
Abstract
Objectives:
The Intranasal Schirmer test (INS) is an easy to administer test that can yield objective measurement of the quantity of nasal secretion and has been studied in patients with various nasal and systemic pathologies; however, the role of INS in patients with allergic rhinitis remains unclear. Our aim was to determine the relationship between various allergic symptoms and the Intranasal Schirmer Test (INS) score and to evaluate the utility of INS in determining treatment effect in patients with allergic rhinitis.
Methods:
This prospective study included patients with allergic rhinitis who were randomly divided into 3 treatment groups (nasal steroid only, oral antihistamine only, nasal steroid and oral antihistamine). For all patients, Total Nasal Symptom Score (TNSS) was used to measure symptom severity and INS was administered before and after treatment. Pre-treatment and post treatment TNSS and INS scores were compared between different treatment groups and within each group.
Results:
The study included 120 patients, with 40 patients in each group. There were significant differences both in pre-treatment and post-treatment symptom severity score with changes of INS scores between treatment groups (P < .001 and P = .002, respectively). There was a significant difference between pre-treatment and post-treatment symptom severity scores and the INS score in each treatment group (P < .001). There was also a significant positive correlation between INS score and TNSS (r = .591 and P < .001).
Conclusion:
The Intranasal Schirmer Test can be used as an objective tool for patients with allergic rhinitis as an adjunct to subjective patient symptom reports and can also be used to determine the response to treatment.
Introduction
Allergic rhinitis is a common condition that affects individuals of all ages and negatively affects quality of life.1 -3 The disease is characterized by mucosal inflammation that triggers an inflammatory pathway, leading to vascular dilation, edema, and an increase in nasal secretion.4,5 Rhinorrhea, nasal itching, sneezing, and nasal congestion are the primary symptoms of allergic rhinitis.3,6 Various tests can be performed to obtain an objective diagnosis of allergic rhinitis; however, there is no easy to use objective test that measures nasal secretion (rhinorrhea).
The Schirmer test is routinely used by ophthalmologists for measuring the amount of lacrimal tear production, and diagnosing dry eye. 7 After the introduction of administering this test intranasally, it has been used to assess nasal cavity secretion and humidity in patients with various nasal and systemic pathologies.8 -10 The Intranasal Schirmer test (INS) is an easy to administer test that can yield objective measurement of the quantity of nasal secretion. 8 Other than ease of administration and acquisition of objective data, INS test is also cost effective, readily available and is well tolerated by patients. 8 INS has been studied in both the general population and in patients with various pathologies, including, but not limited to, such structural pathologies as nasal septal deviation and such systemic pathologies as Sjogren syndrome.8 -11 However, INS has not been studied previously in patients with allergic rhinitis. The primary objective of this study was to determine the utility of INS test in patients with allergic rhinitis and to evaluate the relationship between various allergic symptoms and the INS score. The secondary objective of this study was to evaluate the utility of INS in determining treatment effect in patients with allergic rhinitis and to compare the effect of different treatment modalities on allergic symptoms and the INS score in patients with allergic rhinitis.
Materials and Methods
This prospectively designed study was conducted after local ethical committee approval in our allergy clinic and included allergic rhinitis patients aged 18 to 50 years with positive skin tests for Dermatophagoides pteronyssinus and Dermatophagoides farinae. Patients were negative for other skin test allergens. These patients were diagnosed with allergic rhinitis based on their symptoms (rhinorrhea, nasal pruritus, sneezing and nasal congestion), their nasal examination and their positive skin test. Patients with nasal septal deviation, adenoid hypertrophy, and sinonasal pathologies (sinusitis, nasal polyposis ie,) were excluded. Patients with a history of sinonasal surgery, a history of treatment for allergic rhinitis, systemic diseases and comorbid conditions, use of systemic medications, and a history of smoking during the previous year were also excluded.
For evaluation of patient symptoms, Total Nasal Symptom Score (TNSS) was used to measure symptom severity. All patients were queried about the severity of their symptoms. Patients recorded their symptom severity ratings on a form that included 4 nasal signs of allergic rhinitis (rhinorrhea, nasal pruritus, sneezing, and nasal congestion). Each symptom was scored on a 4-point Likert-type scale, as follows: 0: no symptoms; 1: mild symptoms (symptoms clearly present, but with minimal awareness and easily tolerated); 2: moderate symptoms (awareness of bothersome, but tolerable symptoms); 3: severe symptoms (symptoms difficult to tolerate and/or causing interference with daily activities, sleep, or both).
Next, the INS was administered to all patients, as described by Lindemann et al 8 Briefly, Schirmer test paper strips (Schirmer test paper; Dr. Gerhard Mann Chem.- Pharm Fabrik GmBH, Berlin, Germany) marked at with 1 mm intervals from 1 to 35 mm were used to perform the INS. An angle of 45° was formed by folding the strips at 5 mm distance. The folded strips were placed on the mucosa of the anterior nasal septum bilaterally during anterior rhinoscopic examination. The paper strips were placed such that the 5 mm long part was completely in contact with the anterior septal mucosa and the remaining part of the strip extended out of the nostril. After 10 minutes, the wetted area was measured (mm). Testing was conducted at the same time of day and at the same location in all participants, so as to maintain standardized conditions. All tests were administered by the same physician. Before proceeding to any further treatment measures, all patients were informed about the test results and the main measures that need and can be taken to avoid house dust mites were discussed.
The patients were then randomly divided into 3 treatment groups. Block randomization method was used for randomization of patients. The physician that administered the INS was blinded to the group to which the patient was assigned. Group 1 was administered only nasal steroid (mometasone furoate), group 2 received oral antihistamine (levocetirizine dihydrochloride), and group 3 received both nasal steroid (mometasone furoate) and oral antihistamine (levocetirizine dihydrochloride). All the patients in each group received the same dose and duration of treatment. The dosage for mometasone furoate was 2 actuations (50 mcg/actuation) in each nostril twice a day (total dose 200 mcg) and the dosage for levocetirizine dihydrochloride was one 5 mg tablet once per day.
After 1 month of treatment all the patients came for a follow-up visit, at which time they were examined, and then completed the same TNSS they completed at the beginning of the study. Next, the INS was administered again, so as to note any post-treatment changes in INS values. The patients that did not comply with the treatment were excluded.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Windows v.22.0 (IBM Corp., Armonk, NY, USA). Power analysis was used to determine the sample size, where Alpha value and power were set to 0.05 and 0.8, respectively. The normality of the distribution of data was tested using the Kolmogorov-Simirnov test. Descriptive data are presented as mean ±SD and median. The chi square test was used to compare the gender distribution between the 3 treatment groups. As age, INS scores, and symptom severity scores before and treatment were not normally distributed, the Kruskal-Wallis test was conducted to compare these variables between treatment groups, and the Wilcoxon signed rank test was used to compare the change in each symptom severity score and INS score after treatment in each treatment group. Mann-Whitney test was used for subgroup analysis. While investigating the associations between the INS score and each symptom severity scores, the correlation coefficients and their significance were calculated using Spearman’s correlation test. The level of statistical significance was set at P < .05. Statistically significant differences are denoted in bold text in the tables.
Results
The study included 120 patients (68 female and 52 male). Groups 1, 2, and 3 each included 40 patients. Age and gender did not differ significantly between the groups (P > .05).
A-Symptom Scores (Each Symptom Individually and Total TNSS Score)
Pre-treatment
There were no significant differences in pre-treatment symptom severity scores for rhinorrhea, nasal pruritus, or sneezing (P = .059, P = .052, and P = .141, respectively; Kruskal-Wallis test). However, the pre-treatment nasal congestion severity score differed significantly between the treatment groups; it was significantly higher in group 2 than in groups 1 and 3 (P = .002; Kruskal-Wallis test). In total, there was a significant difference between the pre-treatment symptom scores; scores in group 2 were significantly higher than that in group 1 and group 3 (P = .005; Kruskal-Wallis test) (Table 1).
INS and Symptom Scores Before and After Treatment According to Group.
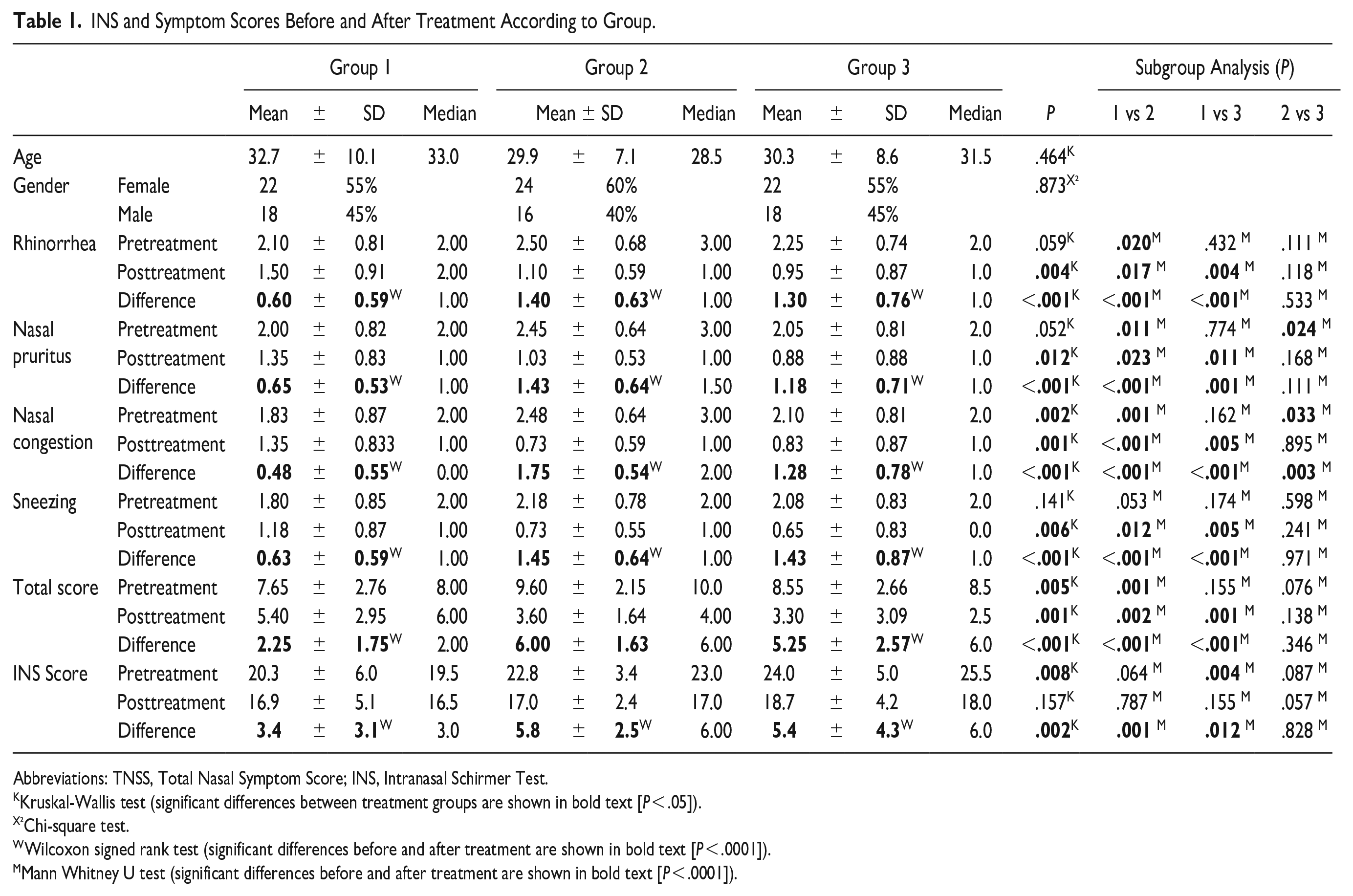
Abbreviations: TNSS, Total Nasal Symptom Score; INS, Intranasal Schirmer Test.
Kruskal-Wallis test (significant differences between treatment groups are shown in bold text [P < .05]).
Chi-square test.
Wilcoxon signed rank test (significant differences before and after treatment are shown in bold text [P < .0001]).
Mann Whitney U test (significant differences before and after treatment are shown in bold text [P < .0001]).
Post-treatment
All symptom severity scores (rhinorrhea, nasal pruritus, nasal congestion and sneezing) differed significantly between the 3 treatment groups (P = .004, P = .012, P = .001, and P = .006, respectively; Kruskal-Wallis test); scores in group 1 were significantly higher than in group 2 and group 3 (P = .001; Kruskal-Wallis test) (Table 1).
Pre-treatment—post-treatment difference
There were significant differences between all pre-treatment and post-treatment symptom severity scores in all treatment groups, pre-treatment—post-treatment score differences were significantly lower in group 1 (P < .001; Kruskal-Wallis test) (Table 1).
B-INS Scores
Pre-treatment
The pre-treatment INS score differed significantly between the 3 treatment groups; group 3 had a significantly higher score than groups 1 and 2 (P = .008; Kruskal-Wallis test) (Table 1).
Post-treatment
There were no significant differences in the post-treatment INS score between the 3 treatment groups (P = .157; Kruskal-Wallis test) (Table 1).
Pre-treatment—post-treatment difference
Pre-treatment and post-treatment INS scores differed significantly in all 3 treatment groups, İn group 1 the difference was significantly lower than in groups 2 and 3 (P = .002; Kruskal-Wallis test) (Table 1).
C-Comparison of Pre-treatment and Post-Treatment Study Values in Each Treatment Group
There was a significant difference between pre-treatment and post-treatment symptom severity scores and the INS score in each treatment group (P < .001; Wilcoxon signed rank test) (Table 1).
D-INS Score Correlations
There was a significant positive correlation between the INS score and pre-treatment and post-treatment change in all symptom severity scores (rhinorrhea, nasal pruritus, nasal congestion, and sneezing) (r = .631, r = .573, r = .357, and r = .382, respectively, P < .001 for all symptoms; Spearman’s correlation test). In total, there was a significant positive correlation between the INS score and total symptom severity score (r = .591 and P < .001; Spearman’s correlation test) (Table 2).
Correlations Between the INS Score and Symptom Severity Scores.
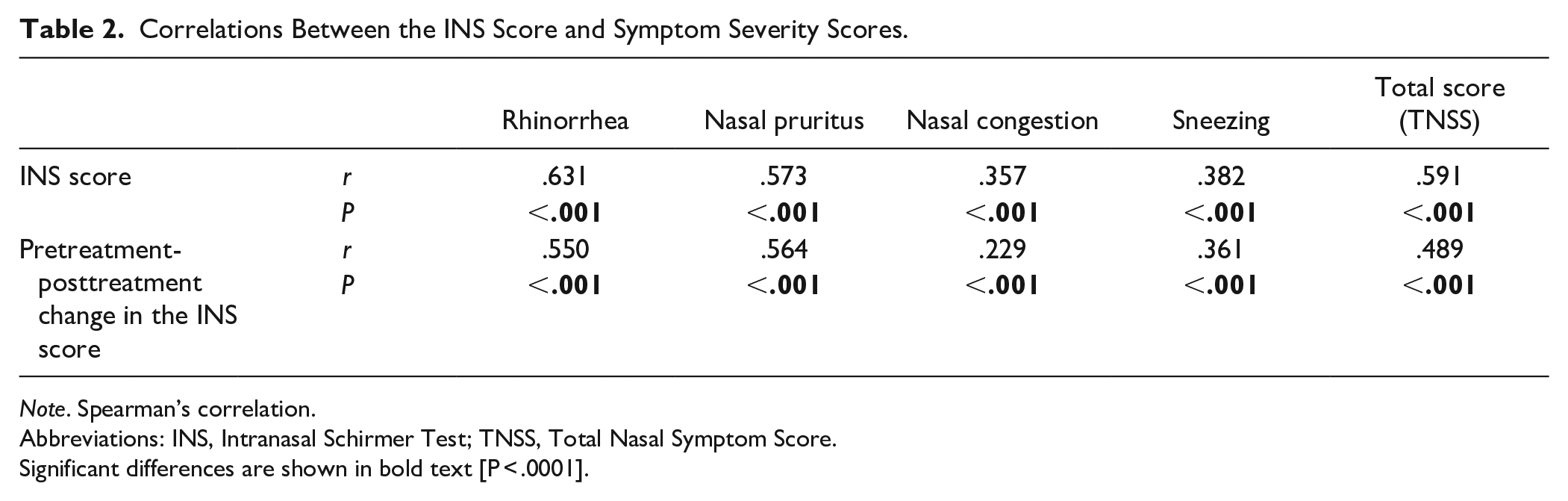
Note. Spearman’s correlation.
Abbreviations: INS, Intranasal Schirmer Test; TNSS, Total Nasal Symptom Score.
Significant differences are shown in bold text [P < .0001].
There was also a significant positive correlation between pre-treatment and post-treatment change in the INS score and pre-treatment and post-treatment change in each symptom severity score (rhinorrhea, nasal pruritus, nasal congestion, and sneezing) (r = .550. r = .564, r = .229, and r = .361, respectively, P < .001 for all symptoms; Spearman’s correlation test). In total, there was a significant positive correlation between pre-treatment and post-treatment change in the INS score and pre-treatment and post-treatment change in the overall symptom severity score (r = .489 and P < .001; Spearman’s correlation test) (Table 2).
Discussion
The present findings show that INS scores were correlated with symptom severity score. Besides, we showed that INS score significantly decreases with the treatment of allergic rhinitis, and that this decrease is significantly correlated with the decrease in allergic symptom severity, regardless of treatment modality. Furthermore, current data suggests that the effect of the treatment of allergic rhinitis can be observed objectively using the INS score and supported by subjective symptom severity scores. These findings show the consistency of the INS score and symptom severity scores.
The INS primarily measures the quantity of nasal secretion. 8 In the present study the INS was used to objectively measure nasal secretion and to support those findings with subjectively measured symptom severity scores. The present findings show that the symptom that corresponds most with increased nasal secretion based on the INS score is rhinorrhea. All the patients had a significant decrease is rhinorrhea that was significantly correlated with the INS score. The other symptoms of allergic rhinitis studied (nasal itching, sneezing and nasal congestion) were also significantly correlated with the INS score.
Intranasal corticosteroids and oral antihistamines can be used alone or in combination for the treatment of allergic rhinitis.1,2,12 All 3 of the present study’s treatment groups exhibited significant improvement after treatment; however; group 1 (intranasal steroids alone) had the least benefit from treatment, which is in contrast to some studies that recommend intranasal corticosteroids over oral antihistamines.13 -15 In group 1 the pre-treatment to post-treatment decrease in the INS score and symptom severity scores was less than in groups 2 and 3, and the difference was significant. In the present study the 3 treatment groups were randomly created, so as to avoid any patient treatment bias. However, Group 1 had the lowest pre-treatment total symptom severity score and the lowest pre-treatment INS score, which could have an effect on the results of the current study. Other than that, the adherence of the patient to a given treatment might be affected by several factors, including but not limited to the number of doses per day and the route of application. The nasal steroids are used twice a day instead of once a day like oral antihistamines, which might affect compliance of the patient. Besides, intranasal use of a medication might be harder for a patient compared to oral medication, also affecting the compliance. Besides, some studies suggest that patient treatment preference is affected by sensory characteristics and that patients tend to choose fluticasone furoate over mometasone furoate— the nasal steroid used in the present study.16,17 Mometasone furoate significantly improves nasal symptoms and quality of life,18,19 but due to its associated bitter taste and nasal irritation some of the present study’s patients might not have been able to use it as necessary secondary to this irritation. All these factors might have an impact on patient compliance with nasal steroids, with the patient skipping some doses unintentionally or using the medication improperly. These patients might still report full compliance but less benefit from the treatment, and we have no objective tools to measure compliance other than patient’s self-report of adherence to treatment. All these findings might also explain why the improvement was lower in Group 1.
In previous studies that INS was evaluated on normal healthy population, it has been reported that INS values for healthy mucosa ranged from 6 to 18 mm. 8 Our results show higher pre-treatment INS values when compared to previous studies with healthy volunteers,8,11 which suggests that INS values increase in patients with allergic rhinitis and that this increase can be measured objectively based on the INS score. In addition, INS scores decreased after treatment in the present study. The present study is the first study to evaluate the INS score in patients with allergic rhinitis and post treatment change in the INS score. The strengths of this study include its prospective design and treatment randomization. Besides, a validated measure of rhinitis symptoms (TNSS) was used. The study included a large study population, and the objective INS score was significantly correlated with the subjective symptom severity scores. Each INS was performed by the same physician that was blinded to the treatment groups, further strengthening the study. INS measures nasal secretion which is related clinically mainly to rhinorrhea, but we also questioned other symptoms of allergy like nasal congestion, sneezing and pruritus. Allergic rhinitis symptoms can be variable, and the patient’s primary complaint might be nasal congestion. Application of INS for these patients might reveal an underlying increased nasal secretion and possibly allergic origin. The addition of these symptoms to the study support the relationship between INS scores and several symptoms of allergic rhinitis, which is important and increases the strength of the study. The study by Lindemann et al showed that smoking significantly decreases the INS values, thus we excluded the patients who smoke to avoid any bias. 8 Lastly, patients with additional nasal and systemic diseases were excluded as these pathologies could have an impact on the INS values.8 -10 All these exclusion criteria also increase the strength of the study.
The follow-up of allergic rhinitis patients is generally based on the use of patients’ subjective reports of symptoms for evaluating treatment effectiveness. The INS can be used as an objective adjunct to these patient subjective reports, which can help physicians and patients to objectively measure symptom improvement, and compare the effects of different medications. The patients will understand their symptoms are appreciated, objectively measured and possibly recorded. This leads to an increase of patient compliance. The clinicians on the other hand, will be more comfortable about having an objective measure, rather than relying only on subjective symptoms. The patients’ symptoms may not always be compatible with the nasal examination; the patient might be symptomatic but the nasal examination may have returned back to normal (or vice versa). Such cases might require a change in medication and a follow up. This might lead to a prolonged follow up time and medication. INS would help in these circumstances, both from the patients and the clinician’s perspective as an objective adjunct to nasal examination and patient symptoms.
INS test gives an objective data which is one of the most important features of a clinically applied test, and this is important for patients with allergic rhinitis. However, several additional features of the test also make it favorable for clinical use. First of all, the test can be easily administered and thus can easily be performed by physicians. As it is easily applied, it does not require a troublesome learning curve. Other than that, the patients tolerate the test pretty well and none of our patients reported any discomfort. This increases the patient compliance and clinical usability of the test. On top of all these, the test is easily accessible and inexpensive, making the test cost effective and readily available. All these factors contribute to wide clinical use of this test, which can help patients and physicians have a more objective discussion about the symptoms and findings of the patients and come up with a more personalized treatment plan.
Conclusion
The INS is an easy to use objective test for evaluating nasal secretion and can be used for patients with allergic rhinitis. The INS score decreases significantly following the treatment of allergic rhinitis, which correlates significantly with patient reported decreases in symptom severity. The present findings show that the INS can be used as an objective tool for patients with allergic rhinitis as an adjunct to subjective patient symptom reports and can also be used to determine the response to treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.