
Abstract
Objectives:
This study investigated the relationship between quantitative value of endolymphatic hydrops in the affected ear and the hearing threshold in patients with unilateral Meniere’s disease.
Study Design:
Prospective study.
Methods:
Forty patients with unilateral definite Meniere’s disease were diagnosed in outpatient clinic. We recorded their clinical symptoms (duration of vertigo and tinnitus and duration of vertigo attacks), and obtained the hearing thresholds of high, middle, and low by pure tone audiometry. A 3D-FLAIR MRI revealed endolymphatic hydrops and assessed quantitative values of cochlear and vestibular endolymphatic hydrops. We assessed the correlation between hearing thresholds and quantitative values of endolymphatic hydrops.
Results:
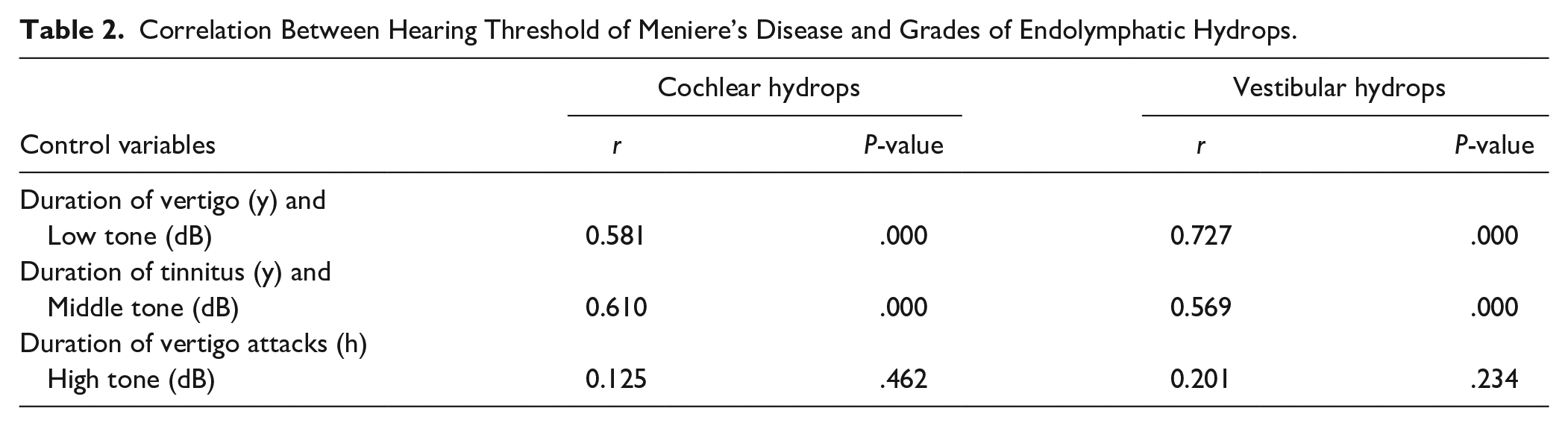
All patients showed varying degrees of endolymphatic hydrops in the affected ear. With the duration of vertigo, tinnitus and vertigo attacks as control variables, partial correlation analysis showed that the correlation coefficients between quantitative value of cochlear hydrops and hearing thresholds of low, middle, and high tone in the affected ear were 0.581, 0.610, and 0.125, respectively. The correlation coefficients between quantitative value of vestibular hydrops and hearing thresholds of low, middle, and high tone in the affected ear were 0.727, 0.569, and 0.201, respectively.
Conclusions:
The degree of endolymphatic hydrops in Meniere’s disease can be revealed and assessed by 3D-FLAIR MRI after intravenous administration of double doses of gadoterate meglumine. Clinical evaluation of endolymphatic hydrops in Meniere’s disease can be assisted by low- and middle-tone hearing thresholds, thereby providing anatomical support for the clinical symptoms of Meniere’s disease.
Introduction
Meniere’s disease is a complex disease of the inner ear. It is characterized by intermittent vertigo attacks, fluctuating hearing loss, tinnitus, aural fullness, and other symptoms. Its pathological substrate is endolymphatic hydrops. 1 Although scholars believe that excessive secretion or an outflow disorder affects the electrophysiological environment of the inner ear, thereby affecting the signal transduction of cochlear and vestibular hair cells, 2 others emphasize a possible role of ischemia due to vascular diseases. 3
In 2015, the American Academy of Otolaryngology Head and Neck Surgery classified Meniere’s disease as either “definite” or “probable” based on the clinical symptoms. 4 Since it is not possible to get histopathological confirmation in vivo, the diagnosis of Meniere’s disease is mainly based on clinical symptoms and otology examination. However, patients complain of subjective clinical symptoms, which are often confused with vestibular migraine, benign recurrent vertigo, and other diseases. 5 According to the diagnostic criteria of Meniere’s disease, patients with the definite type have different degrees of hearing loss. In this context, pure tone audiometry is the main method to detect hearing loss in patients with Meniere’s disease, given that it can measure the hearing threshold at a certain frequency and reflect the degree of hearing loss.
In recent years, with continuous development of magnetic resonance technology and equipment, intravenous injection of gadolinium contrast agent makes it possible to visualize endolymphatic hydrops in Meniere’s disease.6,7 After 3D-FLAIR MRI scan, the perilymph shows high signal and the endolymph shows low signal, so that the boundary between endolymph and perilymph of the cochlea and vestibule can be clearly distinguished and the degree of endolymphatic hydrops in the cochlea and vestibule can be assessed.
Based on a large number of clinical observations and data analysis, it is believed that the early stage of Meniere’s disease mainly involves low-tone hearing loss; with the progression of the disease, vertigo recurs and hearing fluctuation drops, while middle- and high-tone hearing gradually declines in the later stage, finally leading to a flat hearing curve.8,9 In summary, the hearing level in patients with Meniere’s disease decreases gradually with the course of the disease. 10 Other studies have shown that the degree of endolymphatic hydrops in the affected ear in patients with Meniere’s disease gradually increases with the progression of the disease. 11 Therefore, we hypothesized that there is a correlation between hearing loss and endolymphatic hydrops in the affected ear in patients with Meniere’s disease.
In this study, double dose of gadoterate meglumine was intravenously administered to patients with Meniere’s disease and 3D-FLAIR MRI was used to quantitatively assess the degree of endolymphatic hydrops. Then, the correlation between the quantitative value of endolymphatic hydrops and the hearing threshold was assessed to improve clinical diagnosis and provide an anatomical basis for the clinical symptoms of Meniere’s disease.
Materials and Methods
Patients
This is a retrospective study. Forty patients (23 men and 17 women; aged 33-77 years, with an average age of 60 years; 25 left ears and 15 right ears affected) who visited the Otolaryngology department of the First Hospital of China Medical University from November 2019 to December 2020 were included. They were diagnosed as “definite” unilateral Meniere’s disease according to the diagnostic criteria established by the American Academy of Otolaryngology Head and Neck Surgery in 2015. 4
The clinical symptoms of the patients were examined and evaluated by professional otolaryngologists. All the patients had persistent tinnitus and intermittent vertigo. Pure tone audiometry was performed in all patients, and progressive hearing loss was observed in all patients.
All patients had no history of gadolinium contrast agent allergy, neurologic deafness or otitis media, and ear surgery. This study was approved by the Medical Ethics Committee of our Hospital (2018-298-2). All patients were informed of the risks of gadolinium contrast agent examination, and they all signed informed consent.
Pure Tone Audiometry
Pure sound audiometry was conducted in standard sound insulation room with background noise less than 30 dB. Pure tone audiometer OB922 using Danish Madsen and the lifting method was used to test the hearing thresholds of the left and right ears of the receiver at 250 Hz, 500 Hz, 1 kHz, 2 kHz, 4 kHz, and 8 kHz, respectively. The test method was in line with the acoustic audiometry of GB/T16403-1996. We divided the hearing threshold into low (250 and 500 Hz), middle (1 and 2 kHz), and high tone (4 and 8 kHz). The hearing thresholds of low (mean value of hearing threshold at 250 and 500 Hz), middle (mean value of hearing threshold at 1 and 2 kHz), and high tone (mean value of hearing threshold at 4 and 8 kHz) were calculated.
Intravenous Gadoterate Meglumine Injection and MRI
The scan was performed using a 3.0-T MR scanner (Signa Pioneer 3.0T, GE Healthcare) with a 21-channel phased-array receive-only coil. The scanning sequences included brain T2 FLAIR, 3D FIESTA C Shim, and T1WI for inner ear. Four hours after an intravenous injection of double dose of gadoterate meglumine, 3D-FLAIR was performed.
The brain T2 FLAIR sequence parameters were as follows: TR 9000 ms, TE 95 ms, TI 2648 ms, slice thickness 5 mm, matrix size 256 × 256, echo train length 22, acceleration factor 1, and scan time 1 minute and 57 seconds. 3D FIESTA-C Shim sequence parameters were as follows: TR 6.6 ms, TE 3.1 ms, slice thickness 0.8 mm, matrix size 256 × 256, acceleration factor 2, and scan time 3 minutes and 37 seconds. T1WI sequence parameters were as follows: TR 7520 ms, TE 9.5 ms, slice thickness 3 mm, matrix size 320 × 192, acceleration factor 2, and scan time 1 minute and 38 seconds. After the intravenous injection of double dose of gadoterate meglumine (Hengrui Medicine, 20 mL/dose, 0.5 mol/L), the injection dose was 0.4 mL/kg and the speed was 0.2 mL/second, while the parameters of 3D-FLAIR sequence were as follows: TR 9000 ms, TE 163 ms, TI 2175 ms, slice thickness 1 mm, matrix size 288 × 288, echo train length 180, acceleration factor 4, and scan time 12 minutes and 4 seconds.
Imaging Analysis
Routine scan sequence was used to exclude other neoplastic lesions of the brain and ear. The 3D-FLAIR sequence after a 4-hour delay was used to visualize endolymph and perilymph. The quantitative value of endolymphatic hydrops was measured in accordance with the measurement method of the 3-level grading standard proposed by Nakashima et al. 12 The quantitative value of endolymphatic hydrops in vestibule (SVR) was measured at the level where the saccule and utricle showed the largest value. The degree of endolymphatic hydrops in vestibule was expressed by the ratio of the area of endolymph in the vestibule to the area of the entire the vestibule (the sum of the endolymphatic and perilymphatic spaces of the vestibule). The quantitative value of endolymphatic hydrops in the cochlea (CCR) was measured at the optimal location of the cochlear basal turn. The degree of endolymphatic hydrops in the cochlea was expressed as the ratio of the transverse diameter of the cochlear duct to the sum of the transverse diameters of the cochlear duct and the perilymph (the sum of scala vestibuli and scala tympani) of the second turn of cochlea (Figure 1). All images were analyzed by 2 double-blinded radiologists who calculated the SVR and CCR for each patient. An average of both raters was calculated per subject and used for statistical purposes.
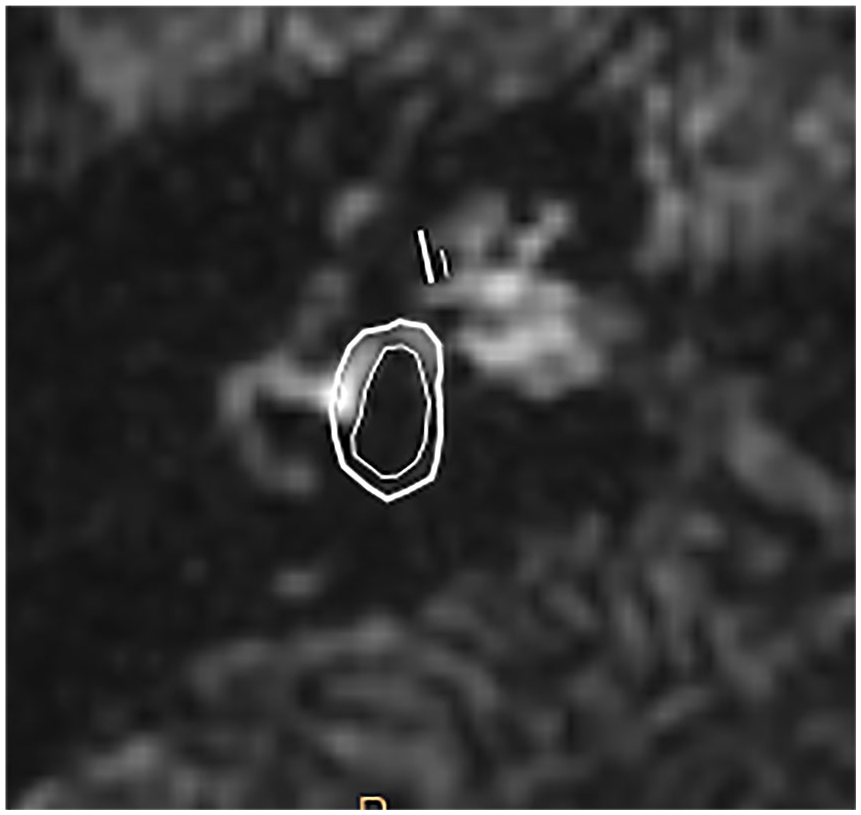
Thin line: transverse diameter of cochlear canal; thick line: transverse diameter of scala vestibule, scala tympani, and cochlear canal. Thin circle: endolymphatic space; thick circle: cross-sectional area of the vestibule.
Statistical Analysis
SPSS 20.0 software was used for data analysis, and the data that did not conform to the normal distribution were represented by the median. Partial correlation was used to analyze the correlation between the low-, middle-, and high-tone hearing thresholds and the degree of the endolymphatic hydrops in cochlea and vestibule (control variables: duration of vertigo and tinnitus and duration of vertigo attacks). A significant difference was considered when P < .05.
Results
No other abnormal shape or signal diseases were found in the inner ear and brain by plain MRI scanning. After intravenous administration of gadolinium, the contrast entered the perilymph but not the endolymph. Therefore, in all patients, the perilymphatic spaces of cochlea, vestibule, and semicircular canals showed an obvious high signal, while the endolymphatic spaces showed low signal. Therefore, cochlea, saccule, utricle, and other structures could be clearly displayed, with a clear boundary between the endolymph and perilymph. All patients had different degrees of endolymphatic hydrops in cochlea and vestibule of the affected ear (Figure 2a-c).
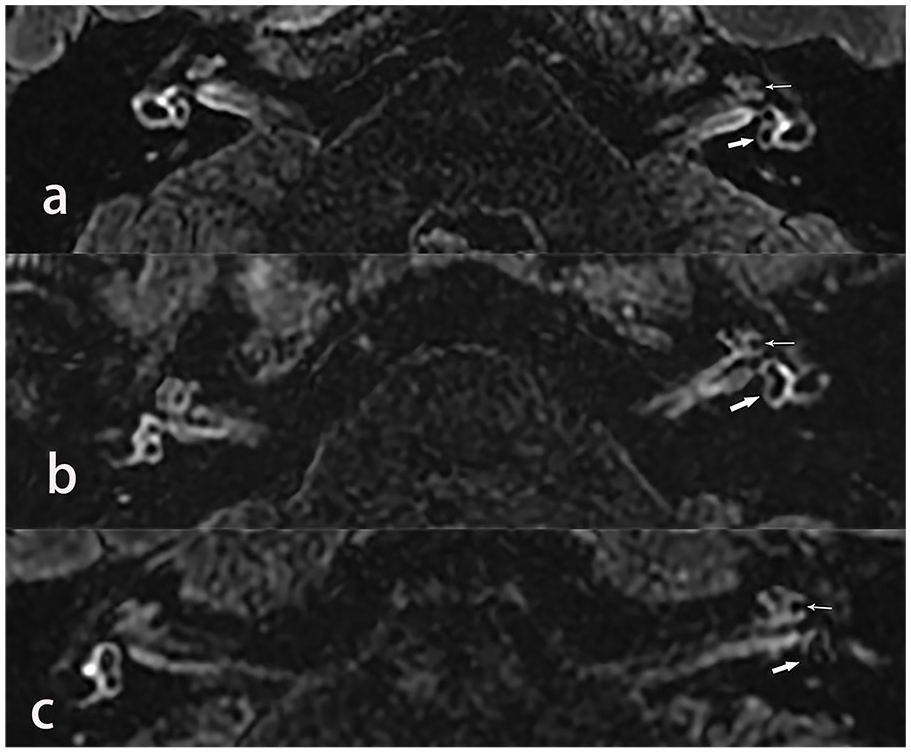
(a) Meniere’s disease of the left ear (22-year-old woman). The quantitative value of endolymphatic hydrops (thin arrow) were 0.211 (cochlea, thin arrow), 0.233 (vestibule, thick arrow). (b) Meniere’s disease of the left ear (70-year-old man). The quantitative value of endolymphatic hydrops (thin arrow) were 0.492 (cochlea, thin arrow), 0.370 (vestibule, thick arrow). (c) Meniere’s disease of the left ear (57-year-old woman). The quantitative value of endolymphatic hydrops (thin arrow) were 0.619 (cochlea, thin arrow) and 0.568 (vestibule, thick arrow).
All patients had different degrees of hearing loss, demonstrated in the audiogram as different hearing thresholds at low, middle, and high tone. The quantitative values of hearing thresholds and cochlear and vestibular endolymphatic hydrops are shown in Table 1.
Detailed Information of All Patients.
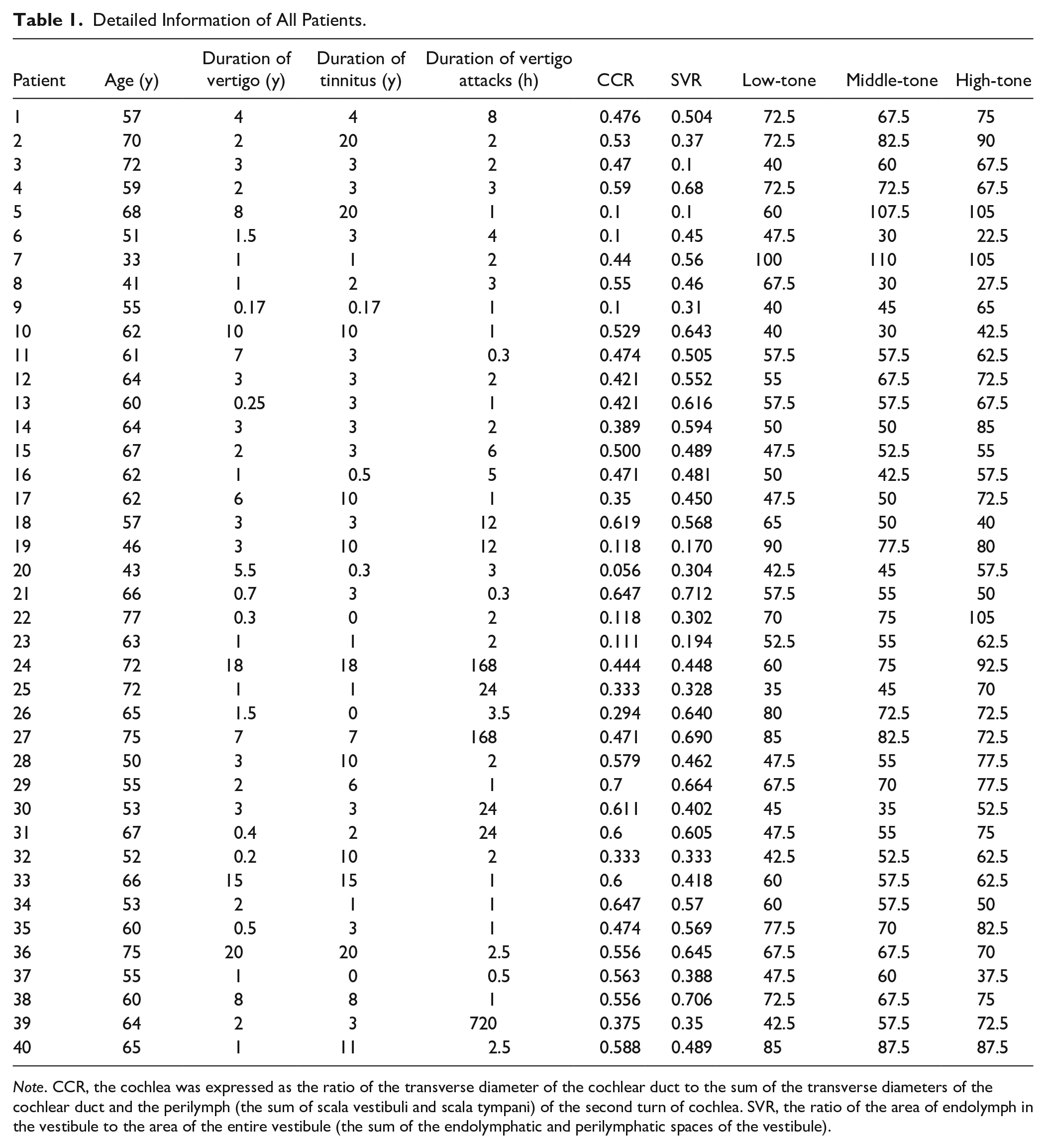
Note. CCR, the cochlea was expressed as the ratio of the transverse diameter of the cochlear duct to the sum of the transverse diameters of the cochlear duct and the perilymph (the sum of scala vestibuli and scala tympani) of the second turn of cochlea. SVR, the ratio of the area of endolymph in the vestibule to the area of the entire vestibule (the sum of the endolymphatic and perilymphatic spaces of the vestibule).
Partial correlation analysis was used to demonstrate the correlation between low-, middle-, and high-tone thresholds and quantitative values of cochlear and vestibular endolymphatic hydrops (Table 2). Among them, the low and middle tone thresholds were significantly positively correlated with the quantitative values of endolymphatic hydrops in the cochlea and vestibule (P < .05). The correlation scatter diagram of the 2 is shown in Figure 3. There was no significant correlation between the high tone and the quantitative values of vestibular and cochlear endolymphatic hydrops (P > .05).
Correlation Between Hearing Threshold of Meniere’s Disease and Grades of Endolymphatic Hydrops.
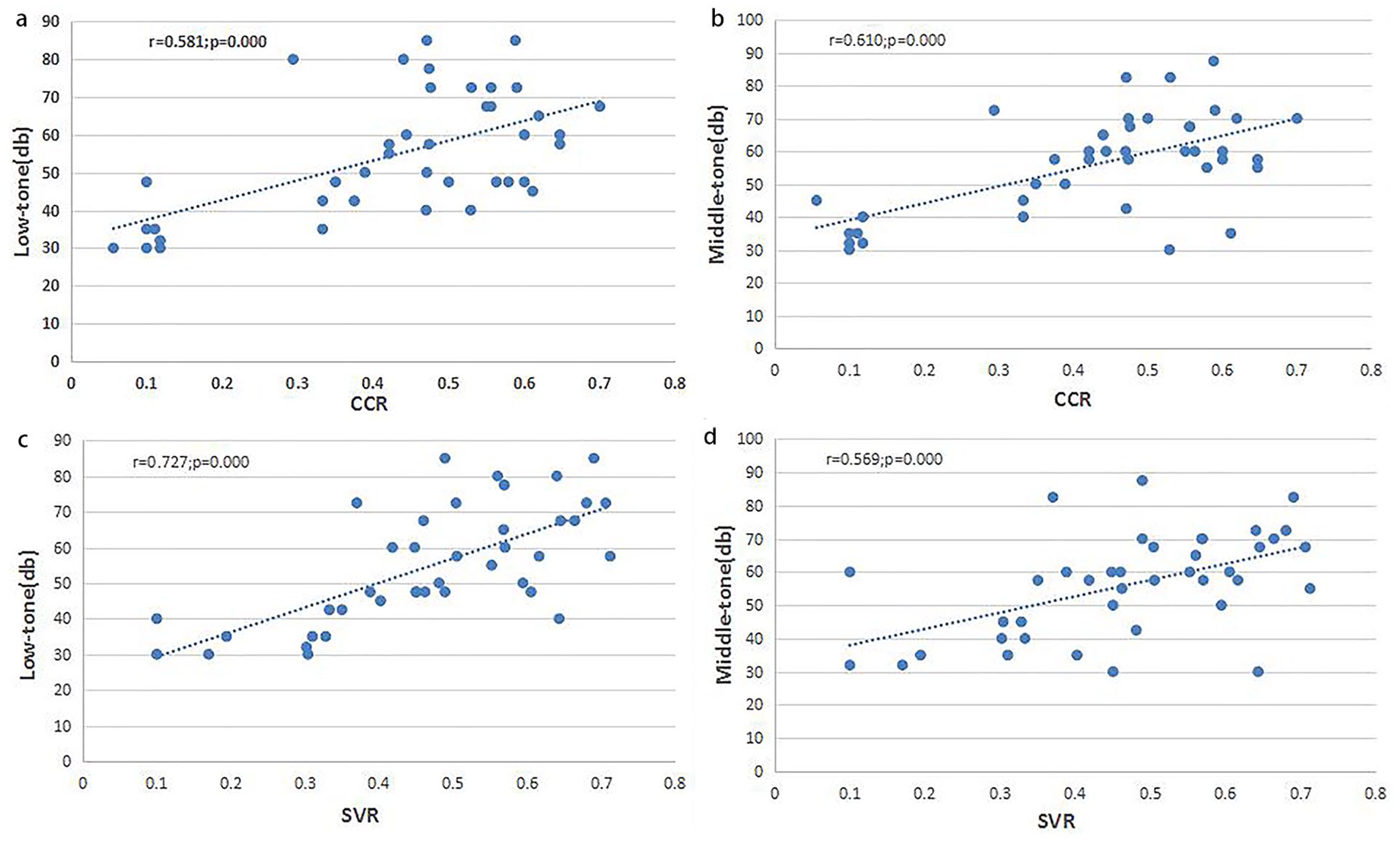
Correlation between quantitative value of endolymphatic hydrops and low- middle tone hearing threshold.
Discussion
Hallpike et al (1937) discovered the presence of endolymphatic hydrops in the inner ear of patients with Meniere’s disease through autopsy. In recent years, endolymphatic hydrops has been considered as one of the main causes of various symptoms of Meniere’s disease. 13 Although endolymphatic hydrops can be detected at autopsy, its diagnosis is merely clinical. With the development of MRI sequence and technique, the visual observation of endolymphatic hydrops has become possible. At present, there are 2 main injection methods: the intratympanic method and the intravenous method. Gadolinium injection in the intratympanic method requires invasive puncture of the tympanic membrane and is affected by the permeability of the round window membrane. 14 Intravenous gadolinium is less invasive and can display bilateral inner ear structures at the same time, whereas the contrast agent is more evenly distributed in both ears. 15 Therefore, intravenous gadolinium has been widely used in the clinical setting.7,16 In this study, MRI scan was performed 4 hours after intravenous injection of double dose gadoterate meglumine, and it was found that all patients had varying degrees of cochlear and vestibular endolymphatic hydrops in the affected ear.
The sound in the external auditory canal causes the eardrum to vibrate, which is transferred to the cochlea through the ossicular chain and the oval window. The basal membrane in the cochlea vibrates in response to the mechanical stimulation, whereas the external hair cells amplify the stimulation and transfer fluid vibration to the internal hair cells that sense sound. The sound frequency determines the location of the maximum vibration of the basal membrane. Clinically, hearing is divided into low (250 and 500 Hz), middle (1 and 2 kHz,), and high tone (4 and 8 kHz). Studies have shown that the tip of the cochlea receives low-tone waves and the basal receives high tone.17,18 Damage to any part of the sound pathway can lead to hearing loss.
As for the course and characteristics of Meniere’s disease, Yamashita found that endolymphatic hydrops in patients started from the cochlear top turn, and early hearing in Meniere’s disease was dominated by the elevation of low tone threshold, 19 which is consistent with our previous inferences. The results of this study showed that the increase in low- and middle-tone hearing threshold significantly and positively correlated with the degree of endolymphatic hydrops in the cochlea and vestibule, which indicated that the generation of endolymphatic hydrops interfered with the transmission of inner ear sounds, thus leading to hearing loss. Our results are consistent with what has been reported in previous studies.20 -22 The elevation of low- and middle-tone hearing thresholds reflects the severity of endolymphatic hydrops to some extent. In the absence of MRI images, it can provide a basis for the assessment of severity of endolymphatic hydrops in patients with Meniere’s disease, and early control of endolymphatic hydrops may delay the progression of hearing loss.
Another result of this study showed that there was no significant correlation between the elevation of high-tone hearing threshold in these patients, and the quantitative value of endolymphatic hydrops in cochlea and vestibule, which was not consistent with the results of Yang et al. 23 The reason may be that most of the patients in this study were older individuals, and some studies have suggested that the increase in high-tone hearing threshold is related to advanced age. 10 Albera et al 10 keep affected ear hearing threshold after deducting the contralateral hearing threshold, found that the audiogram from peak to rise, therefore, considered that age may affect the change of the high tone hearing threshold. Hence, to obtain more accurate results, future studies will need a larger sample size and removing the factor of age to analyze the relationship between the high-tone hearing threshold and the endolymphatic hydrops.
In addition, this study found that the 3D-FLAIR MRI of the inner ear after a 4-hour delay revealed lamellar high signal enhancement in the base of the inner auditory canal of both ears in Meniere’s disease (Figure 4), which was also seen in other studies of Meniere’s disease using intravenous administration.21,24,25 In the study of transtympanic injection, no enhancement was observed in the inner auditory canal base. The main auditory nerve and small blood vessels at the bottom of the inner auditory canal were accompanied by a small amount of cerebrospinal fluid. However, after intravenous contrast agent injection, the inner auditory canal base in both ears appeared enhanced. The question arises whether there is a barrier at the bottom of the inner auditory canal in the ear that allows a small amount of gadolinium to seep through the blood vessels, resulting in enhanced image. The morphological and signaling changes after dynamic enhanced scanning may provide more insights, which will be the direction of our next research.
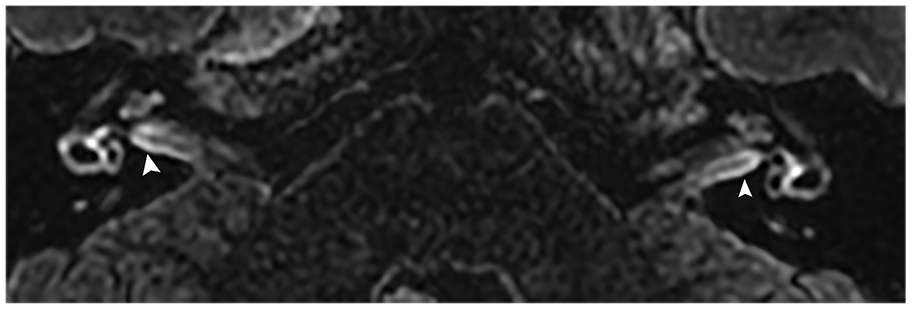
Lamellar high signal enhancement at the base of the inner auditory canal (arrow).
Limitation
Because there was no histopathological evidence in vivo, this study could not prove the existence of endolymphatic hydrops through pathohistology.
Conclusion
The degree of endolymphatic hydrops in Meniere’s disease can be revealed and assessed by 3D-FLAIR MRI after intravenous administration of double dose of gadoterate meglumine. Clinical evaluation of endolymphatic hydrops in Meniere’s disease can be assisted by the low- and middle-tone hearing thresholds and provide anatomical support for the clinical symptoms of Meniere’s disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Sky Image Research Foundation (Z-2014-07-1912).