
Abstract
Background:
Many people with cystic fibrosis (PwCF) have chronic rhinosinusitis (CRS). CRS requires additional management beyond that of pulmonary disease and leads to increased utilization of healthcare resources. Elexacaftor/tezacaftor/ivacaftor (ETI) is a highly effective modulator therapy that has been shown to improve CRS in PwCF. However, the impact of ETI on rhinologic healthcare utilization is understudied.
Objective:
To compare rates of rhinologic healthcare utilization and procedures among PwCF prior to and after initiating ETI therapy.
Methods:
A single-center, cohort study investigating adult PwCF was performed in January 2023. Demographics, clinical characteristics, and data related to CF treatment were retrospectively abstracted. Characteristics of the cohort were compared over 2 periods: the 12-months prior to ETI initiation and the 12-months after ETI initiation. Post-ETI data were linearly extrapolated if a subject had not yet completed the full 12 months of ETI. Paired t-testing, Wilcoxon signed rank testing, and regression analysis were performed.
Results:
Of 126 PwCF, 98 (77.8%) were on ETI therapy and 35 (27.7%) were both on ETI and concurrently followed by the rhinology service (ETI-ENT). Rhinology clinic visits (P = .007) and frequency of obtaining nasal cultures (P = .046) decreased for the ETI-ENT cohort after initiating ETI treatment. There were no significant changes in the number of endoscopic sinus surgeries (P = .452) performed. Beyond ETI use, regression analysis did not identify any factors associated with changes in utilization.
Conclusion:
Aspects of rhinology healthcare utilization by PwCF decreased after initiation of ETI therapy. Additional studies are needed to determine rhinologic healthcare requirements for PwCF who remain on ETI for the long-term and to evaluate larger cohorts of PwCF on ETI.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a common complication of cystic fibrosis (CF) that can increase the frequency of pulmonary exacerbations and worsen health-related quality of life (QOL).1,2 Many people with CF (PwCF) require dedicated management of their sinonasal disease with the assistance of a rhinologist. 1 Rhinologic management of CRS typically consists of topical saline irrigations, steroids, and antibiotics—endoscopic sinus surgery (ESS) is recommended for patients who fail medical treatments. ESS is effective at reducing symptom burden and improving sinonasal QOL. ESS and nearly all interventions carry a cost as well as time burden for PwCF.
The expansion of highly effective modulator therapy including elexacaftor-tezacaftor-ivacaftor (ETI) modulator therapy has reshaped CF management. Besides improving pulmonary function and reducing the frequency of pulmonary exacerbations, ETI has been shown to reduce CRS symptoms and objective disease severity on sinus CT and nasal endoscopy.3 -6 However, the impact of ETI on rhinologic healthcare utilization is understudied. Therefore, the aim of this investigation was to compare rates of rhinologic healthcare utilization and procedures among PwCF prior to and after initiating ETI therapy.
Methods
This study is a single-center, retrospective cohort evaluation of PwCF seen by the Adult CF Clinic at the University of California, Los Angeles from October 2018 to January 2023. Institutional Review Board approval was obtained (IRB #22-001047), and the requirement for informed consent was waived. Inclusion criteria included age≥18 years with a diagnosis of CF based on sweat chloride or genetic testing and currently followed by a UCLA rhinologist. Demographics (age, gender, race/ethnicity, comorbidities), disease characteristics, data related to CF treatment, and data related to rhinology clinic visits and rhinology-specific care were retrospectively abstracted from the medical record. Outcome measures included number of rhinology clinic visits, percent-predicted FEV1 (ppFEV1), and number of nasal cultures, sinus debridements, and ESS procedures performed.
Participants were separated into 2 cohorts: PwCF concurrently followed by a UCLA rhinologist and receiving ETI therapy (ETI-ENT), and PwCF followed by a UCLA rhinologist but not receiving ETI therapy (Non-ETI). Characteristics of the ETI-ENT cohort were compared over 2 periods: the 12-months prior to ETI initiation (pre-ETI) and the 12-months after ETI initiation (post-ETI). Post-ETI data were linearly extrapolated if a subject had not yet completed the full 12 months of ETI. Characteristics of the Non-ETI cohort were compared between the 12-months prior to the initiation of the California COVID-19 lockdown on March 19, 2020 (pre-Lock) and the 12-months after issuance of the stay-at-home order (post-Lock). Statistical comparisons were completed using STATA software (version 17.0; StataCorp, College Station, TX). Power analysis indicated that assuming a 2-sided alpha level of 0.05, a sample size of 35 was able to achieve 80% power for minimally detecting a standardized effect size (Cohen’s d) of 0.5 (G*Power, version 3.1). Data were evaluated for normality using Shapiro-Wilks testing. Bivariate comparisons between the ETI-ENT and Non-ETI cohorts were computed using either 2-tailed independent sample t-testing or Mann–Whitney U testing, and chi-square testing for categorical variable comparisons. Matched samples comparisons were performed using 2-tailed paired t-testing and Wilcoxon signed-rank testing (statistical significance: P < .05).
Results
Forty eight PwCF were included in this study, 35 were in the ETI-ENT cohort and 13 were in the Non-ETI cohort. Demographics, disease characteristics, treatment history, and modulator use are reported in Table 1. The mean age was 36.9 [±15.1] years, and 56.3% of patients were female. Over two-thirds had documented nasal polyposis or a history of prior ESS. Most patients (79.2%) had at least one copy of the F508del variant, 35 (72.9%) were on current ETI therapy, and 2 (4.1) were on ivacaftor. Dates of ETI initiation ranged from October 2019 to September 2022. Bivariate comparisons revealed that presence of a F508del mutation was more common in the ETI-ENT cohort (Table 2).
Enrollment Demographics and Clinical Characteristics.
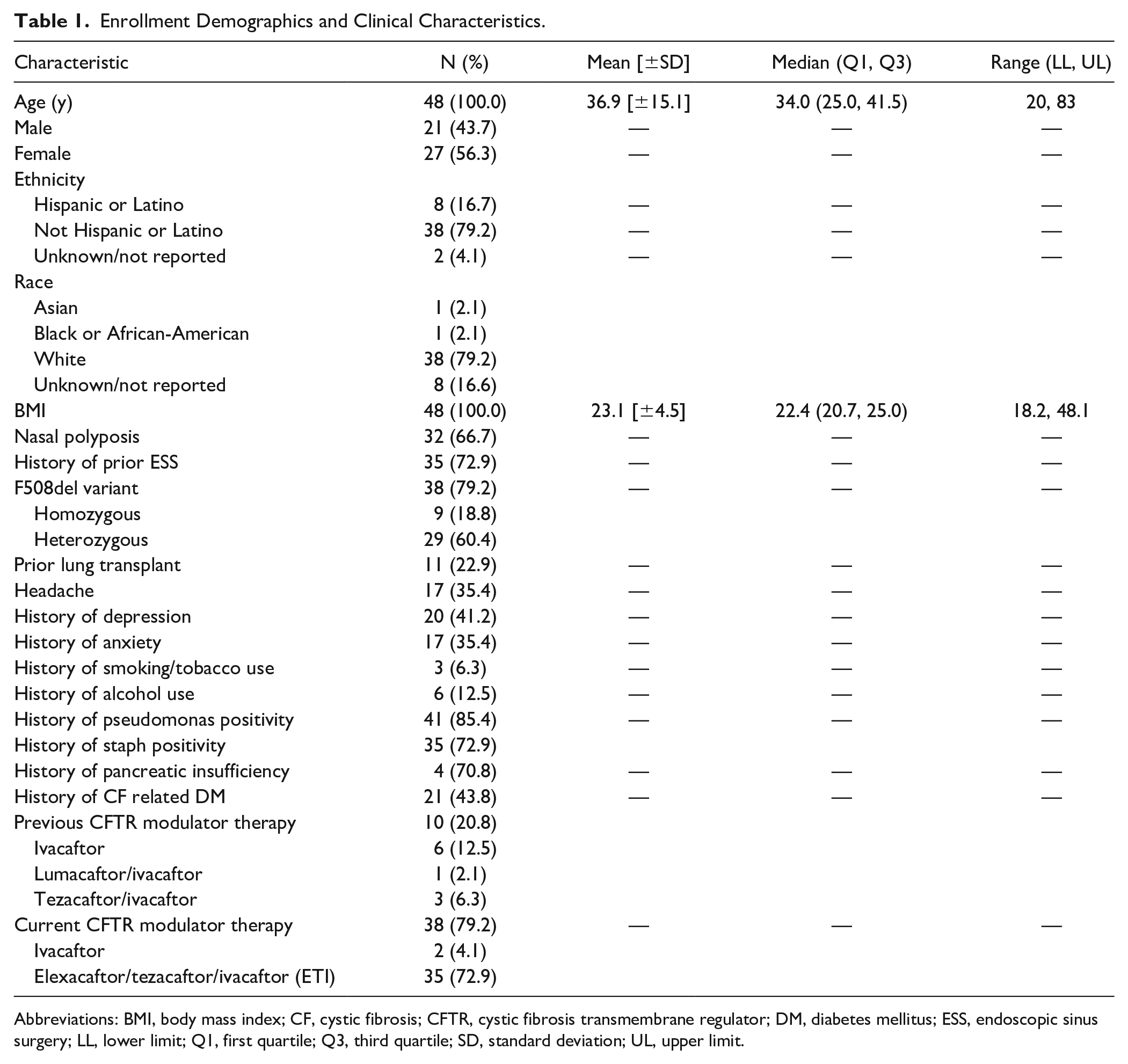
Abbreviations: BMI, body mass index; CF, cystic fibrosis; CFTR, cystic fibrosis transmembrane regulator; DM, diabetes mellitus; ESS, endoscopic sinus surgery; LL, lower limit; Q1, first quartile; Q3, third quartile; SD, standard deviation; UL, upper limit.
Bivariate Comparisons of Demographics and Clinical Characteristics Between ETI-ENT and Non-ETI Cohorts.
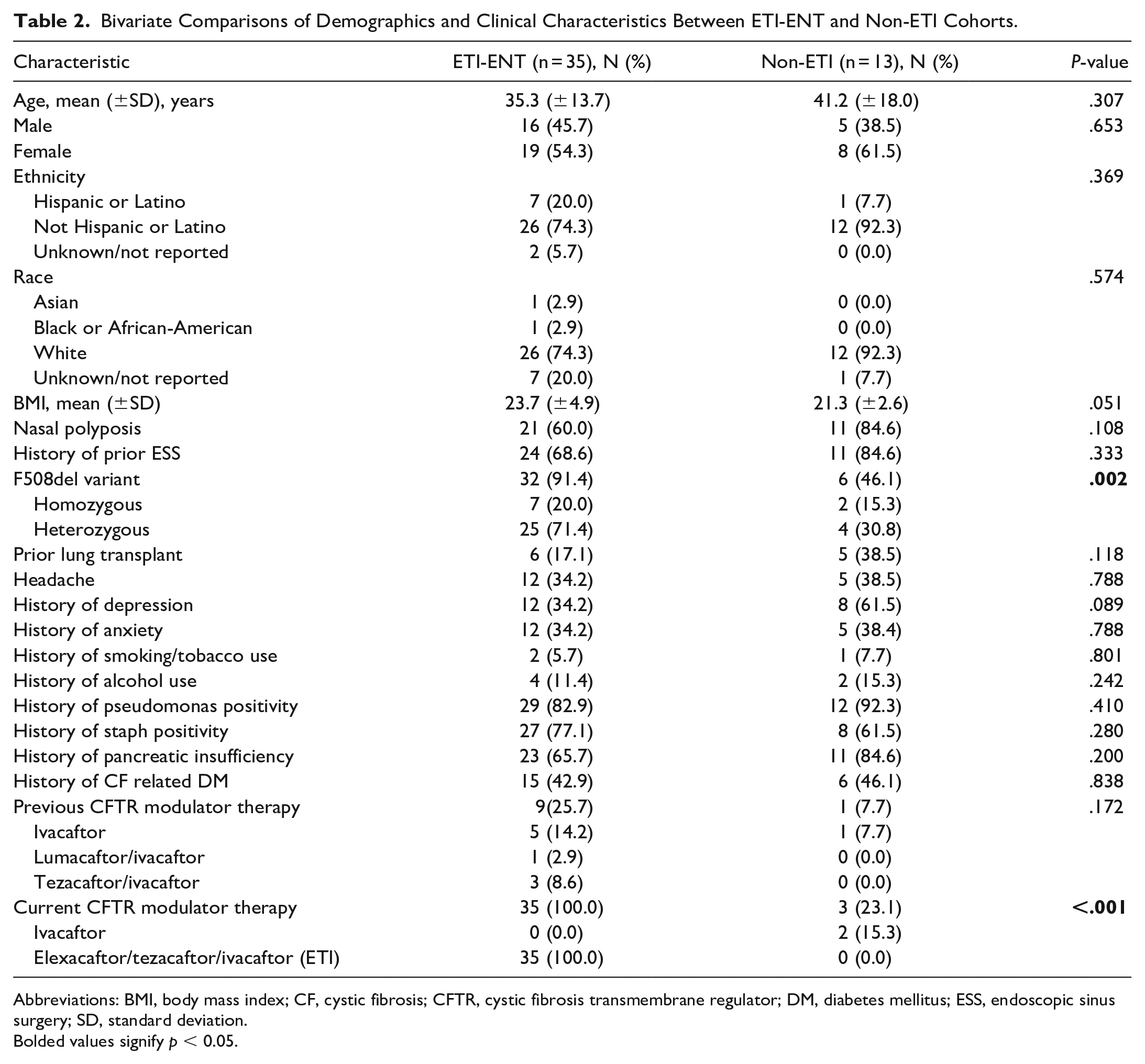
Abbreviations: BMI, body mass index; CF, cystic fibrosis; CFTR, cystic fibrosis transmembrane regulator; DM, diabetes mellitus; ESS, endoscopic sinus surgery; SD, standard deviation.
Bolded values signify p < 0.05.
Rhinologic healthcare utilization, pulmonary function, and sinonasal symptom burden were compared between the pre-ETI and post-ETI periods in the ETI-ENT cohort and, separately, between the pre-Lock and post-Lock periods in the Non-ETI cohort (Table 3). Rhinology clinic visits significantly decreased in the post-ETI period (P = .007) for ETI-ENT. Although there were no significant changes in the number of ESS procedures performed, PwCF on ETI underwent fewer sinus debridements (P = .031) and nasal cultures (P = .046) post-ETI. ppFEV1 also increased after ETI therapy, indicating improved lung function (P = .007). There were no significant changes in rhinology clinic visits, nasal cultures, sinus debridements, or ppFEV1 in the Non-ETI cohort between the pre-Lock and post-Lock periods.
Care Utilization by ETI-ENT 12 months Pre/post-ETI Initiation Versus Non-ETI 12 months Pre/post-lockdown.
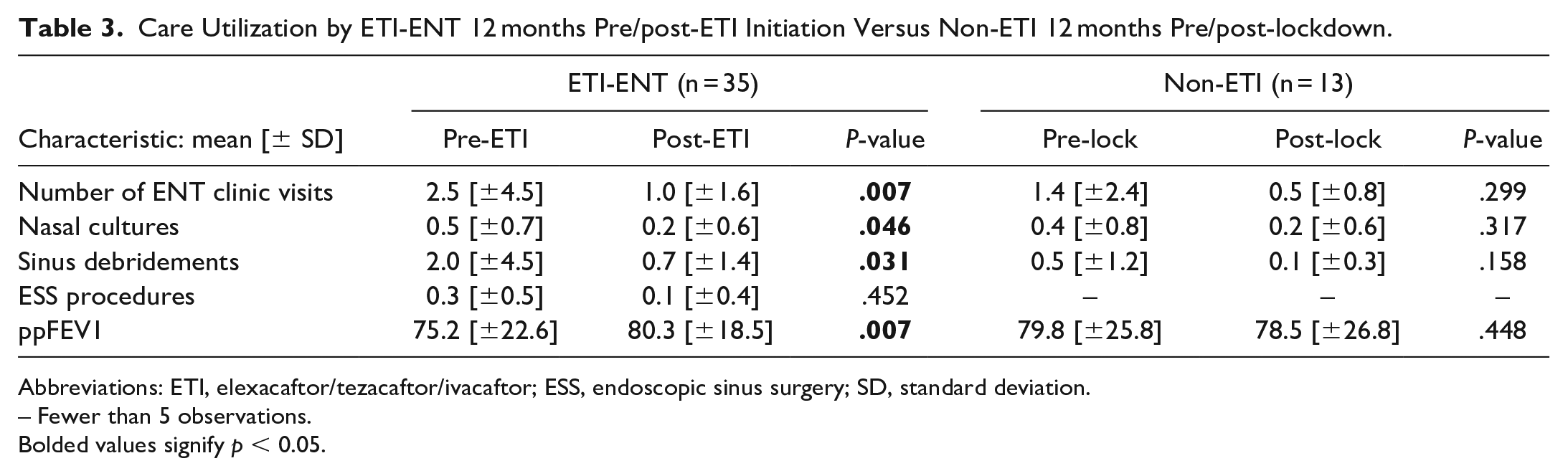
Abbreviations: ETI, elexacaftor/tezacaftor/ivacaftor; ESS, endoscopic sinus surgery; SD, standard deviation.
– Fewer than 5 observations.
Bolded values signify p < 0.05.
Discussion
Elexacaftor-tezacaftor-ivacaftor therapy has revolutionized the management of CF and is expected to further extend lifespans in the coming years. 7 Beyond improvements in pulmonary status, ETI also improves sinonasal QOL and reduces CRS severity on imaging and endoscopy.3,4 To our knowledge, this study is the first to demonstrate that ETI therapy is associated with reductions in rhinology healthcare utilization in PwCF, including rhinology clinic visits, sinus debridements, and nasal cultures. Consistent with prior work, our findings also demonstrated improvement in pulmonary function after ETI initiation, with the more modest improvements in this domain likely related to the higher baseline ppFEV1 than the cohorts included in prior clinical trials. 5
PwCF experience high treatment burden, and the time and psychological stressors associated with disease management often interfere with family and professional goals. A recent quantitative and thematic analysis of survey responses from PwCF and carers of PwCF identified number of treatments, time lost due to care coordination, and psychosocial aspects of treatment as major contributors to treatment burden. 8 Thus, minimizing treatment burden has become an emerging focus in CF research, especially in the era of highly effective modulator therapy. 9 Future prospective research should examine whether decreased need for health care utilization is specifically associated with improvements in quality of life, as is being pursued for CF-CRS. 10
Findings from this study should be evaluated in the context of potential limitations. Approximately half of the ETI-ENT cohort (18/35) initiated ETI prior to March 2020, and post-ETI follow-up may have been impacted by COVID-19 isolation policies. We attempted to control for the effects of pandemic isolation policies by comparing care utilization between the ETI-ENT and Non-ETI cohorts, the latter of which did not experience significant changes in rhinology care utilization after initiation of pandemic lockdown policies in California. We also attempted to incorporate changes in medication usage (corticosteroid sinus rinses, oral corticosteroids, oral antibiotics) and utilize other outcome measures, such as nasal endoscopy scores and sinus CT scans, however these data were not reliably available, related to the retrospective nature of our study and the pandemic. A 12-month period of data collection pre/post ETI initiation may also have been insufficient to capture changes in relatively infrequent events such as ESS; a numerical but not statistically significant change was seen for this measure. Finally, while selection bias may arise if patients on ETI therapy are not referred to rhinologists as frequently, most of the ETI-ENT cohort had already established care with a rhinologist due to the relatively recent introduction of ETI. We were unable to assess rhinology care utilization of PwCF who do not seek rhinology care from our institution.
Overall, our findings of reduced rhinologic healthcare utilization suggest that highly effective modulator therapies alleviate healthcare burden in CF-CRS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.M.B.: In the last 24 months, D.M.B. has received grant support unrelated to this work from the CF Foundation and International Society of Inflammation and Allergy of the Nose consultant for Garner Health (equity); received honorarium from Rockpointe.
J. L.T-C.: In the last 36 months, J.L.T-C. has received grants to her institution unrelated to this work from Vertex Pharmaceuticals Incorporated, Eloxx, and 4DMT; has received fees from Vertex Pharmaceuticals Incorporated related to consultation on clinical research design, participation on advisory boards, and speaking engagements; and has served on advisory boards and/or provided clinical trial design consultation for Insmed, 4DMT, and AbbVie. She serves on a DMC for AbbVie. She serves as the adult patient care representative to the CFF Board of Trustees, and on the CF Foundation’s Clinical Research Executive Committee, Clinical Research Advisory Board, Racial Justice Working Group and as immediate past chair of the CF TDN’s Sexual Health, Reproduction and Gender Research Working Group, on the scientific advisory board for Emily’s Entourage, and on the ATS Respiratory Health Awards, Scientific Grant Review and Clinical Problems Assembly Programming Committees.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.