstrated that the most common sites of sCSF leak are the cribriform plate, lateral sphenoid sinus/sphenoid lateral pterygoid recess, ethmoid roof, and tegmen tympani; all of which are relatively thin portions of the skull base.8-13 Although sCSF leaks may occur in the anterior or lateral skull base, these are likely a manifestation of the same disease process.
Unlike traumatic CSF leaks, sCSF leaks are unlikely to resolve spontaneously. The common surgical approaches for lateral skull base sCSF treatment are the middle cranial fossa (MCF), transmastoid, and combined approaches.14,15 While currently there is no consensus on which technique is more effective, the MCF approach allows for better visualization of the tegmen tympani, which may be helpful in repairing larger and more anterior defects.16,17 The transmastoid approach is less invasive as it avoids craniotomy while offering good visualization of the mastoid tegmen and posterior fossa plate. 18 For anterior skull base defects, endoscopic transnasal approaches are effective in offering definitive treatment for sCSF leaks when conservative measures fail.10,19 Lumbar drains can be used when post-operative otorrhea or CSF rhinorrhea persists; however, this method is somewhat controversial. 7 Some providers suggest that lumbar drains decrease pressure on the site of the repair by diverting CSF. However, there is little evidence that lumbar drains prevent leak recurrence.20,21
As obesity continues to rise, it becomes increasingly important to better understand the risk factors that are predictive of recurrent sCSF leaks. This study aims to explore patient characteristics that are predictive recurrent sCSF leaks.
Materials and Methods
Study Design
This is a single institution retrospective review of patient records of individuals diagnosed with anterior and lateral skull base spontaneous CSF leaks at a tertiary referral center between 1/1/2009 and 11/1/2019 (n = 69). The study was approved by the Institutional Review Board (IRB) STUDY20190451.
Study Population
Study participants were identified using a 2-step process. Three hundred ninety-two patients at a single academic institution were selected using the ICD-10 diagnosis code G96.0 or ICD-9 codes of 339.8, 348.4, 349.0, 792.0 for CSF leak as potential candidates. Individual patient charts were reviewed to confirm the diagnosis of sCSF leak, defined by evidence of beta 2 transferrin positive otorrhea or rhinorrhea in the absence of possible traumatic, iatrogenic, or other secondary cause. Out of 392 patients, 89 did not have beta-2 transferrin confirmed CSF leak, 193 patients had surgical causes for a CSF leak, 37 patients had traumatic cause of CSF leak, and 4 patients had insufficient documentation of comorbidities and treatment. The final cohort included 69 patients between the ages of 18 and 89 with sCSF leaks. Variables collected included body mass index (BMI), gender, age at diagnosis, site of CSF leak (anterior skull base (ASB) or lateral skull base (LSB)), and recurrence. Surgical approach and use of lumbar drains were also recorded. CSF leak recurrence was defined as a diagnosis of sCSF leak following initial repair, in the same location as the original leak, with signs of dehiscence on computed tomography (CT) and a positive beta-2 transferrin test result. The diagnosis of Idiopathic Intracranial Hypertension (IIH) was determined by papilledema on an ophthalmology exam or elevated opening pressure on lumbar puncture. Opening pressures of above 25 cm H2O were defined as elevated. Patients with prior IIH diagnosis as noted in otolaryngology or neurology charts were also noted. Diabetes mellitus (DM) and obstructive sleep apnea (OSA) status were collected and determined by presence of each diagnosis in otolaryngology and primary care documentation.
Surgical Method and Post-Surgical Management
All ASB leaks were repaired using an endoscopic transnasal approach using nasoseptal flap and fat graft. This method of repair has demonstrated excellent results in providing robust anterior skull base closure, especially in patients with sCSF leaks that are at higher risk of recurrence. LSB leaks were repaired using MCF, transmastoid, or combined approaches. Lateral skull base approach was determined by the size and location of the defect. The transmastoid approach was used when the defect was small and lateral to the ossicular chain. When the defect involved the epitympanum and was medial to the ossicles, an MCF approach was preferred by all surgeons in the study.
Lumbar drains (LD) were used to manage elevated intracranial pressures contributing to CSF leaks or to reduce intracranial pressures during repair of skull base defects. While more recent practices indicate that some surgeons use a LD for all sCSF leaks, LD use remains controversial. At this institution surgeons earlier in the study period were more likely to use LD in patients with persistently elevated intercranial pressure despite mannitol administration, patients with high flow CSF leaks, large skull base defects, and very obese patients with high central venous pressure or those with multiple defects. When used, lumbar drains were placed for 2 to 5 days, and clamped for 24 hour prior to removal.
Statistical Methods
Demographic and clinical characteristics were evaluated using means with standard deviations, medians with interquartile ranges (IQR) for continuous variables, and frequencies for categorical variables. Continuous variables were compared using Mann-Whitney U tests and categorical variables were compared using Fisher’s exact tests due to low sample size. Complication rate among different surgical treatment groups was compared using chi-square tests. Additional comparisons among patient groups were performed using independent sample t-tests or chi-square tests. Odds ratios were used to evaluate the likelihood of CSF leak recurrence based on comorbidity status. Multivariate logistic regression was utilized to assess the contribution of comorbidities on the recurrence of CSF leaks while controlling for other variables. The regression included the evaluation of the effects of OSA and DM diagnoses as categorical variables, and BMI as a continuous variable, using leak recurrence as a binary outcome. Wald’s tests were used to assess P-values for odds ratios (OR). All analyses were performed using R version 3.3.3 (R Foundation, 2017). P values less than .05 were considered statistically significant.
Results
A total of 69 patients met criteria for spontaneous CSF leak and were included in the present study. Of these patients, 51 (73.9%) were female with an average age of 57.9 ± 12.8 years. The average BMI was 37.0 ± 7.9. Age was not different between men (60.9 ± 8.5) and women (56.6 ± 14.0) but men had lower BMI on average when compared to women (32.9 ± 5.8 vs 38.8 ± 8.0; P = .001). Twenty-one (30.4%) patients presented with a sCSF leak of the anterior skull base while 48 (69.6%) had lateral skull base leaks (no cribriform defects). All ASB leak patients were evaluated with MRI or CT scan with 9 (42.8%) patients having evidence of sphenoid skull base defects, 3 (14.3%) patients had evidence of cribriform defects, 2 (9.5%) patients have medial lamella defects, 1 (4.8%) had a posterior ethmoid defect, 1 (4.7%) had a fovea ethmoidalis defect, 5 (23.8%) patients did not have clear evidence of a skull base defect on CT or MRI. All LSB leak patients had CT scan or operative findings of tegmen tympani or mastoid defects. Fifteen patients had a diagnosis of IIH (21.7%), 25 (36.2%) presented with DM and 22 (31.8%) presented with OSA. Ten patients had both OSA and DM while 2 patients had both OSA and IIH. Thirteen patients (18.8%) were managed with Diamox, 4 (5.8%) received ventriculoperitoneal shunts, and 1 patient (1.4%) received bariatric surgery following sCSF leak repair. Eleven patients (15.9%) reported a sCSF leak recurrence after initial surgical correction. Two patients (9.5%) with ASB leaks had recurrence while 9 patients (18.8%) with LSB leaks had recurrence. LSB sCSF leaks had a nonsignificant 2.192 increased risk of recurrence compared to anterior skull base leaks (95% CI:0.431-11.157, P = .483). Recurrence occurred between 1 and 84 months (average of 27.9 months) following initial surgery. Average follow up time after second repair was 13.2 ± 6.8 months.
Demographics and comorbidities of recurrent and nonrecurrent sCSF leak patients were compared (Table 1). Of those that experienced recurrence, 7 (63.5%) had OSA whereas 15 (25.9%) of those without recurrence were diagnosed with OSA (P = .029). OSA was the only significant individual predictor of sCSF leak recurrence. Patients with OSA had similar BMIs to those without OSA (39.27 ± 7.0 vs 35.92 ± 8.3, P = .103). All patients had CT or MRI imaging and 50 (72.5%) had evidence of encephalocele or meningoencephalocele on imaging. The presence of encephaloceles (P = .162) and multiple defects at the site of the leak (P = .237) were not associated with recurrence.
Demographics, Comorbidities, and Outcomes of sCSF Leak Patients Divided by Recurrent sCSF Leak Status.
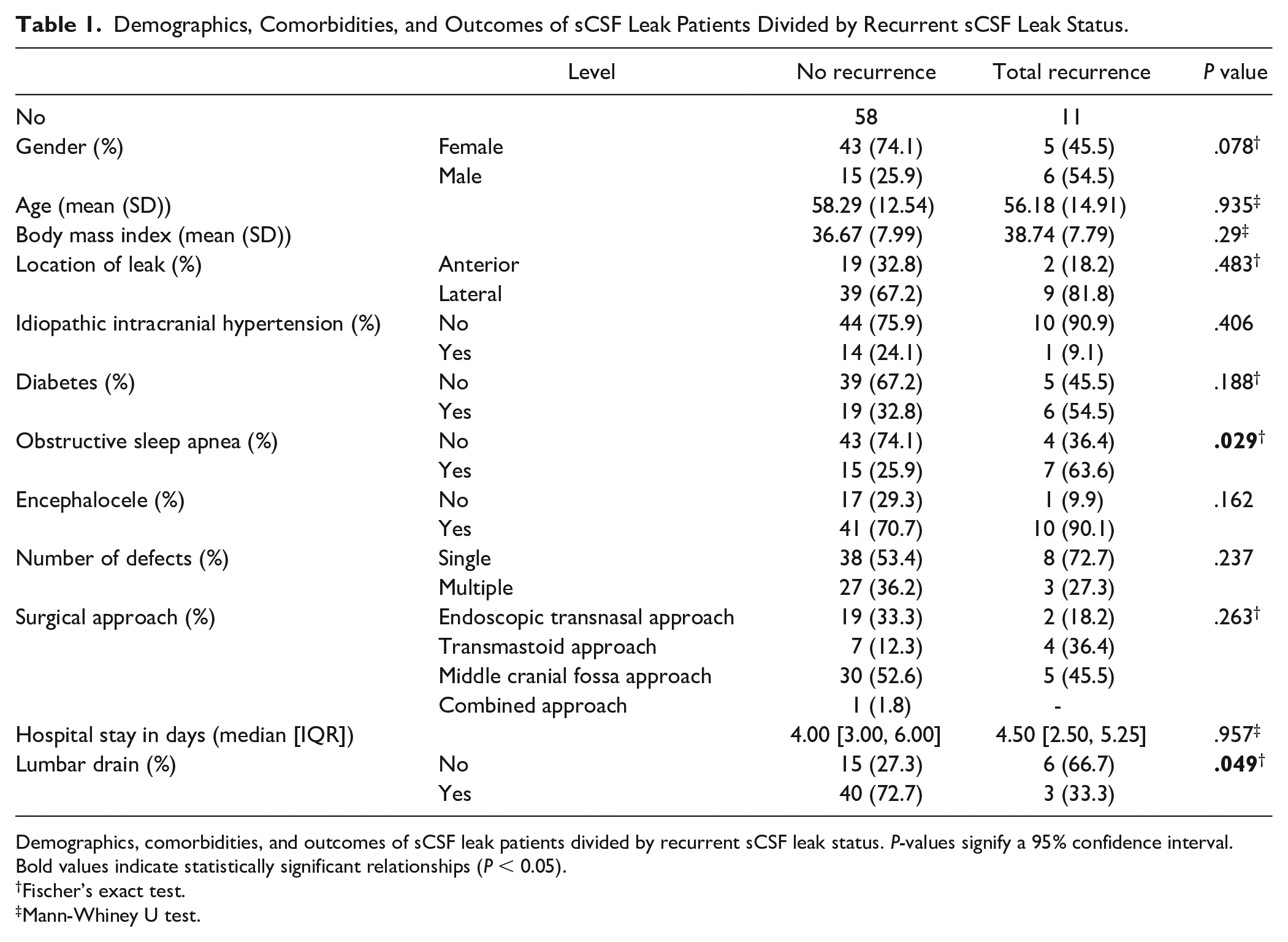
Demographics, comorbidities, and outcomes of sCSF leak patients divided by recurrent sCSF leak status. P-values signify a 95% confidence interval. Bold values indicate statistically significant relationships (P < 0.05).
Fischer’s exact test.
Mann-Whiney U test.
The contribution for each comorbidity toward leak recurrence was determined using odds ratios (OR) (Table 2). The OR of a CSF leak recurrence in patients with OSA was 5.017 (95% CI = 1.285-19.583, P = .020). DM increased risk for leak recurrence by 2.46351 (95% CI = 0.666-9.105, P = .188) while BMI increased the risk for leak recurrence by 1.026 (95% CI = 0.963-1.094, P = .290), neither of which were statistically significant. Of the 10 patients with both OSA and DM 50% had a recurrence of sCSF leak, more than the patients with only OSA (16.7%), only DM (6.3%), or neither comorbidity (8.6%) (P = .021) (Figure 1).
Univariate Odds Ratios for OSA, DM, and BMI Contributions to sCSF Leak Recurrence.
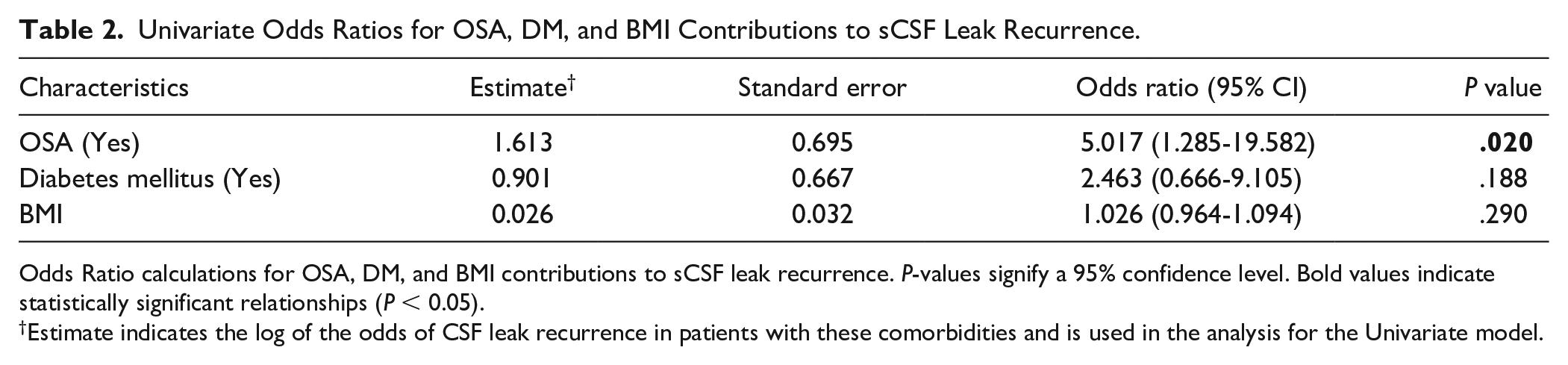
Odds Ratio calculations for OSA, DM, and BMI contributions to sCSF leak recurrence. P-values signify a 95% confidence level. Bold values indicate statistically significant relationships (P < 0.05).
Estimate indicates the log of the odds of CSF leak recurrence in patients with these comorbidities and is used in the analysis for the Univariate model.
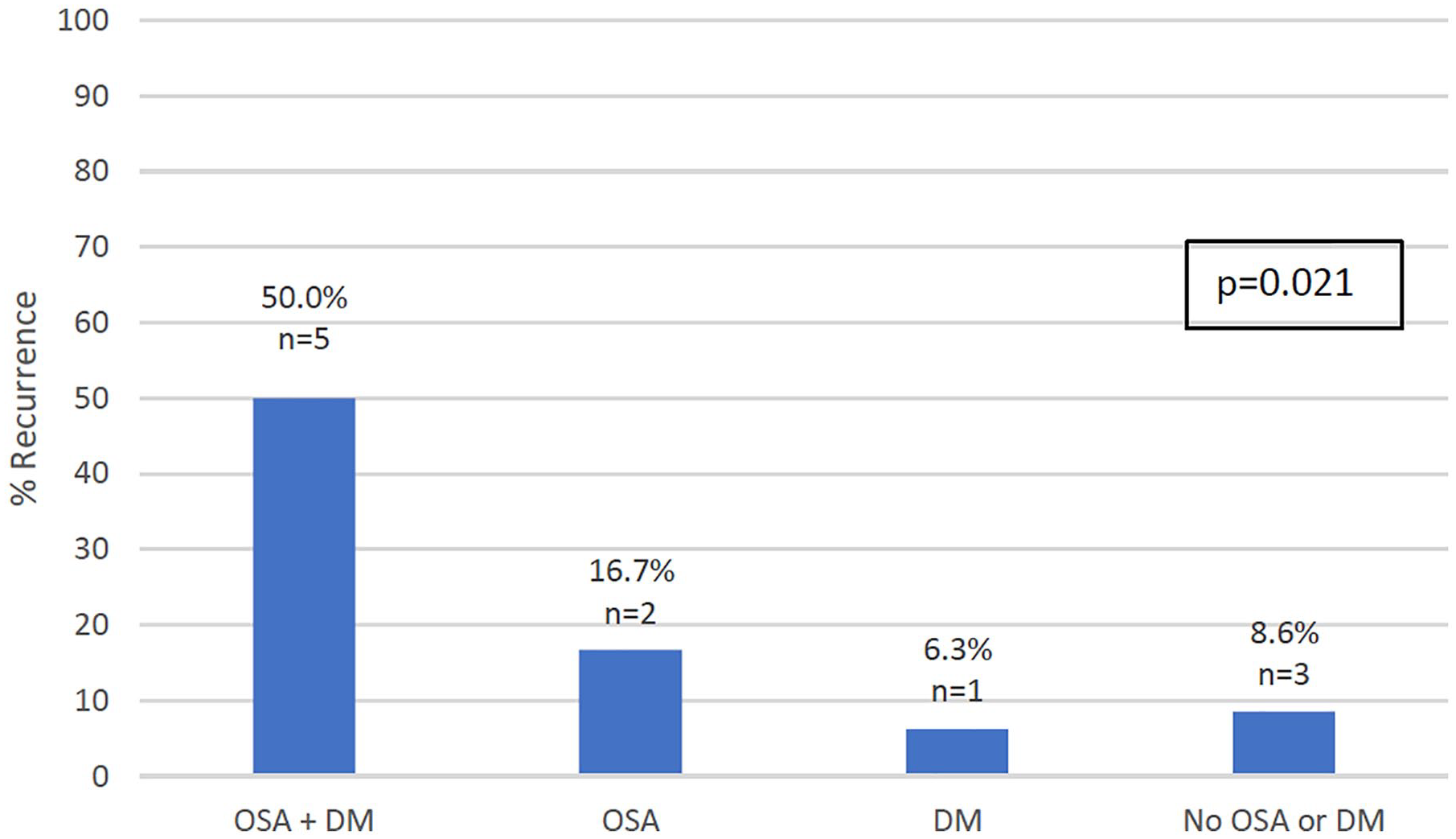
Spontaneous cerebrospinal fluid leak recurrence in patients with obstructive sleep apnea (OSA) and diabetes mellitus (DM)(OSA + DM), only OSA(OSA), only DM(DM), neither OSA nor DM (No OSA or DM). Fisher’s exact test was used to determine statistical significance of the proportion differences among the groups.
The association of OSA, DM, and BMI with sCSF leak recurrence rate were evaluated using multivariate logistic regression (Table 3). The model comparing OSA, DM, and BMI reported that none of the variables had an independent statistically significant contribution to leak recurrence, with OSA diagnosis expressing the highest OR of 3.93 (95% CI = 0.953-15.983, P = .058).
Multivariate Analysis of CSF Leak Recurrence Comorbidity Associations.
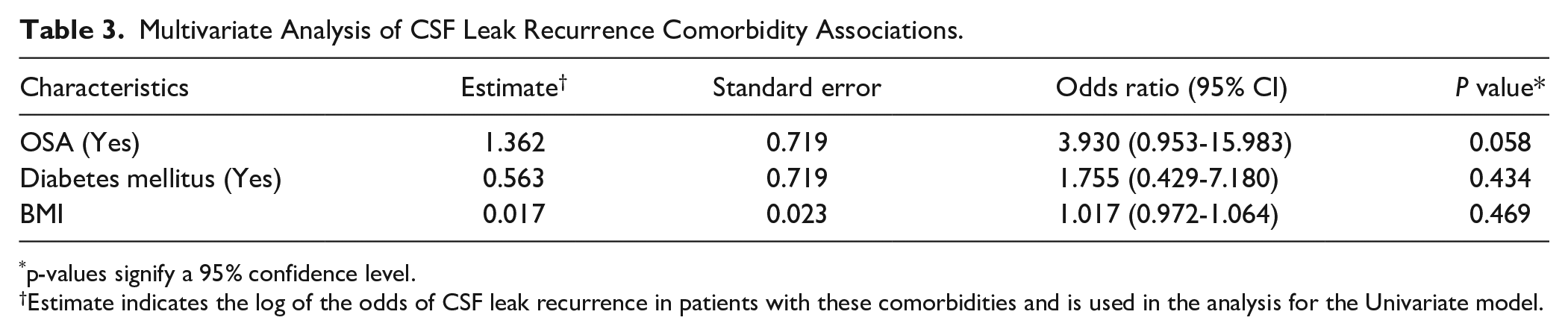
p-values signify a 95% confidence level.
Estimate indicates the log of the odds of CSF leak recurrence in patients with these comorbidities and is used in the analysis for the Univariate model.
All 21 anterior skull base surgical sCSF leak patients were treated with endoscopic transnasal approaches, and 2 (9.5%) experienced a sCSF leak recurrence. All ASB leaks were repaired using a nasoseptal flap with fat graft. Of the 47 surgically treated for LSB leaks, 11 (23.4%) were treated using transmastoid approaches, 35 (74.4%) with an MCF approach, and 1 with a combined approach. One patient was not surgically treated and did not experience leak recurrence. Four patients treated with a transmastoid approach (36.4%) and 5 treated with an MCF approach (14.3%) experienced recurrence of sCSF leak (Figure 2). No statistical difference was observed among these surgical approaches with respect to frequency of leak recurrence (P = .186). However, patients treated using a transmastoid approach had a lower median hospital stay (1 day, IQR = 1,3.5) when compared to those treated with the MCF approach (4 days, IQR = 3.5, P = .016). Forty of the 47 (85.1%) surgically repaired LSB defects were repaired using locally harvested bone graft, fascia, and synthetic dural sealant with the bone replaced by titration plates and screws. Seven (14.9%) were repaired using autologous conchal cartilage and temporalis graft.
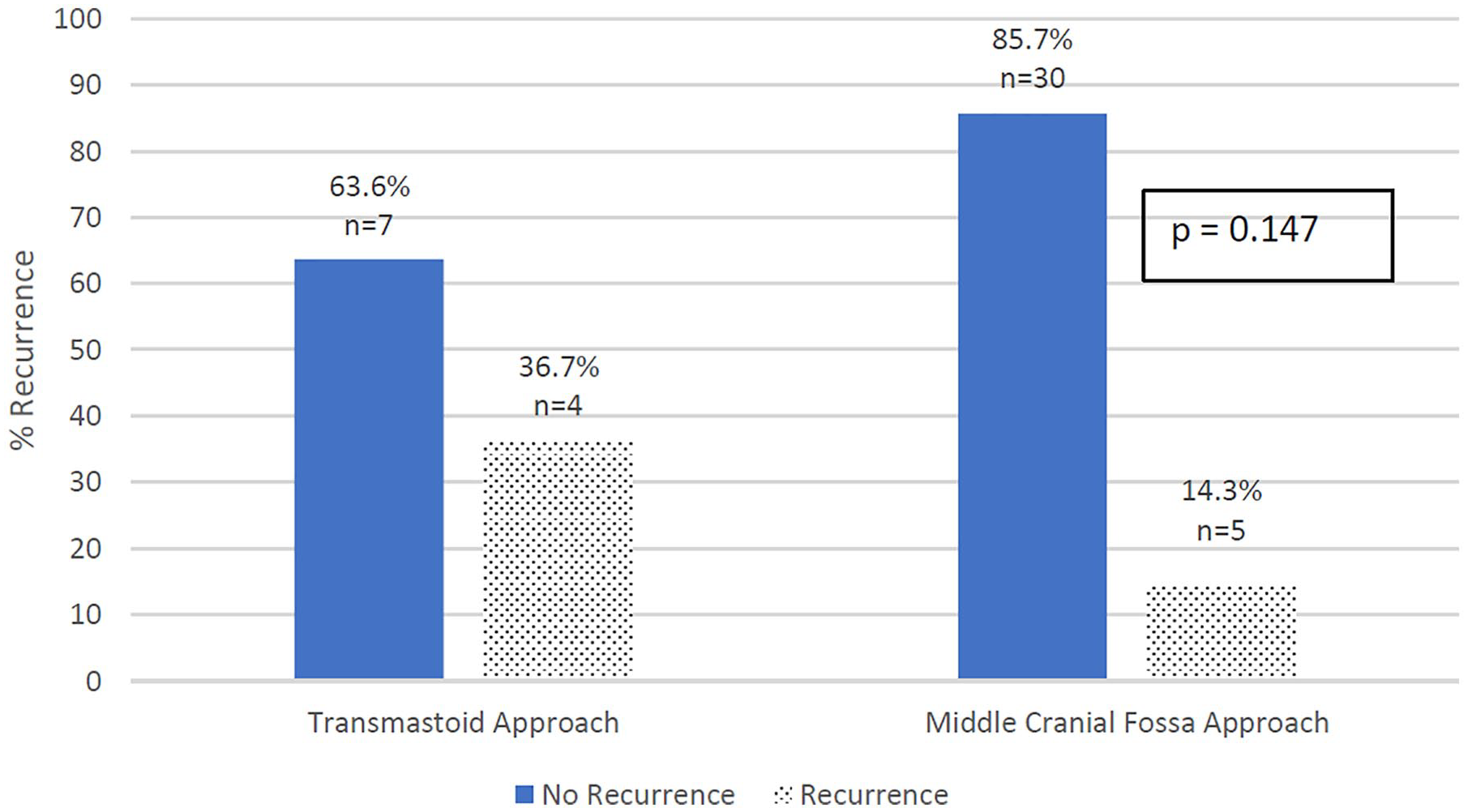
Solid bars represent percent of non-recurrent spontaneous cerebrospinal fluid (sCSF) leak, dotted bar represents recurrence rate of lateral sCSF leaks treated with Transmastoid and Middle Cranial Fossa approaches.
Three (27.7%) patients treated with transmastoid approach and 20 (57.1%) treated with the MCF approach were managed post-operatively with a lumbar drain (P = .432). Patients that received lumbar drains had lower recurrence rates (7.0%) compared to patients without lumbar drains (28.6%) (P = .049). The median number of days using lumbar drains was not significantly different between the recurrence and non-recurrence groups (3, [2,4]; 2[2,3]) (P = .72)).
Discussion
Cranial cerebrospinal fluid leaks are characterized by an egress of CSF fluid from the intracranial cavity. While most frequently caused by trauma and surgery, spontaneous CSF leaks are idiopathic. 1 However, the link between obesity and spontaneous CSF leaks has been well documented.4-6 As the prevalence of obesity continues to increase, the incidence of spontaneous CSF leaks can be expected to rise accordingly.4,22,23 The rise in BMI is aligned closely with the increased incidence of sCSF leaks nationwide, 4 as higher incidences of sCSF leaks are reported in areas with higher BMIs throughout the United States. 24
Only 22% of patients in this cohort of sCSF leak patients met diagnostic criteria of IIH of papilledema or elevated open pressure on lumbar puncture. In a retrospective review by Yancey et al 25 17% of sCSF leak patients were found to have evidence of IIH. In a retrospective survey study on 167 patients with recorded sCSF leaks, Zocchi et al 26 demonstrated that only 29% had prior symptoms of IIH. These relatively low proportion of patients with IIH is likely due to inappropriate timing of intracranial pressure evaluation as CSF leakage may normalize intracranial pressure during an active leak. Evaluating patients for intra-cranial hypertension may be more effective after repair of sCSF leaks through neuro-ophthalmology evaluation and opening pressure measurements, however, criteria were not well established for follow up and testing patients for IIH after surgery improved symptoms. This has led to a much lower rate of IIH diagnosis in patients within this cohort and sCSF leak patients across the United States. Prospective studies in which ICP is monitored in patients with repaired sCSF leaks would provide the best estimate of the rate of IIH in this patient group. Arachnoid granulations may also cause sCSF leaks but these were not noted in this patient cohort.
Although IIH is difficult to diagnosis given the current criteria, OSA has been linked to sCSF leaks in previous studies.4,6 The pathophysiology of this association is thought to be due to intermittent nighttime breathing disturbances leading to episodes of hypercapnia and reflexive increase in cerebral vasodilation resulting in erosion of the skull base. In this series, patients with OSA were up to 5 times more likely to have recurrence on univariate analysis, indicating that OSA is likely an important contributor to the high recurrence rates of sCSF leaks. Although the contribution of OSA to sCSF leaks did not reach significance on multivariate analysis (P = .058), this is a testament to the multifactorial nature of elevated intracranial pressure and the contributions of obesity and metabolic disorders such as DM on its pathology. Furthermore, while the percentage of OSA patients in this cohort is similar to some studies, the prevalence of OSA is approximately 17% in the general population but shown to be as high as 83% in sCSF leak patients.6,27 This indicates that OSA is largely underdiagnosed in this patient cohort and in patients with sCSF leaks in general. These factors also explain the relatively wide 95% confidence interval when risk of recurrence was assessed with OSA on univariate analysis.
Obesity remains a consistent feature in sCSF leaks. The patient characteristics included in this study closely adhere to existing literature. The average age (58.2 years), BMI (37.1 kg/m2), and percentage female (74%) of those included in the final analysis were also very similar to a multicenter retrospective analysis published by Nelson et al in 2015, which reported an average age of 57.03 years and average BMI of 37.8 kg/m2. 4 These findings underscore the importance of obesity in the development of this pathology. While BMI was not found to be independently associated with sCSF leaks recurrence, the sequelae of obesity including OSA and DM have ties to both the initial progression of sCSF leaks as well as their recurrence. Consequently, weight control measures such as adherence to diet and exercise as well as bariatric surgery may prevent development and recurrence of sCSF leaks. 28
The surgical approach for repair of lateral spontaneous sCSF leaks is determined generally by the location and size of the leak as well as surgeon preference. While the MCF approach offers the ability to perform wide multilayer repair, the transmastoid approach offers a less invasive mechanism of repair. 29 The relative safety and efficacy of the MCF and transmastoid approach have not been extensively studied in systematic controlled studies. 14 In this study, there was no significant difference in the sCSF leak recurrence rates of patient treated with the transmastoid and MCF approaches. In addition to these 2 approaches, a combined MCF-transmastoid approach has been rising in favor as a complex, yet effective method repairing sCSF leaks. 25 Spontaneous CSF leaks are known to have a higher rate of recurrence compared to other etiologies of CSF leak, as reported by Chaaban et al 30 Previously published studies have cited leak recurrence rates between 25% and 87%.6,14,21,31,32 More recent retrospective studies have cited the recurrence rate of anterior skull base CSF leak of 8% (range 0%-38%), similar to that recorded in this cohort (9.5%). Lateral skull base leaks have a recorded leak recurrence rates ranging between 0% and 22% which adheres closely to the recurrence rate of 18.8% in this study. 14
Having a lumbar drain placed at the primary surgery seemed to decrease recurrence rate. Lumbar drain use remains a debated topic in anterior and lateral spontaneous CSF leaks. Little evidence exists that lumbar drains reduce sCSF leak recurrence,33,36 yet lumbar drains continue to be used, especially in high-risk patients with multiple defects or large defects with high flow.14,24 Over the course of the study period, the use of lumbar drains evolved with the understanding of sCSF leaks. While this finding suggests that lumbar drains facilitate effective healing of the surgical bed and allow for the equilibration of CSF pressures following repair, the relationship between LD use and recurrence is unclear as the average time to recurrence is 27 months following repair, not in the immediate post-operative period. This may suggest that this statistical difference is more due to chance. Therefore, evaluation of lumbar drain use under more robust criteria is necessary for definitive conclusion.
This cohort of patients is unique as it is entirely composed of patients with either anterior or lateral skull base spontaneous CSF leaks. Despite the different locations in the skull base and clinical symptomatology, anterior and lateral skull base spontaneous CSF leaks are different manifestations of the same disease process. This allows us to adequately analyze pertinent comorbidities and risk factors of all sCSF leaks to inform clinical decision making and management. Medical and surgical management of OSA may help prevent sCSF leaks and their recurrence, however there are reports of continuous positive air pressure (CPAP) contributing to a case of CSF leak.34,35
There are several limitations to this study. The sample size of 69 with 11 leak recurrences is relatively small, which limits the statistical power of the analysis. The retrospective nature of data collection is limited by non-systematic reporting of major clinical variables. Inconsistent reporting of CPAP pressures, CPAP compliance and Apnea Hypopnea Index (AHI) make a more granular analysis of the contribution of OSA to sCSF leaks unreliable. Furthermore, because this patient cohort had inconsistent evaluation of IIH post-operatively, the percentage of true IIH in this group cannot be determined accurately. Future prospective trials are needed to gain a better understanding of this relationship. Prospective studies in which patients diagnosed with sCSF leaks obtain sleep studies at a single institution and provide consistent documentation of CPAP compliance and CPAP pressures would provide valuable insight into the relationship of OSA and sCSF leak recurrence. Prospective evaluation of ICP following sCSF leak repair through consistent neuro-ophthalmology follow up and post-operative opening pressure evaluations would provide more definitive analysis of IIH in this population. This study is limited by its retrospective nature but adds novel information about the relationship of OSA to sCSF leak recurrence to a growing body of literature on the understanding of this pathology.
Conclusion
Spontaneous CSF leak recurrence is complex and multifactorial, but these findings suggests that OSA is a significant predictor for recurrence. Our study also indicates that patients with sCSF leak and concurrent OSA and DM should be counseled on increased risk of recurrence. Close monitoring of patients with these comorbidities post-operatively may be indicated. Surgical technique of lateral and anterior skull base CSF leaks was not correlated with recurrence. Patients with lumbar drains had a lower rate of sCSF leak recurrence compared to those without drains, but controlled prospective studies are needed for more definitive conclusions on the safety and efficacy of these interventions.
Footnotes
Author contributions
Firas Hentati, BS: Study design and conception, data collection and analysis, manuscript writing
Armine Kocharyan, MD: Study design and conception, data analysis, manuscript review and editing.
Jeremy Ruthberg, MD: Study design and conception, manuscript review and editing.
Stephen Trudeau, MD: Study design and conception, manuscript review and editing.
Tarun Jella, MPH: Data analysis, graph and table drafting.
Nirav Patil, MBBS, MPH: Data analysis, graph and table drafting.
Claudia I. Cabrera, MD: Study design, data collection
Sarah Mowry, MD: Study design and conception, manuscript review and editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.