
Abstract
Background:
About 80% of congenital hearing loss cases have genetic causes, often autosomal recessive and non-syndromic. Autosomal Recessive Non-syndromic hearing loss is characterized by extreme genetic heterogeneity.
Objectives:
To report a case of congenital hearing loss with novel homozygous deletion in GRXCR1 gene.
Methods:
Case reports and review of literatures.
Results:
In this study, the proband was a 32-year-old woman seeking pre-marriage genetic counseling with non-syndromic congenital hearing loss. An owing negative test for GJB2 mutations, she underwent exome sequencing, unveiling a novel homozygous exon 2 deletion of the GRXCR1 gene. This mutation was confirmed in her affected mother and sibling by PCR and Quantitative Real-Time PCR.
Conclusion:
We identified a novel GRXCR1 gene mutation related to congenital hearing loss in a family. Our study highlights the efficiency of exome sequencing in discovering gene mutations in cases of diseases with genetic heterogeneity.
Introduction
Congenital hearing loss is one of the most common neurosensory disorders, with an incidence of 1 to 3 per 1000 newborns worldwide. Genetic hearing losses account for approximately half of cases and are mainly non-syndromic with autosomal recessive inheritance. 1
Autosomal Recessive Non-syndromic hearing loss (ARNSHL) is characterized by extreme genetic heterogeneity; since the first report in 1997, mutations in 78 genes have been identified to be involved in ARNSHL (http://hereditaryhearingloss.org).
In 2010, Schraders et al 2 revealed that mutations in glutaredoxin and cysteine-rich domain containing 1 (GRXCR1) gene underlie ARNSHL. To the best of our knowledge, all reported GRXCR1 mutations so far were point mutations.3-5 Here, we report a case of ARNSHL with a homozygous deletion of exon 2 in the GRXCR1 gene, identified through exome sequencing. Segregation analysis was performed using PCR and quantitative Real-Time PCR.
Case Presentation
The proband was a 32-year-old woman with congenital hearing loss referred to our clinic for genetic counseling before marriage. She was the child of a cousin consanguineous parents. Her mother and one of her siblings had hearing loss (Figure 1A).
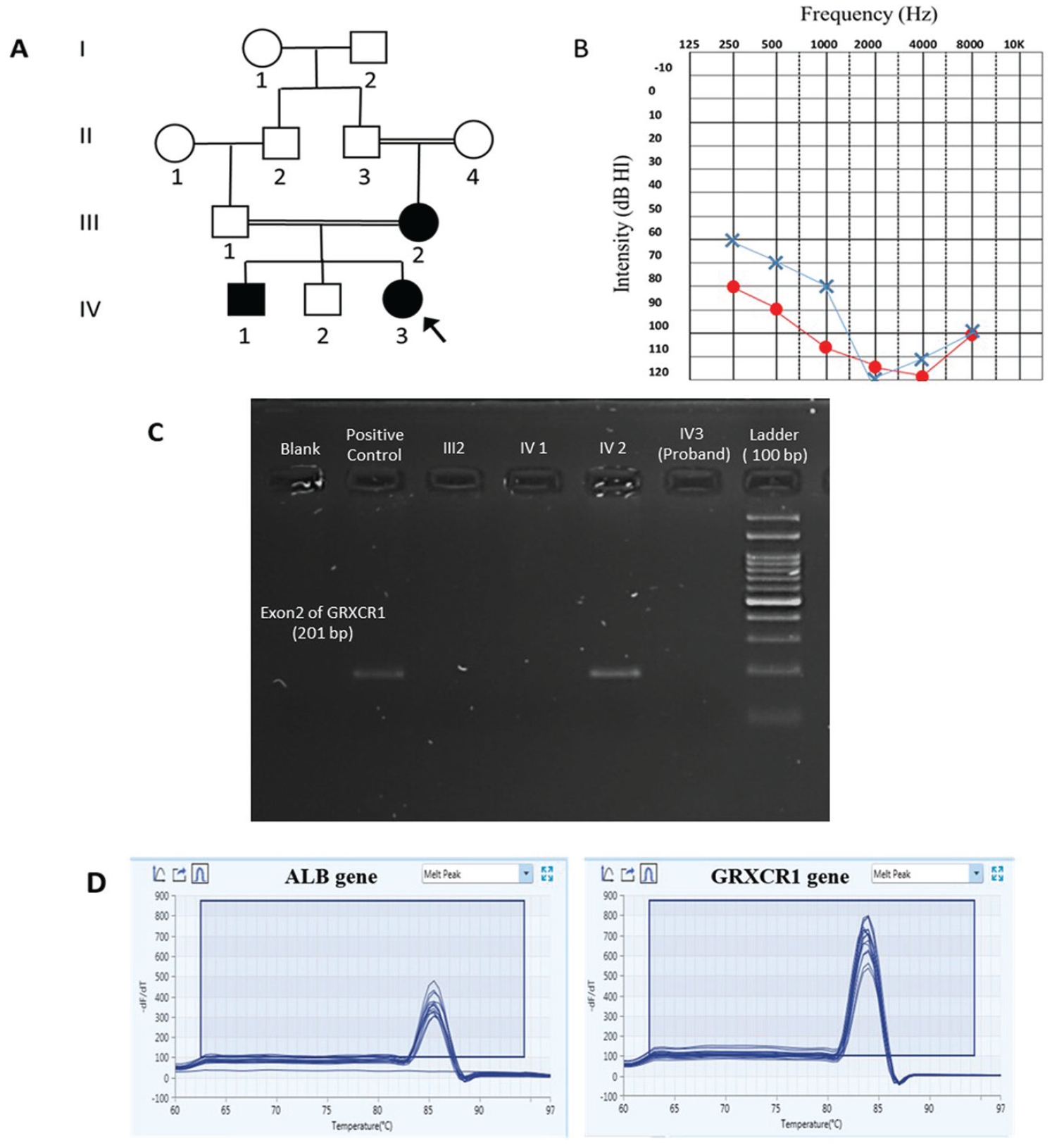
Summary of clinical and molecular genetic analyses (A) Pedigree of an affected family with non-syndromic hearing loss. The arrow denotes the proband, and darkened symbols represent the affected members. (B) Audiogram of the affected proband indicates air conduction for right [o] and left ear [x]. (C) Results of the PCR-electrophoresis analysis in the proband, affected, and healthy member of the family. (D) The Real-Time-PCR product melting curve analysis result for ALB and GRXCR1 genes.
The patient had a normal Tympanogram, type A, in both ears. Her audiogram report indicated symmetric air conduction levels up to 120 dB at 4 kHz (Figure 1B). In the clinical examination and past medical history, she had no other health problems representing a syndromic hearing loss.
Using a standard salt-chloroform protocol, genomic DNA was extracted from the proband, affected mother, and 2 siblings, including one healthy brother as a control.
Based on Sanger sequencing, the proband was negative for mutations in the GJB2, the most common worldwide ARNSHL gene. Therefore, exome sequencing was performed on her genomic DNA with the Agilent SureSelect V7 Kit on an Illumina NovaSeq TM 6000 platform (Illumina Inc., San Diego, CA, USA), yielding paired-end 150 bp sequence reads The exome sequencing data analysis using the Integrative Genomics Viewer (IGV) app revealed a homozygous deletion of 15 091 bp at loci chr4: 42 955 467-42970558 (GRCH37/hg19) that encompasses the exon 2 and surrounding DNA sequences in flanking introns of the GRXCR1 gene.
We designed a pair of primers to verify this deletion: F: ATTTATACCACCTGCCTTCGTGTG and R: GTAATGGCCATCAATGAACACAA to amplify exon 2 of the GRXCR1 gene specifically. Then Polymerase Chain Reaction (PCR) was carried out at an annealing temperature of 63°C, generating amplicons of 201 bp in length. This deletion was confirmed using PCR and Electrophoresis of PCR products on a 2% agarose gel in the proband and her affected family members. Her healthy brother was negative for this homozygous mutation (Figure 1C).
Copy numbers of the GRXCR1 exon 2 were determined in the proband and her family (parents and siblings) by SYBR Green-based real-time PCR assay. 6 The method involves the amplification of the ALB (Albumin) gene as a reference gene on chromosome 4 and GRXCR1 exon 2.
The sequences of real-time PCR primer pairs were as follow: GRXCR1: (F: ATACCACCTGCCTTCGTGTG, R: TTCAGAAACTCGTCGGCATCG) and ALB: (F: AGCTATCCGTGGTCCTGAAC, R: TTCTCAGAAAGTGTGCATATATCTG). The reaction mixture contained 10 μL SYBR Green Master Mix, 1.25 μL of each primer (250 nM), 1 μL template DNA (50 ng), and 6.5 μL of water to reach a final reaction volume of 20 μL. The assay included the proband and her family’s genomic DNA, a healthy person’s genomic DNA as a reference DNA, and a no-template control in duplicate.
The thermocycling conditions were as follows: 5 minutes at 95°C, 40 cycles of 15 seconds at 95°C and 60 seconds at 60°C. After PCR amplification, the specificity of the PCR reaction was checked by generating a melting curve for every PCR product.
Copy numbers of GRXCR1 were calculated by the delta-delta CT method. Our analysis revealed a deletion of both copies of exon 2 of the GRXCR1 gene in the proband and her affected mother and sibling, and one copy of it in her father and healthy brother.
Discussion
In a patient with congenital hearing loss, we identified a novel mutation in the GRXCR1 gene, homozygous deletion of exon 2. Using PCR and quantitative Real-Time PCR method, this mutation was confirmed in the affected mother and brother.
Previous studies have reported 10 pathogenic point mutations in the GRXCR1 gene in cases with severe-to-profound non-syndromic hearing loss, of which 3 mutations were located in exon 2 (Table 1). To our knowledge, there is no previous report on this gene’s homozygous deletion of exon 2.
Overview of the Reported GRXCR1 Mutations in Patients With Non-Syndromic Hearing Loss.
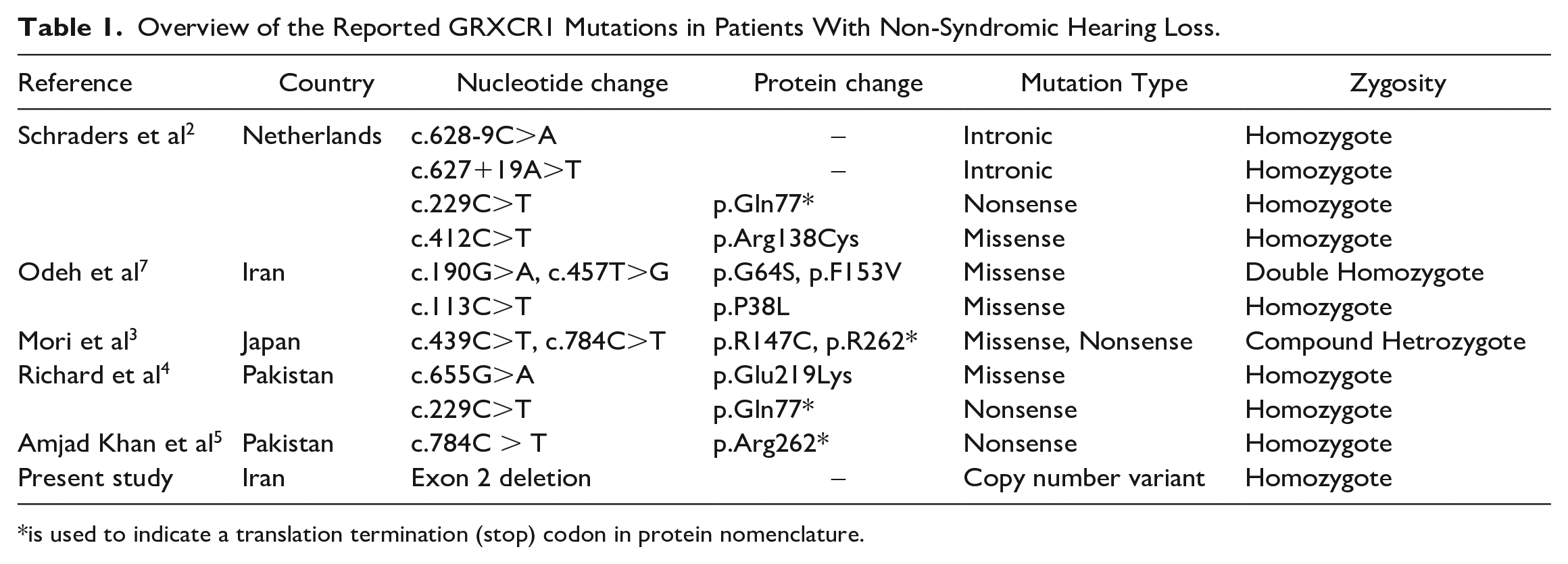
is used to indicate a translation termination (stop) codon in protein nomenclature.
GRXCR1 is expressed in the inner ear sensory epithelia, and its encoded protein is diffused throughout the stereocilia length. This protein contains GRX-like domains, encoded by exon 2, that may play a role in actin organization in hair cells through S-glutathionylation. The intact architecture of hair cell stereocilia is needed for normal hearing. Odeh et al. 7 showed that homozygous Loss of function of Grxcr1 results in the formation of abnormal stereocilia in the inner hair cells of pirouette mice.
In conclusion, we identified a novel GRXCR1 gene mutation related to congenital hearing loss in an Iranian family. In addition, our study highlights the efficiency of exome sequencing in discovering gene mutations in cases of diseases with genetic heterogeneity.
Footnotes
Acknowledgements
Researchers appreciated the Clinical Research Development units of Kamali and Rajaee at Alborz University of Medical Sciences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.