
Abstract
Objective:
To describe treatment pathways and long-term outcomes in 64 patients with idiopathic subglottic stenosis (iSGS), including the impact of serial intralesional steroid injection (SILSI) on degree of stenosis, need for subsequent operation, and patient-reported outcome measures.
Methods:
Retrospective review of 64 female patients with iSGS undergoing varied management approaches, 57 of whom underwent SILSI as at least part of their care. Treatment pathways included SILSI only, endoscopic intervention followed by SILSI only, endoscopic interventions only, endoscopic intervention followed by SILSI followed by need for repeat endoscopic intervention, open surgery, and tracheotomy. Outcomes assessed included subjectively estimated percent airway stenosis, dyspnea index (DI), modified medical research council (MMRC) dyspnea scale, voice handicap index-10 (VHI-10), number of operative and office-based procedures performed, need for subsequent operative intervention, and inter-operative interval.
Results:
Treatment pathways included SILSI alone (n = 6), endoscopic intervention(s) followed by SILSI only (n = 31), SILSI followed by additional endoscopic or office-based procedures (n = 16), open surgery (n = 3), and tracheostomy (n = 4). 57 of 64 patients underwent SILSI as at least part of their treatment. Inter-operative interval was increased after starting SILSI. Of patients undergoing SILSI, those with more procedures or shorter inter-operative interval prior to SILSI were more likely to return to the operating room. Estimated stenosis, DI, MMRC, and VHI-10 decreased with SILSI. Stenosis was not correlated with DI, MMRC, or VHI-10, though DI was correlated with both MMRC and VHI-10 score.
Conclusion:
Of 57 patients undergoing SILSI, 37 did not require further operative intervention. Improvements in inter-operative interval, dyspnea, and voice were observed across patients. Randomized trials to identify which patients may benefit most from SILSI are warranted.
Keywords
Introduction
Idiopathic subglottic stenosis (iSGS) was first described in 1972, and is defined as cricotracheal junction stenosis without intubation, trauma, autoimmune disease, or neoplasia.1-3 Treatment options have a variety of risk profiles from open operations with the highest risk profile to office-based interventions with the lowest, while endoscopic operative treatment has an intermediate risk profile and is the most utilized.4-11 As endoscopic treatment is rarely curative, inter-operative interval (IOI) is a commonly employed measure, with typical intervals of 1 to 1.5 year on average.4,10,11
A more recent option is serial intralesional steroid injection (SILSI) proposed by Franco et al. 12 Steroids are injected transcutaneously or via flexible endoscope.12-16 SILSI has been used as a solitary treatment or as a supplement to endoscopic operation with the goal of prolonging inter-operative interval or avoiding future endoscopic procedures. Short-term results have shown high safety, tolerance, improved subjectively estimated stenosis, and improved dyspnea symptoms; however, not all patients respond, and longer-term results are limited. Further, a recent multi-institutional study did not show significant benefit for adding SILSI after endoscopic dilation for time to recurrent operation, peak expiratory flow, or clinical COPD questionnaire score. 17 Of note, that multi-institutional study did not employ a uniform SILSI protocol and steroid injections began a median of 1 year after dilation. Naunheim et al reported the largest single institution cohort of 55 patients with average follow-up of 3.5 years. 16 That study focused on voice-related quality of life and spirometric measures rather than the need to return to the operating room.
Though endoscopic and office-based interventions are now the most common methods of treating iSGS, open surgery including cricotracheal resection or laryngotracheal reconstruction is also employed.7,18-20 Lastly, select patients may be managed with tracheotomy due to a variety of patient- and disease-related factors.
The objectives of this study are two-fold: first, to describe the clinical history and outcomes of patients undergoing different treatment pathways for iSGS; and second, to describe the longer-term outcomes of patients undergoing SILSI as sole or adjunctive treatment. This dataset includes long-term follow-up on relatively large group of patients from a single institution with consistently employed SILSI protocol, typically starting soon after endoscopic intervention, with routinely collected patient-reported outcome measures. Practical considerations faced by patients that may motivate treatment decisions are also discussed. Frequency of intervention, patient-reported outcome measures, and subjectively estimated degree of airway stenosis were recorded to characterize outcomes to provide a framework to help guide clinician and patient expectations for outcomes that may be expected with different treatment pathways.
Methods
The study was approved by the University of Wisconsin Institutional Review Board. A review was performed of all patients treated by the senior author for iSGS from 1/2003-2/2022. Patients were excluded if they had intubation-related stenosis or were diagnosed with an autoimmune etiology via serologic and/or pathologic testing. When serologic testing was equivocal, pathologic evaluation was relied upon to rule out underlying autoimmune disease.
Variables Collected
Patient charts were reviewed for demographic (age, sex, race) and treatment (type and timing of intervention(s)) variables. Subjectively estimated percent airway stenosis, voice handicap index-10 (VHI-10), 21 dyspnea index (DI; Gartner-Schmidt et al), 22 and modified medical research council (MMRC) 23 scores were noted.
Endoscopic treatment varied over time, but consisted of some combination of balloon dilation, laser excision or radial incisions, and steroid injection. Most operations were performed with rigid exposure and jet ventilation, with some performed with intermittent apnea. A few patients were treated using laryngeal mask airway (LMA) ventilation and flexible bronchoscope using the same techniques as above. Both potassium titanyl phosphate (KTP) and carbon dioxide (CO2) laser have been used.
Five patients underwent office-based laser intervention, which was classified as an additional procedure other than steroid injection. Patients who underwent an office-based laser procedure were included in the group of patients who required additional interventions beyond steroid injections after starting SILSI. These patients were not included in the inter-operative interval calculation.
SILSI Technique
SILSI has been used at our institution since February 2014. This was initially performed transcutaneously and then transitioned to a transnasal approach.13,14 While our protocol is to perform one injection every month for 3 injections followed by a 1-month post-SILSI tracheoscopy, some variation may occur due to rapid response, logistical factors, and limited response leading to more injections in a series. If post-SILSI tracheoscopy shows stable or improved stenosis, patients return in 6 months for repeat tracheoscopy and possible initiation of the next series.
Airway Stenosis Estimation
Measurements of percent stenosis were estimated by the senior author at the time of exam and obtained by chart review for this study, to a precision of 5%. Where the chart was incomplete, prior videos of transnasal tracheoscopy or operative images were reviewed by the senior author.
Statistical Analysis
Demographic characteristics were summarized by treatment groups.
Comparison of patients undergoing SILSI who required additional interventions and those who did not
Following initiation of SILSI, some patients required additional procedures other than SILSI and some did not. Patient-related factors were compared between these 2 groups with independent samples t-tests or Mann-Whitney rank sum tests if data did not meet parametric testing assumptions. Tests were 2-tailed with a significance level of α = .05. Additional procedures include operative endoscopic dilation, tracheotomy, open airway reconstruction, or office procedures other than steroid injection (office-based laser treatment, scar lysis). Factors evaluated included age, number of procedures prior to SILSI, most recent inter-operative interval (for patients with at least 2 endoscopic dilations prior to SILSI), stenosis at time of first injection, and dyspnea index at time of first injection.
Evaluation of effect of SILSI on inter-operative interval
The effect of SILSI on inter-operative interval was evaluated in all patients who underwent at least 2 operations prior to SILSI using a paired t-test. For patients who have not undergone other procedures after starting SILSI, follow-up duration had to be as long as pre-SILSI inter-operative interval to be included in the analysis. For example, a patient with a pre-SILSI inter-operative interval of 1 year who did not require an additional operation would be excluded if time lapse since most recent operation was less than 1 year. No patients who required other procedures after starting SILSI were excluded from the analysis.
Effect of SILSI on stenosis and patient-reported outcome measures
Changes in estimated percent stenosis, dyspnea index, modified medical research council scale, and voice handicap index-10 scores over a SILSI series were evaluated using repeated measures analysis of covariance (ANCOVA). Whether patients underwent a subsequent procedure after SILSI was included as a covariate. For this analysis, all SILSI series where a patient had pre- and post-SILSI values were included. All series were averaged within a given patient such that each patient was included once in each parameter analysis, and were not weighted disproportionately if they underwent more series. Tests were 2-tailed with a significance level of α = .05.
Correlation analysis among stenosis and patient-reported outcome measures
Lastly, Pearson product moment tests were performed to evaluate correlations among stenosis, DI, MMRC score, and VHI-10. All values were averaged within a given patient such that each patient was included only once in each analysis, and patients with more values available were not weighted disproportionately. Tests were 2-tailed with a significance level of α = .05.
Analyses were performed using SPSS software (IBM Corporation, Armonk, NY) and GraphPad Prism 9.3.1 (San Diego, CA).
Results
Data are presented as mean ± standard deviation unless otherwise specified.
Treatment Pathways
Sixty-four patients are included (Figure 1). All were female, including 62 Caucasians, 1 American Indian or Alaskan native, and 1 not answering. Average age was 48 ± 11 years at presentation and 55 ± 11 at data review. Of the 64 patients, 6 were managed only with SILSI. Thirty-one underwent endoscopic intervention(s) followed by SILSI and did not require other procedures. Sixteen underwent endoscopic intervention(s) followed by SILSI but required further operations or office-based procedures beyond steroid injection. Four patients were managed with intermittent endoscopic interventions only. Three patients underwent open airway surgery, including 2 patients who underwent laryngotracheal reconstruction with anterior cartilage graft for tracheal A-frame deformity in the setting of prior tracheotomy and one who underwent cricotracheal resection. Four patients had tracheostomy at time of data review.
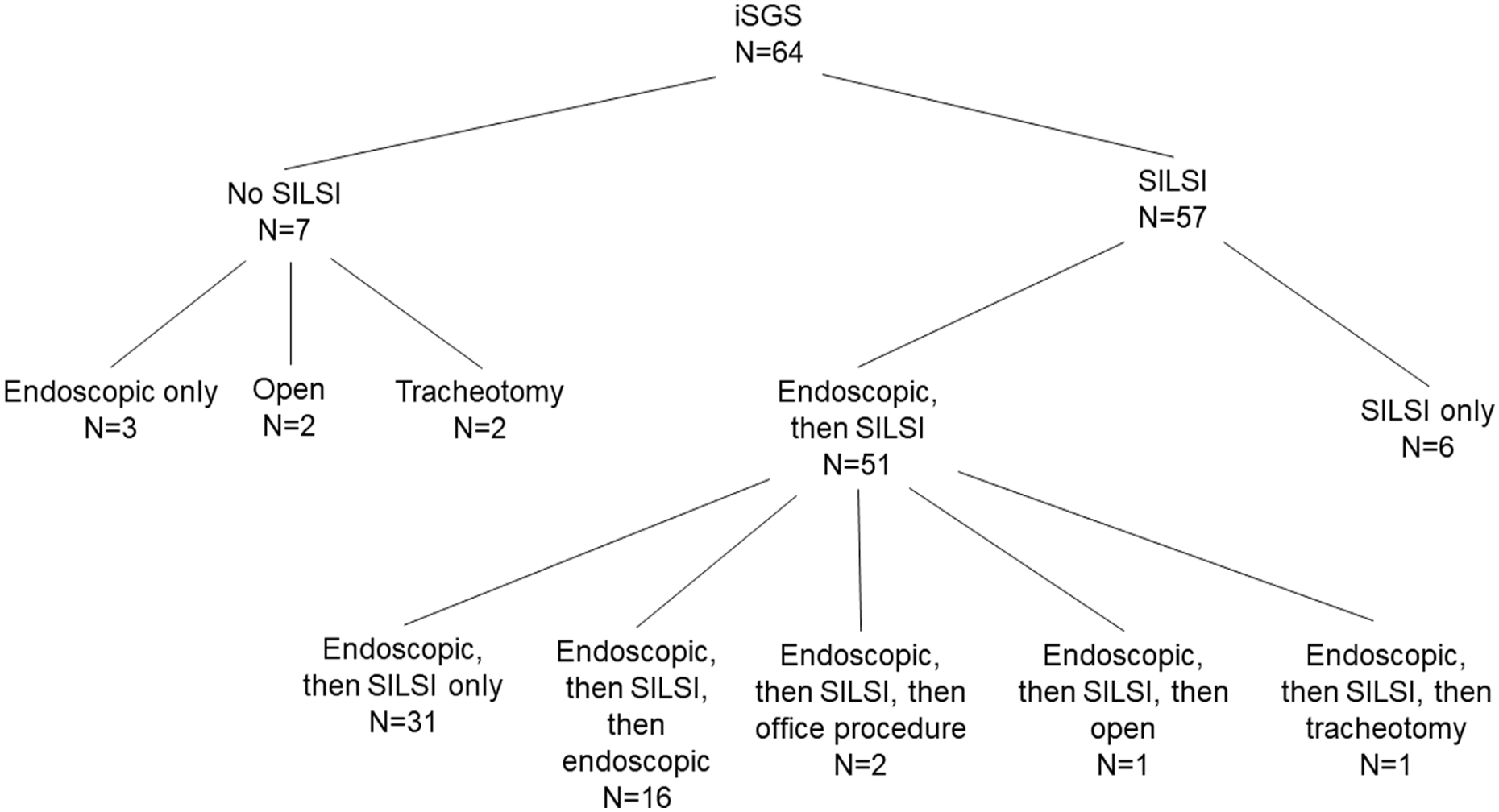
Flow chart depicting treatment pathways for patients in this study.
SILSI only
Six patients were managed exclusively with SILSI. Average age at time of treatment initiation was 47 ± 10 years. Patients underwent 1.7 ± 1.0 series of injections (range: 1, 3), with follow-up duration from completion of most recent injection being 584 ± 507 days, and time since initial visit being 922 ± 423 days. Stenosis decreased from 50% ± 15% to 20% ± 15% and dyspnea index decreased from 22 ± 13 to 7 ±8.
Endoscopic intervention(s) followed by SILSI only
Thirty-one patients were managed initially with endoscopic interventions and did not require procedures other than steroid injection after starting SILSI. Age at treatment initiation was 51 ± 10 years. Patients underwent 2.1 ± 1.6 endoscopic operations (range: 1, 7) prior to starting SILSI, followed by 2.5 ± 1.3 series of steroid injections (range: 1, 5). SILSI was started 185 ± 264 days (median: 63 days) after the last endoscopic intervention. For patients who underwent at least 2 endoscopic interventions, most recent inter-operative interval prior to SILSI was 987 ± 862 days (median: 639 days). Time from final endoscopic intervention to most recent follow-up visit (inclusive of all SILSI-related visits) for the same group was 1435 ± 871 days (median: 1248 days). Patients had baseline estimated stenosis of 60 ± 20% (median: 60%) and dyspnea index of 30 ± 7 (median: 30).
Additional intervention(s) following SILSI
Sixteen patients underwent additional endoscopic or office-based interventions other than steroid injection after starting SILSI. Patients were aged 45 ± 11 years (median: 43 years) and underwent 3.3 ± 2.4 endoscopic interventions (median: 2.5) prior to SILSI and 2.3 ± 1.3 interventions following SILSI (median: 2). Patients underwent 4.4 ± 1.8 (median: 4; range: 2, 7) series of SILSI over the data review period.
Of the sixteen, twelve returned to the operating room. Four underwent additional office-based procedures without operative intervention. This included 1 scar lysis with cup forceps, 1 flexible CO2 laser division of anterior scar, and 2 scar incisions using the KTP laser. These patients are included in data review for completeness and in correlation analyses, but are not included in inter-operative interval analysis.
Of the 12 patients that returned to the operating room, 9 underwent at least 2 endoscopic operations prior to SILSI allowing for calculation of a pre-SILSI and post-SILSI inter-operative interval. For those patients, pre-SILSI inter-operative interval was 523 ± 303 days (median: 504 days) and post-SILSI inter-operative interval was 814 ± 322 days (median: 794 days).
Open airway surgery
Three patients underwent open surgery, including 1 who underwent outside cricotracheal resection and 2 with prior tracheostomy who underwent laryngotracheal reconstruction with anterior costal cartilage graft for A-frame deformity.
Tracheostomy
Seven patients underwent tracheostomy, including 4 with tracheostomy at time of data review and 3 who were decannulated. Two patients with tracheostomy still present had recalcitrant disease despite frequent interventions and 2 lived far from medical care and elected to keep the tracheostomy. Two patients who were decannulated underwent endoscopic intervention followed by SILSI, followed by decannulation and then laryngotracheal reconstruction with costal cartilage graft for an A-frame deformity. The third patient was be decannulated following endoscopic interventions and SILSI.
Comparison of 2 Patient Groups: Those Undergoing SILSI Who Required Additional Interventions and Those Who Did Not
Patients did not differ according to age (U = 281; P = .1385), stenosis at time of SILSI (U = 351; P = .9964), DI at time of SILSI (U = 81; P = .5627), or time lapse between endoscopic dilation and SILSI (U = 300.5; P = .8596) (Table 1). Patients not requiring additional procedures underwent fewer procedures prior to starting SILSI (U = 212.5; P = .0056) and had a longer pre-SILSI inter-operative interval (U = 48; P = .0377).
Comparative Patient Characteristics for Patients Undergoing SILSI Who Did Not (“SILSI only”) and Did Undergo Additional Procedures (“Addl. Proc.”) Other Than Steroid Injection After Initiating SILSI.
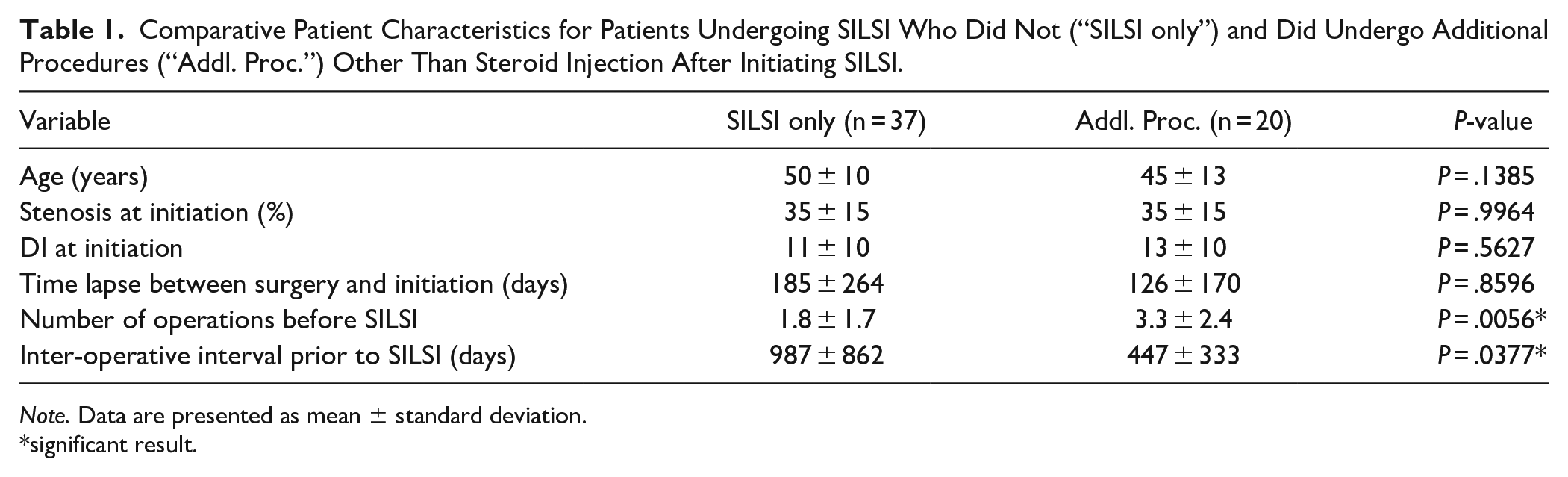
Note. Data are presented as mean ± standard deviation.
significant result.
Effect of SILSI on Inter-Operative Interval
Among patients undergoing at least 2 operations prior to SILSI, inter-operative interval increased from 550 ± 305 days to 1322 ± 797 days (t = 4.116; P = .0007; 95% confidence interval: 377, 1169) (Figure 2).
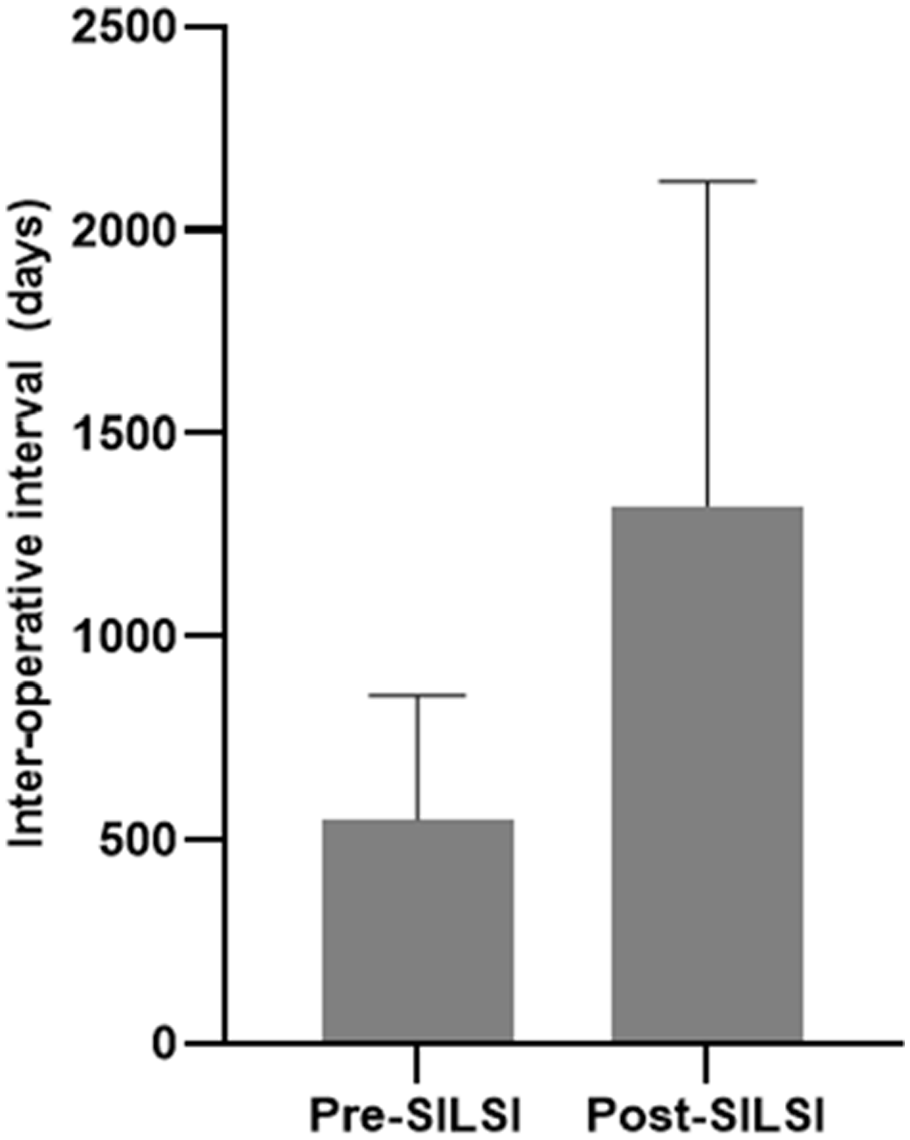
Average inter-operative interval before and after initiating SILSI for patients with at least 2 operations prior to starting SILSI. Bar height is mean and error bar represents standard deviation.
Effect of SILSI on Airway Stenosis and Patient-Reported Outcome Measures
Among patients undergoing at least one series of SILSI, significant decreases occurred in percent stenosis (n = 58; t = 6.523, P < .0001; 95% CI: −15, −8), DI (n = 55; t = 4.890; P < .0001; 95% confidence interval: −5.6, −2.3), MMRC score (n = 55; t = 4.132; P = .0001; 95% confidence interval: −0.5, −0.2), and VHI-10 score (n = 55; t = 2.298; P = .0255; 95% confidence interval: −2.1, −0.1) (Figures 3-5). Improvement in each parameter was greater in patients who did not require subsequent operative interventions after starting SILSI compared to those that did.
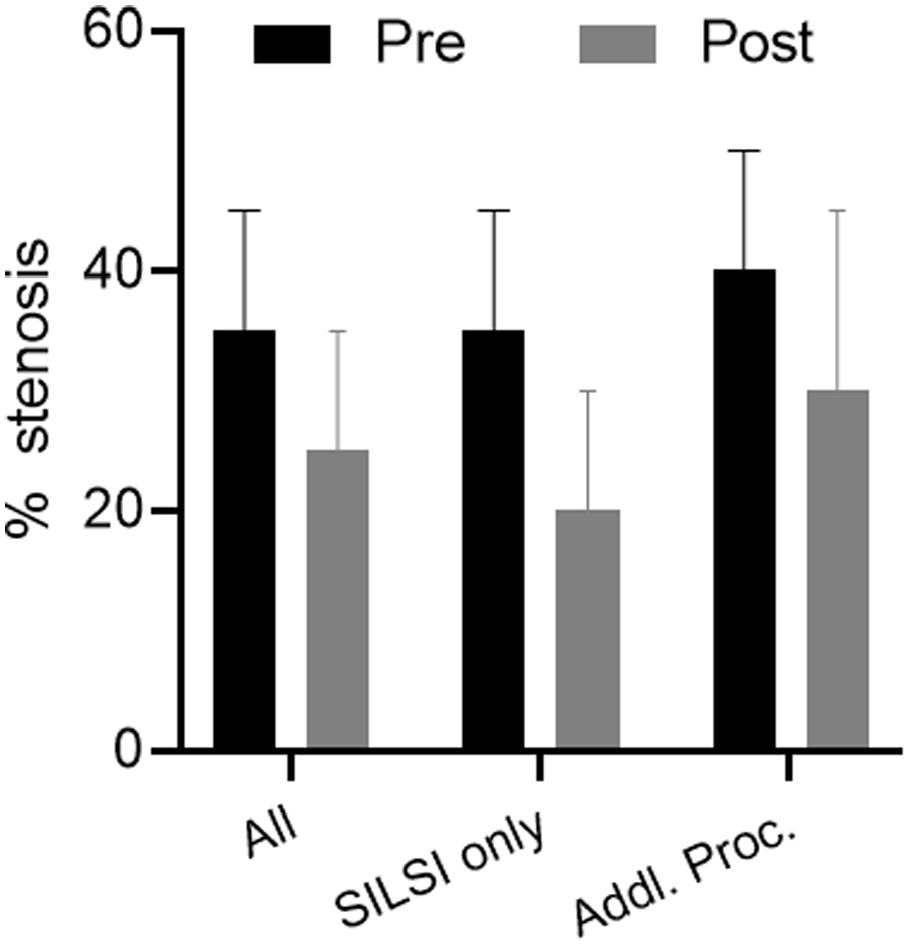
Average change in estimated percent airway stenosis for one SILSI series. Data are presented for all patients, those who did not require additional procedures after starting SILSI (“SILSI only”), and those who did require additional procedures (“Addl. Proc.”). Bar height is mean and error bar represents standard deviation.
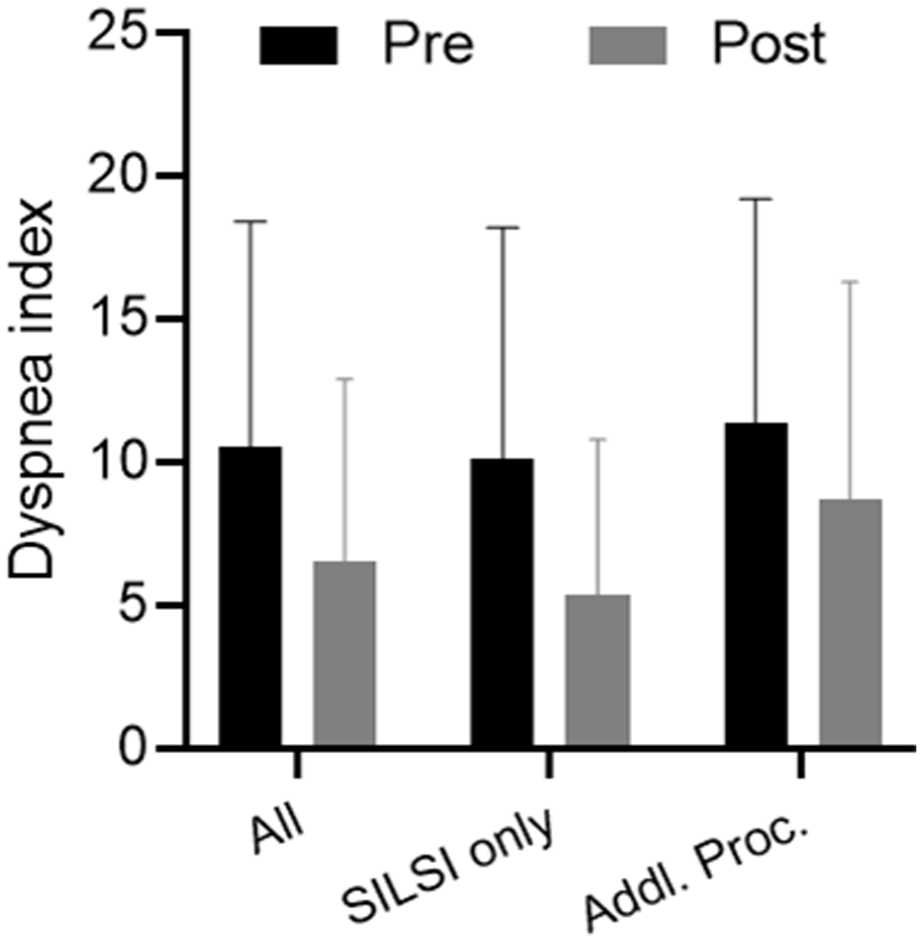
Average change in dyspnea index for one SILSI series. Data are presented for all patients, those who did not require additional procedures after starting SILSI (“SILSI only”), and those who did require additional procedures (“Addl. Proc.”). Bar height is mean and error bar represents standard deviation.
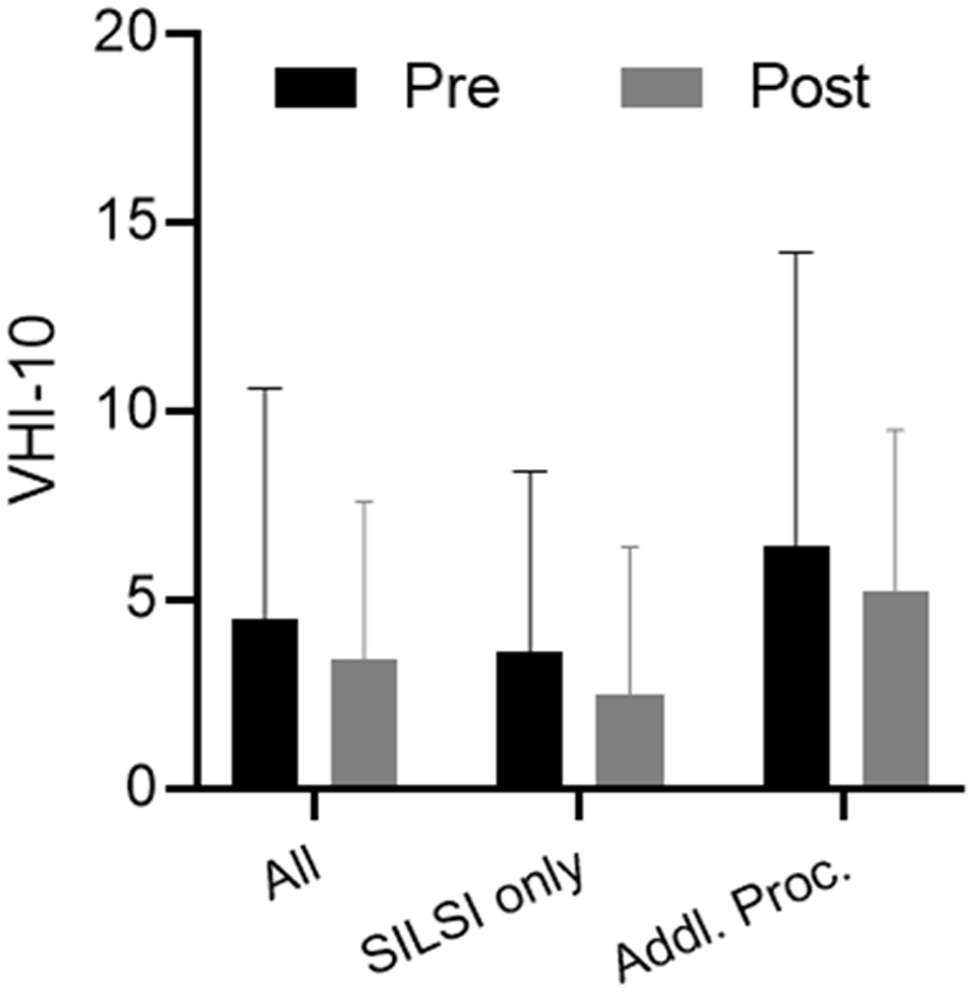
Average change in voice handicap index-10 for one SILSI series. Data are presented for all patients, those who did not require additional procedures after starting SILSI (“SILSI only”), and those who did require additional procedures (“Addl. Proc.”). Bar height is mean and error bar represents standard deviation.
Correlation Analysis Among Airway Stenosis and Patient-Reported Outcome Measures
Estimated stenosis was not correlated with the patient-reported outcome measures. Correlation coefficient was highest for MMRC score (r = .255; P = .051). DI was correlated with MMRC score (r = .625; P < .001) and VHI-10 (r = .532, P < .001). MMRC score was correlated with VHI-10 (r = .270, P = .039).
Discussion
iSGS is a unique entity within laryngotracheal stenosis.4,5 Introduction of SILSI by Franco et al 12 changed how patients can be counseled and treated. At our institution, most patients undergo SILSI. Implementation of a consistent protocol with close follow-up and patient-reported outcome measures allows for multi-parametric evaluation of outcomes. Initial single-institution studies evaluating the effect of SILSI on iSGS included 10 to 19 patients.12-15 More recent studies focusing on side effects and changes in voice-related quality of life and peak expiratory flow have included 49 and 55 patients.16,24 Of the 64 patients in this study, 57 underwent SILSI, allowing for evaluation of effects on stenosis, inter-operative interval, and patient-reported dyspnea and voice impairment in a relatively large group.
Potential benefits of SILSI include prolongation of inter-operative interval and longer periods of time spent with less airway stenosis and consequently lower symptom burden. Thirty-seven of fifty-seven patients who initiated SILSI did not require subsequent operative intervention. Further, interoperative interval increased among all patients undergoing at least 2 operations prior to SILSI, including those who did and did not return to the operating room. Of note, inter-operative interval as an outcome measure has inherent limitations due to clinician- and patient-related subjectivity associated with that decision. Additionally, decreased estimated stenosis, DI, MMRC, and VHI-10 score were observed following a SILSI cycle across all patients. Predictably, improvements were less notable among patients requiring procedures beyond SILSI.
SILSI is a voice-preserving treatment option. Our initial study on VHI-10 scores did not demonstrate a change in 16 patients, 14 while a small, statistically significant change was observed in 55 patients here. Small improvements in voice-related quality of life were observed by Naunheim et al 16 Most importantly, there is not worsening of vocal function as may occur with cricotracheal resection or even occasionally in the setting of repeated direct microlaryngoscopic procedures.
SILSI has some inherent limitations. First, it requires substantial time investment by patient and clinician. Second, there is non-negligible systemic steroid exposure. This can lead to menstrual irregularities, changes in mood or energy, or difficulty sleeping. 24 Suppression of the hypothalamic-pituitary axis is a potential concern, though cortisol may normalize within 7 days. 25 There is one case report of a patient developing Cushing syndrome. 26 Care should be taken in patients with diabetes, as studies on epidural steroid injection have shown increases in glucose by over 100 mg/dl for 2 days. 27 Lastly, not all patients appear to benefit from SILSI and a recent multi-institutional study did not show a comparative benefit for heterogeneously implemented SILSI on time to recurrence, peak expiratory flow, or clinical COPD questionnaire scores. 17 Accordingly, identifying which patients are most likely to benefit is desirable. In our dataset, 2 measures reflecting pre-SILSI disease severity (number of operations prior to SILSI and most recent inter-operative interval) predicted higher likelihood of needing additional procedures after starting SILSI. Stenosis or dyspnea index at time of first injection were not significant predictors. Identification of patient serologic or histopathologic features predicting response to SILSI would be helpful in guiding counseling and clinical decision-making.
A less frequently described benefit of SILSI is use as a prognostic tool. Patients have multiple treatment pathways available, including close observation, SILSI, endoscopic dilation, open surgery, and tracheotomy. Given reported benefit of SILSI in at least a subset of patients as well as the variable recurrence rate after endoscopic surgery, it is reasonable to attempt one or both of these more conservative therapies first prior to discussing potential open surgery. As shown here, some patients have lasting benefit following a limited number of injections and would not be recommended to undergo a more invasive procedure. Along the same rationale, patients who recur rapidly despite adjuvant steroid injections are more likely to have a risk/benefit ratio favoring more invasive procedures. Patients who tolerate SILSI and wish to avoid the operating room are also candidates for other office-based interventions, including cold or laser-based division of thin scar bands as described in select patients in this study. Office-based balloon dilation has also been described and is an option in select highly cooperative patients. 28 This intervention is not currently performed at our institution.
Open surgery was performed in 3 patients, including one outside cricotracheal resection and 2 laryngotracheal reconstructions. While cricotracheal resection is the more commonly described open operation in this population, it has risks including anastomosis dehiscence, voice change, significant perioperative care, edema, recurrent laryngeal nerve injury, and recurrence. Laryngotracheal reconstruction with an anterior graft is helpful in setting of comorbid A-frame deformity and creates a subglottis which is supra-normal in diameter, thus allowing for greater reserve and increased tolerance of stenosis within the neo-subglottis.
Seven patients underwent tracheostomy, including 4 who remained tracheostomy-dependent. Although performed less commonly for idiopathic stenosis, tracheostomy remains an option for management of all airway stenosis. There was no mortality within this cohort. Patients who elected to remain tracheostomy-dependent had complicating clinical factors, including long distance from medical care or refractory disease that recurred quickly despite frequent operative and office-based interventions.
Several limitations are noted. This is a retrospective series. Additionally, routine peak expiratory flow measurements were not available. Lastly, this is a single institution study, which provides benefit in being able to describe outcomes for a fairly uniform SILSI protocol, but decreases generalizability. Prospective randomized trials evaluating the impact of SILSI and determining which patients may be most likely to benefit are warranted.
Conclusion
These data provide information which may help guide counseling on outcomes for multiple treatment pathways. Specifically, impact of a single institution SILSI protocol had significant impacts on inter-operative interval as well as patient-reported measures of dyspnea and dysphonia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.