
Abstract
Objectives:
To assess novel morphometric measurement strategies and observer perception ratings as potential metrics for evaluating gender-affirming transvestibular chondrolaryngoplasty in reducing contour protrusion of the neck.
Methods:
High-resolution preoperative and 3-month postoperative photographs of a pilot series of 10 patients (n = 10) who underwent endoscopic transvestibular chondrolaryngoplasty were collected. Morphometric measurements of “light reflex” and lateral view thyroid protrusion angles of the neck contours were analyzed. Pre- and postoperative photographs were presented in random order in a survey to 17 untrained judges and rated on perceived masculinity/femininity and thyroid notch protrusion on a 7-point scale. A pre- to postoperative change in morphometric angles and subjective ratings was assessed using paired t-tests and Wilcoxon signed-rank tests.
Results:
Mean light reflex angles were reduced after surgery from 78.6° to 40.5° in the anterior neutral view (P = .0003), from 45.2° to 24.4° in the anterior extended view (P = .003), and from 7.03° to 4.32° in the lateral view (P = .006). Median survey ratings of neck photographs were improved after surgery, from 4 to 3 in gender perception toward more feminine perception (P < .0001) and from 4 to 2 in thyroid protrusion toward less protrusive perception (P < .0001).
Conclusions:
Morphometric analysis in anterior and lateral views as well as subjective gender perception and contour protrusion measures following feminization chondrolaryngoplasty by endoscopic transvestibular scarless approach demonstrate encouraging possibilities as outcome evaluation measures for chondrolaryngoplasty.
Keywords
Introduction
Chondrolaryngoplasty, commonly referred to by the anatomical misnomer “tracheal shave,” is a surgical procedure aimed toward reducing the neck contour deformity caused by the laryngeal prominence of the thyroid cartilage. It is a surgery primarily offered for transgender patients seeking gender-affirming surgical care. 1 Since its earliest introduction into the literature in 1975, chondrolaryngoplasty is typically performed through a transcervical incision and has been met with excellent safety and efficacy measures.1 -3 Patient satisfaction with transcervical chondrolaryngoplasty has been reported from 60% to 98%.4,5 In recent years, a transvestibular approach to chondrolaryngoplasty has allowed for laryngeal prominence reduction without visible evidence of a surgical scar and has similarly demonstrated great safety and efficacy.6 -10
Prior studies on chondrolaryngoplasty outcomes have primarily relied on patient-reported outcome measures (PROMs) as evaluation metrics. 11 Cohen et al designed an outcomes instrument based on previously published and validated outcome instruments utilized in facial plastic surgery, consisting of 7 questions, 6 of which assessed patient satisfaction and quality of life postoperatively on a 5-point Likert scale.4,12 Amir et al investigated observer visual gender perception of the neck by using untrained judges to evaluate standardized photographs of cis-men and cis-women. They did so through a 3-question survey assessing the degree of masculinity or femininity of each photograph. 13
Yet published outcome measures for other cervicofacial reconstructive procedures such as rhinoplasty and skin rejuvenation have been combined with objective quantitative tools.14 -16 However, to date, there have been few measurement tools beyond PROMs and no objective measurement tools evaluating chondrolaryngoplasty outcomes. Our group therefore sought out to conduct a small proof of concept pilot study to help elucidate what kinds of new objective and subjective evaluation methods may warrant further exploration and development.
In this pilot study, we aim to test the use of several objective and subjective measures of the neck contour changes on pre- and postoperative standardized photographs of a series of patients who underwent endoscopic transvestibular chondrolaryngoplasty. Specifically, we test objective “light reflex angle” and thyroid protrusion angles and subjective third-party observer grading of gender specific contour and thyroid protrusion. We hypothesized that these objective and subjective measures would reflect a reduction in thyroid cartilage protrusion and more feminine neck appearance after chondrolaryngoplasty.
Materials and Methods
A retrospective review was performed reviewing all patients who underwent endoscopic transvestibular chondrolaryngoplasty over 24 months. From this database, 10 patients with available high resolution preoperative and greater than 3-month-postoperative photography were identified. This study was approved by the University of California Los Angeles (UCLA) Institutional Review Board (IRB# 11-000925).
All patients underwent endoscopic transvestibular chondrolaryngoplasty (“scarless”). The surgical technique is described in detail elsewhere,9,10 but briefly, the procedure proceeds through a 4 cm lower labial incision, 1 cm anterior to the gingivobuccal sulcus. The pocket is dissected with direct visualization deep to the mental soft tissue to connect with the subplatysmal cervical space. With 30-degree down-angled endoscopy the pretracheal strap musculature is exposed to identify the thyroid cartilage notch. Using endoscopic rongeurs and a surgical burr, the superior thyroid cartilage of the notch and lateral ala are resected until optimal contour is achieved.
Objective Measures
We tested the “light reflex” angle and the thyroid protrusion angle as objective measures for evaluating a change to thyroid cartilage protrusion after chondrolaryngoplasty in anterior and profile views respectively. The “light reflex angle” is a visible angled pattern of shadows/lights created by patients’ thyroid cartilage anatomy in an anterior view; this was patterned after a similar visual analysis technique used in rhinoplasty. 17 The thyroid protrusion angle is the visible protrusion of the thyroid cartilage beyond the profile of the neck, chosen as a lateral view measurement of laryngeal prominence.
Objective morphometric analysis was performed on preoperative and postoperative standardized photographs of 10 (n = 10) subjects captured in a professional photography setting. These images were analyzed using an open-source freeware image editing software GIMP (GNU Image Manipulation Program) 18 which allowed us to the highlight the “light reflex angle” and thereby more accurately measure these changes.17,19 -21 Using the color selection and contrast enhancement tools, the borders of a “light reflex” created by the laryngeal prominence in the anterior and anterior extended views were delineated (see Figure 1). In these modified images, we then measured the angle created by the shadow/light borders at the thyroid notch in both the anterior and anterior extended views. In the lateral view, an additional measurement was performed in unmodified images. In this view, the angle between the anterior border of the neck—from the cervicomental angle to the sternal notch—and the anterior aspect of thyroid notch/laryngeal prominence was measured (Figure 2).
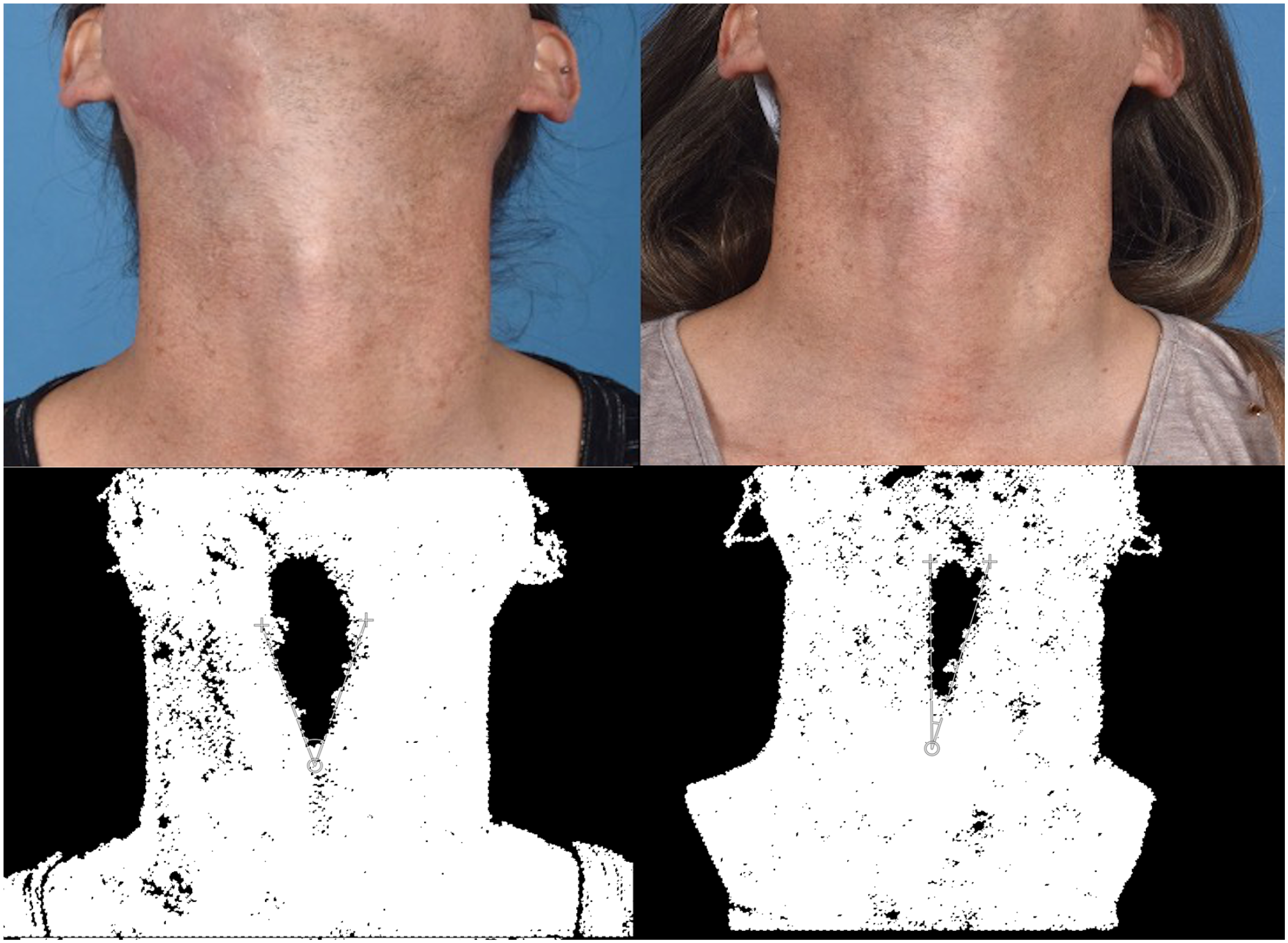
Preoperative (left) and postoperative (right) images in the anterior extended view. Below are color-selection and contrast-enhancement modifications applied to enhance visualization of the “light reflex” angle of the laryngeal prominence created by the shadow/light borders at the thyroid notch.
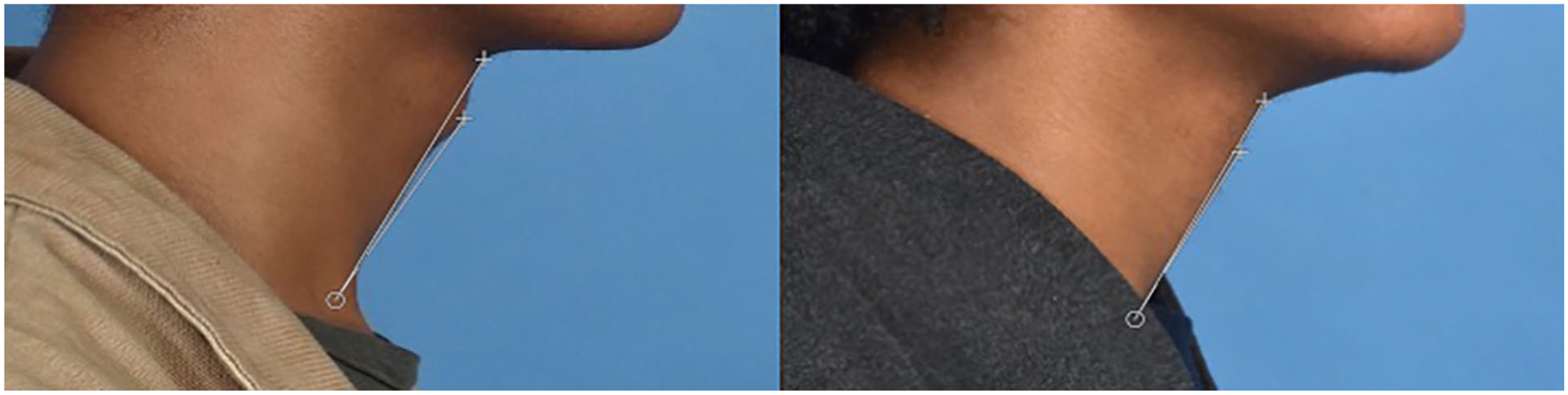
Unmodified photograph in lateral view with the thyroid protrusion angle or the visible protrusion of the thyroid cartilage beyond the profile of the neck (cervicomental angle to sternal notch).
Subjective Measures
For subjective measures, a survey was administered to 17 untrained judges to evaluate the photographs of the subjects (n = 9) regarding perception of masculinity/femininity and thyroid protrusion. These judges were recruited via convenience sampling of otolaryngology residents at an academic institution’s residency program. Pre- and postoperative photographs were randomized and presented to judges who were asked to rate the extent of masculinity and femininity using a 7-point scale (1 = “very feminine” to 7 = “very masculine”). Judges were also asked to rate the thyroid protrusion of the neck (1 = “not protruding” to 7 = “very protrusive”). This is similar to the 7-point rating scale approach to evaluating neck perceptions used by Amir et al. 13
Statistical Analysis
All statistical analyses were performed using Microsoft Excel (Microsoft Corporation, Renton, WA), SAS version 9.4 (SAS Institute, Cary, NC), and Stata version 17 (StataCorp LLC, College Station, TX). Morphometric results were calculated using means and standard deviations. Differences between pre- and postoperative morphometric results were assessed with the paired 2 sample t-test. Interrater reliability of survey judges was assessed using the intraclass correlation coefficient (ICC). ICC estimates were calculated based on a 2-way mixed-effects model, with a threshold of acceptable reliability set to 0.70. Ordinal survey rating results were calculated using medians and quartiles. Because 7-point survey ratings were considered as ordinal data, statistical analyses involving survey ratings utilized nonparametric tests. Differences between pre- and postoperative survey rating results for each subject were assessed using the Wilcoxon signed-rank test for paired ordinal data. Overall differences in pre- and postoperative perceived gender and thyroid protrusion were assessed with the Wilcoxon signed-rank test using the pooled survey ratings for all subjects. In addition to testing change in these objective and subjective measures following surgery, testing for potential correlations between objective and subjective measurements were performed using the Spearman correlation. Correlation testing was conducting between morphometric angle measurements in each view and median ratings of ordinal survey rating results of perceived gender and thyroid protrusion for each subject. These correlations were done for preoperative values, for postoperative values, and for changes in values from preoperative to postoperative. Significance level was set to .05, and 2-sided P-values are reported.
Results
Morphometric analysis of pre- and postoperative photographs (n = 10) demonstrated significant reduction in the lateral view angle and the angle created by light reflex due to the thyroid prominence in both the anterior neutral and anterior extended views (Table 1). Mean anterior neutral light reflex reduced from 78.6° preoperatively to 40.5° postoperatively (P = .0003). Mean anterior extended light reflex reduced from 45.2° preoperatively to 24.4° postoperatively (P = .003). Mean lateral thyroid protrusion angle reduced from 7.03° preoperatively to 4.32° postoperatively (P = .006). Therefore, objective morphometric measures in the anterior and lateral views were able to reflect changes in neck contour after chondrolaryngoplasty.
Morphometric Light Reflex and Lateral Angles (n = 10) and Overall Survey Ratings* of 9 Subjects (n = 9).
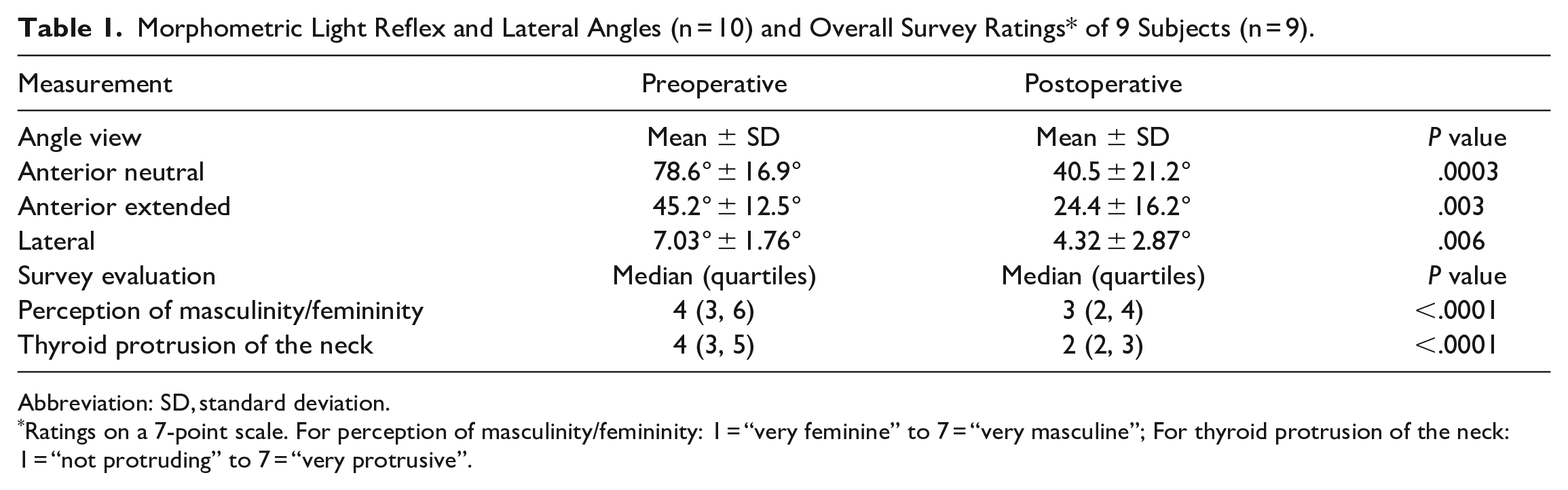
Abbreviation: SD, standard deviation.
Ratings on a 7-point scale. For perception of masculinity/femininity: 1 = “very feminine” to 7 = “very masculine”; For thyroid protrusion of the neck: 1 = “not protruding” to 7 = “very protrusive”.
The reliability of ratings from all 17 judges was excellent for subjectively evaluating photographs of the neck, with intraclass correlation coefficient greater than .90 for all 4 rating evaluations: pre- and post-operative gender perceptions and pre-and post-operative thyroid protrusion (Table 2). Judges were a mean age of 27.7-years-old. Ten judges identified as cisgender men and 7 judges identified as cisgender women.
Inter-rater Reliability of 17 Untrained Judges (n = 17).
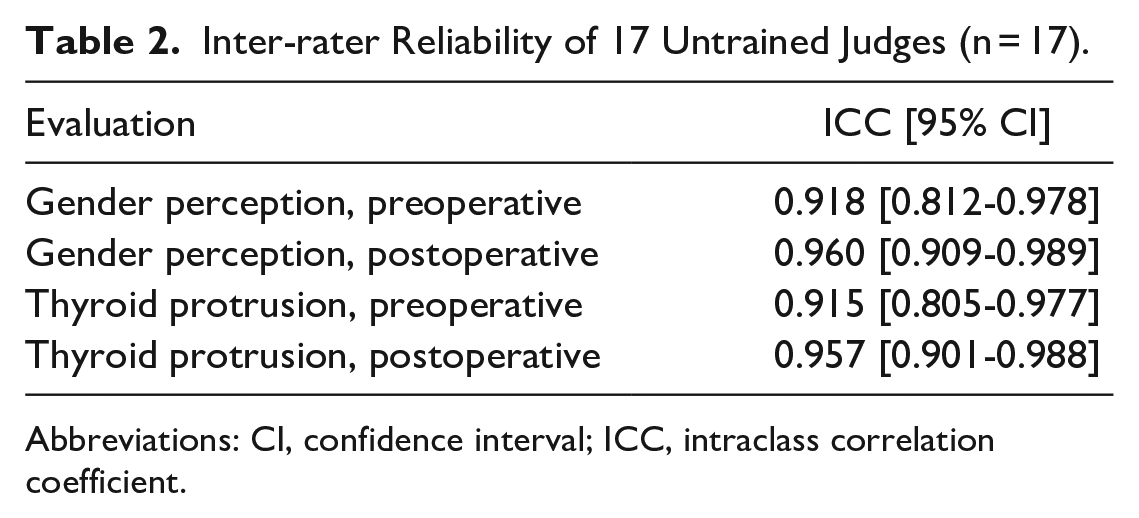
Abbreviations: CI, confidence interval; ICC, intraclass correlation coefficient.
Overall survey results of the subjective measures for the preoperative and postoperative photograph groups demonstrated significant trends toward a more feminine and less thyroid-protrusive perception of the neck after chondrolaryngoplasty (Table 1 and Figure 3). Overall, all the subjects’ necks were perceived as more feminine after surgery, decreasing from a median gender perception rating of 4 to a median rating of 3 (P < .0001). Overall, subjects were perceived as having less protrusive thyroid prominence after surgery, decreasing from a median thyroid protrusion rating of 4 to a median rating of 2 (P < .0001). For subjective rating results of individual subjects, 7 out of 9 subjects had a significant trend toward feminine gender perception (Figure 4) and a non-protrusive thyroid cartilage (Figure 5) after surgery.
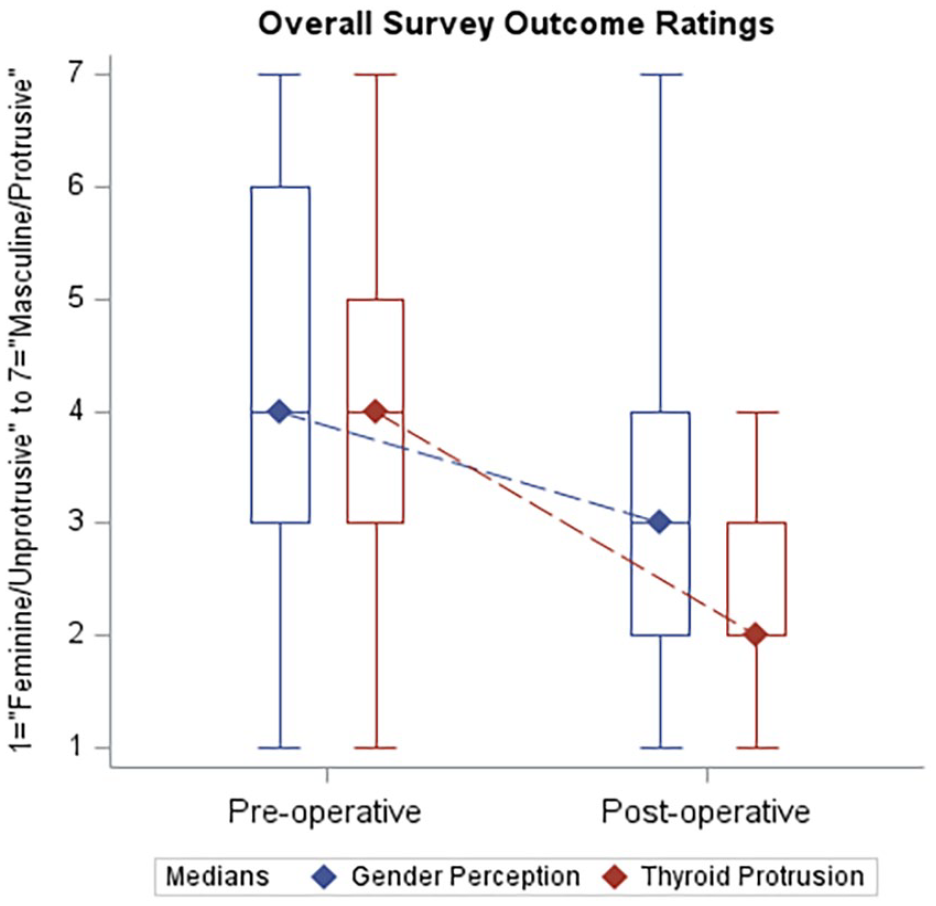
Overall pre- and post-operative survey ratings of gender perception (left) and thyroid protrusion (right). Ratings on a 7-point scale. For gender perception: 1 = “very feminine” to 7 = “very masculine”; For thyroid protrusion of the neck: 1 = “not protruding” to 7 = “very protrusive.” Dashed line between diamonds indicates change in median outcome rating.
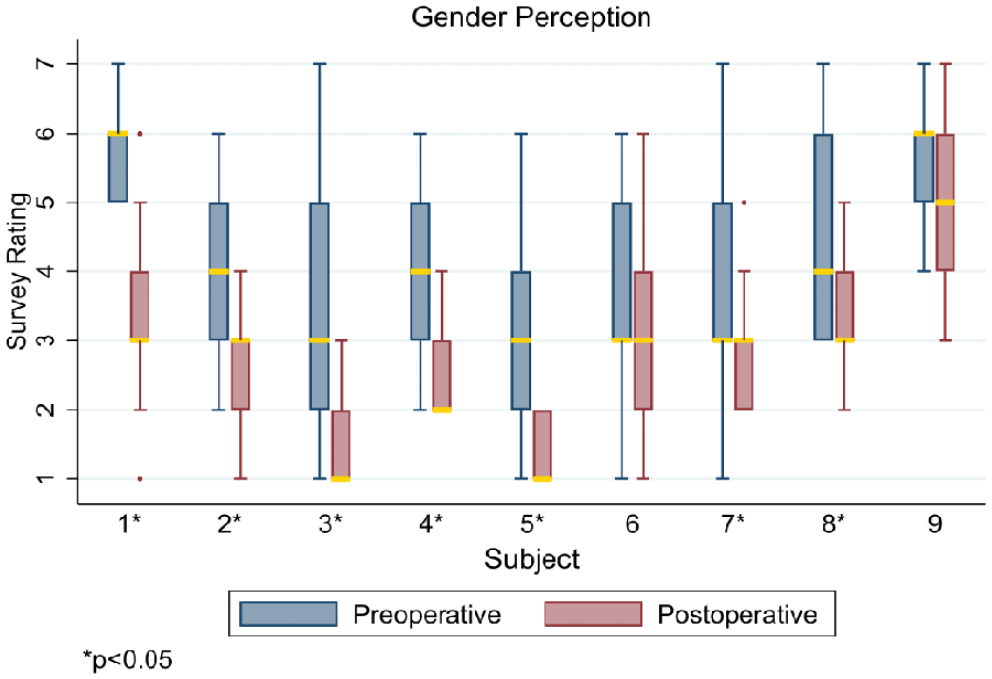
Survey ratings of gender perception (femininity/masculinity) before and after surgery, by subject. Ratings are on a 7-point scale, with 1 = “very feminine” to 7 = “very masculine”. Gold bar indicates median rating. *Denotes a significant difference after surgery.
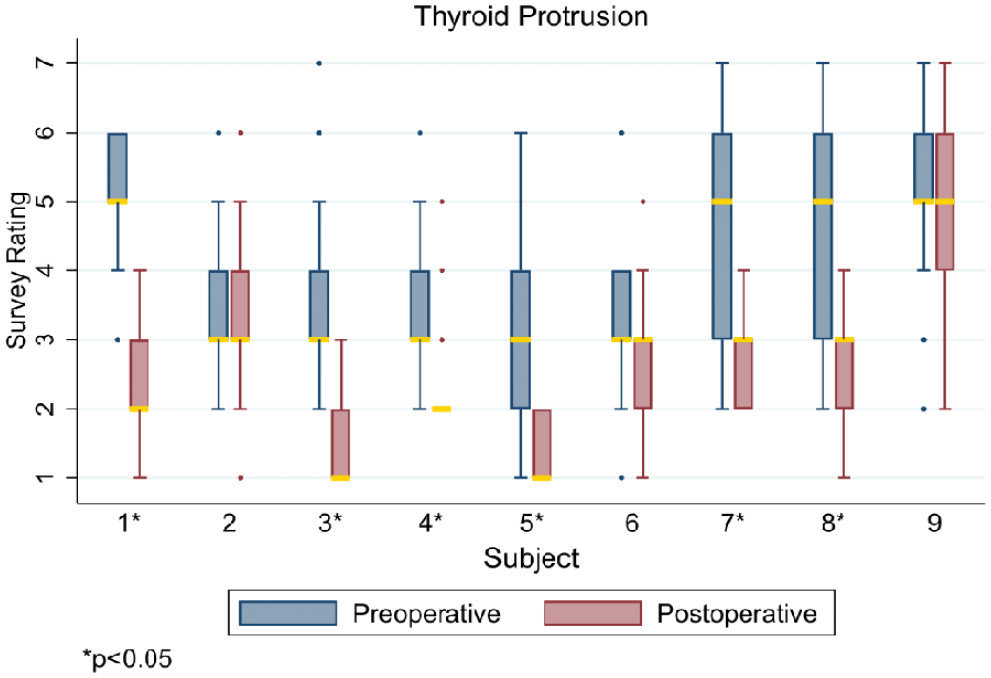
Survey ratings of thyroid protrusion before and after surgery, by subject. Ratings are on a 7-point scale, with 1 = “not protruding” to 7 = “very protrusive”. Gold bar indicates median rating. *Denotes a significant difference after surgery.
Correlation testing between objective and subjective measurements demonstrated morphometric thyroid protrusion angle in the lateral view was strongly correlated with thyroid protrusion rating in preoperative (r = .866, P = .003) and postoperative (r = .791, P = .01) photographs as well as gender perception rating in postoperative photographs (r = .853, P = .003) (Table 3). Thus, smaller postoperative morphometric angles in the lateral view were strongly correlated with more feminine and with less protrusive thyroid notch ratings of the neck after surgery. The “light reflex angles” in the anterior and anterior extended views were not statistically significantly correlated with either subjective measurement.
Spearman Correlation Tests for Correlations (rho) Between Objective Measurements and Subjective Ratings for Preoperative, Postoperative, and Change in Measures.
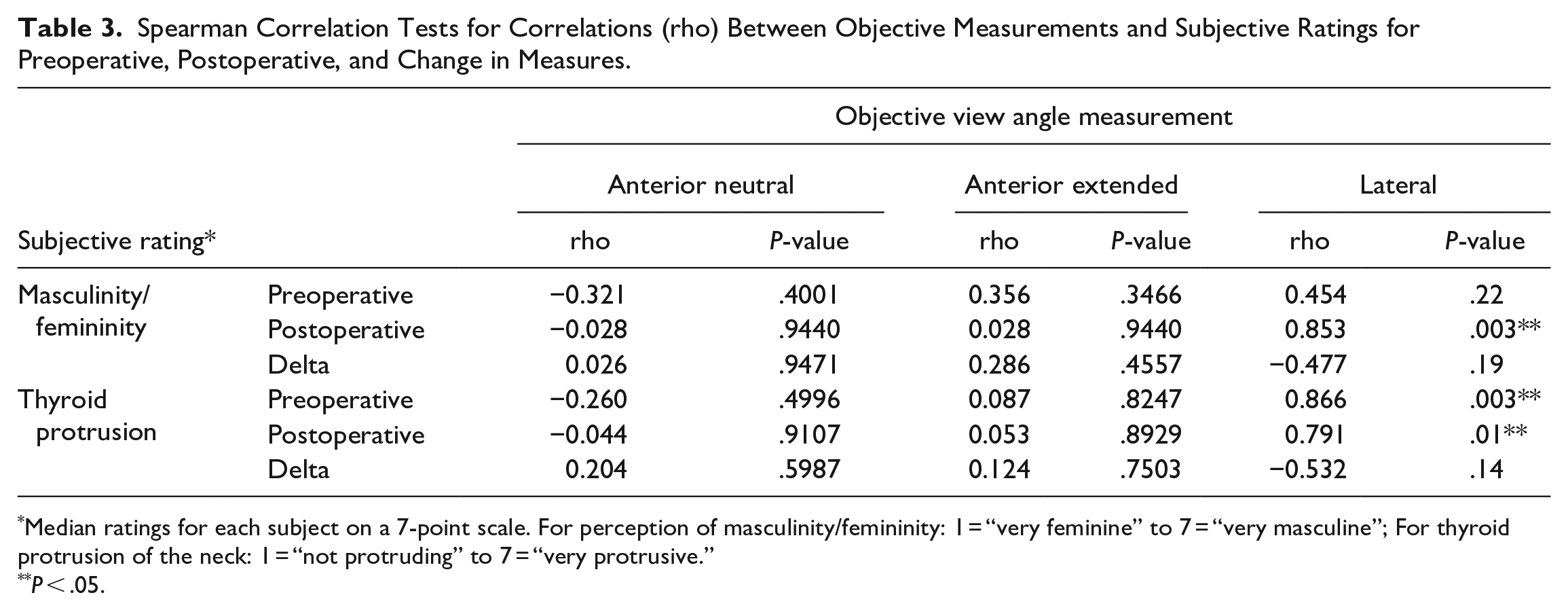
Median ratings for each subject on a 7-point scale. For perception of masculinity/femininity: 1 = “very feminine” to 7 = “very masculine”; For thyroid protrusion of the neck: 1 = “not protruding” to 7 = “very protrusive.”
P < .05.
Discussion
These data demonstrate anterior view “light reflex” and lateral view thyroid protrusion angles as well as 7-point rating scales of observer perceptions of neck femininity and thyroid protrusion are able to reflect changes in neck contour morphometry after endoscopic chondrolaryngoplasty. Specifically, thyroid protrusion by the objective “light reflex” and lateral view angles as well as subjective ratings of thyroid protrusion decreased, and subjective ratings of neck femininity increased after chondrolaryngoplasty as hypothesized. Good interrater reliability across all judges supports use of untrained observers as a viable measure in evaluating clinical outcomes of chondrolaryngoplasty. Furthermore, our results from subjective evaluation measures are consistent with those in Amir et al ’s study on perceptions of the neck after chondrolaryngoplasty. 13 When examining potential correlations between our tested objective and subjective measures, objective lateral view thyroid protrusion angle in postsurgical photographs was correlated with subjective ratings of neck femininity and thyroid protrusion by third-party observers. This suggests when the neck is analyzed in profile, the morphometric angle of the laryngeal prominence after chondrolaryngoplasty may be useful as a surrogate measure of public perception of the neck. These objective and subjective measures show promise as potential evaluation measures of chondrolaryngoplasty outcomes and should be considered for further investigation and development.
Perception of neck femininity is inherently complex and nuanced. One study investigating objective neck measurements demonstrated that cisgender male and female necks are not merely scaled versions of each other but rather are geometrically different, although laryngeal prominence was not specifically evaluated. 22 In studying physical attributes of the neck that contribute to gender perception, Amir et al found that the attributes of thyroid protrusion, neck girth, and skin-smoothness most significantly and independently contributed to subjective gender perception. 13 With an endoscopic approach to chondrolaryngoplasty, laryngeal prominence reduction takes center stage as the sole visual outcome without scar evidence of surgery. The objective and subjective methods of measurement tested in this pilot study may facilitate new opportunities for evaluating and researching chondrolaryngoplasty. For example, the “light reflex” and lateral thyroid protrusion angles may provide an objective metric usable by artificial intelligence programs to analyze large samples of photographs more efficiently, allowing higher statistical power studies on chondrolaryngoplasty. Future research may be directed to identify additional techniques for objectively and subjectively evaluating outcomes in patients undergoing surgical gender affirmation of the neck.
This study is limited using untrained judges rather than assessing patient satisfaction—a more commonly employed outcomes measure. Due to the small sample size of this pilot study, Spearman correlation testing likely had insufficient statistical power to detect smaller or moderate correlations as significant, and correlations between subjective and objective measures should continue to be explored. A larger cohort of both patients and untrained judges could quantify the impact of feminine gender perception of the neck by this scarless approach. Our study also relied on the use of physician judges who all identified as cisgender. A more diverse sample of randomly selected non-physician judges, including those from the LGBTQ community, may also better represent appropriate subjective assessment and thereby support the generalizability of this evaluation method as a dependable secondary outcomes instrument. And while the focus on outcomes for this surgery in transgender women in this study has advantages, future inclusion of cisgender individuals seeking reduction in thyroid protrusion may also reveal different patterns.
Conclusion
Morphometric “light reflex” and thyroid protrusion angles as well as subjective observer perceptions of gender-specific contour and thyroid protrusion may represent promising novel methods for evaluating outcomes after endoscopic chondrolaryngoplasty. Lateral thyroid protrusion angle after chondrolaryngoplasty may also be a good indicator for how observers will perceive neck femininity and thyroid protrusion.
Footnotes
Authors’ Note
Alden Smith is now affiliated to Department of Otolaryngology - Head & Neck Surgery, Stanford University, Palo Alto, CA, USA.
Abie H. Mendelsohn is now affiliated to Los Angeles Center for Ear, Nose, Throat and Allergy, Los Angeles, CA, USA
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.