
Abstract
Objectives:
To investigate the role of normal weight central obesity (NWCO) in the prognosis of sudden sensorineural hearing loss (SSNHL).
Methods:
We retrospectively investigated 807 cases of SSNHL from January of 2008 to August of 2019 from the Department of Otorhinolaryngology at Kaohsiung Medical University Hospital in southern Taiwan. We analyzed the association between overweight and obesity, NWCO, and the prognosis of SSNHL. The demographic and clinical characteristics, audiometry results, and outcomes were also reviewed.
Results:
The nonobese (body mass index [BMI] < 24 kg/m2) and overweight and obese groups (BMI ≥ 24 kg/m2) comprised 343 (42.50%) and 464 (57.50%) patients, respectively. The favorable prognosis rates in the nonobese and the overweight and obese groups were 45.48% and 45.91%, respectively, without a significant difference (P = .9048). Multivariate logistic regression revealed that BMI (adjusted odds ratio [aOR] = 1.00, 95% CI = 0.948-1.062, P = .9165) was not significantly associated with SSNHL recovery. The normal weight noncentral obesity (NWNCO) and NWCO groups comprised 266 (77.55%) and 77 (22.45%) patients, respectively, and had favorable prognosis rates of 48.50% and 35.06%, respectively. The difference between the groups was significant (P = .0371). Multivariate logistic regression analysis revealed that NWCO (aOR = 2.51, 95% CI = 1.292-5.019, P = .0075) was significantly associated with SSNHL recovery.
Conclusions:
NWCO may significantly affect the prognosis of SSNHL.
Keywords
Introduction
Hearing loss and obesity are growing global public health concerns that place a considerable economic burden on society and psychological burden on patients. The World Health Organization (WHO) has estimated that 466 million people (6.1% of the global population) are living with disabling hearing loss worldwide, 1 with sudden sensorineural hearing loss (SSNHL) affecting 5 to 20 per 100 000 people annually, although this number may be underestimated due to individuals who experience mild SSNHL or a quick, spontaneous resolution of SSNHL often not seeking medical care. 2 Numerous hypotheses regarding the pathophysiology of SSNHL have been proposed, with microvascular circulation compromise being one of the most widely accepted theories. 3 This would suggest the biological plausibility of an association between SSNHL and vascular risk factors. In addition, obesity, which is an independent risk factor for age-related hearing loss, has been proposed as a predisposing factor for SSNHL through cochlear microvascular circulation mechanisms, lipotoxicity, and related oxidative stress.4-8 A relatively high body mass index (BMI), which is a measure of overall obesity, and a relatively large waist circumference (WC), which is a measure of central adiposity, have been verified as being associated with a relatively poor hearing threshold in human studies.1,8-12
Few studies, however, have assessed the associations between the prognosis of SSNHL and obesity. 13 Moreover, most studies that have done so have used the WHO cutoff point for western subjects without consideration of ethnic or cultural factors. Furthermore, adipose tissue distribution has become increasingly recognized as an independent risk factor for cardiometabolic disease. 14 Therefore, we sought to investigate the combined effect of BMI and WC using the criteria of our own population on the outcomes of adults with SSNHL through a retrospective cohort study in which patients’ medical charts were reviewed in detail.
Materials and Methods
SSNHL cases from January of 2008 to August of 2019 were retrospectively collected from Kaohsiung Medical University Hospital, and information on the patients’ demographic characteristics was collected. Included patients with SSNHL had received audiometric testing, including pure tone audiometry, auditory brainstem-evoked responses, and magnetic resonance imaging, to exclude the possibility of acoustic neuroma. All recruited patients were treated according to a standard protocol, and we recorded each patient’s age, sex, BMI, WC, presenting symptoms, duration from onset to treatment, and medical history, including the patients’ history of coronary artery disease (CAD), hypertension (HTN), diabetes (DM), and lipid profile.
We assessed all included patients’ overall obesity using BMIs and their central obesity using WCs. Overweight and obese were defined as BMI ≥ 24 kg/m2 and nonobese was defined as BMI < 24 kg/m2 in accordance with the cutoff of the Ministry of Health and Welfare of Taiwan. The WHO definitions for overweight and obese were not adopted in this study because they are primarily based on criteria derived from studies of European populations; research has suggested that the cutoff point for such populations may be too high for Asian subjects and may, therefore, lead to underestimation of associated health risks.15-17 WC was measured at the narrowest point between the lower costal border and the iliac crest at the end of a normal exhalation, with the arms relaxed at the widest circumference of the buttocks, and central obesity (CO) was defined in accordance with the values specified by the Ministry of Health and Welfare in Taiwan as WC ≥ 90 cm in men and ≥80 cm in women. 18 Normal weight central obesity (NWCO) was defined as central obesity (according to WC) in participants with normal weight (according to BMI).19,20 Normal weight noncentral obesity (NWNCO) was defined as noncentral obesity and BMI in the normal range.
All included patients had received oral prednisolone (1 mg/kg per day, maximum of 60 mg, gradually tapered within 14 days). Exclusion criteria were an age younger than 20 years, external or middle ear disease, conductive hearing loss, acoustic trauma, brain tumor or vestibular schwannoma, fluctuating hearing loss, such as in Meniere’s disease, having received initial treatment later than 14 days, and cases with incomplete data or that were incompletely recorded. All patients were followed up at least 3 months after initial treatment in the outpatient department. We averaged the thresholds at 250, 500, 1000, 2000, and 4000 Hz to obtain the average pure tone audiometry threshold for each subject. Hearing improvement was evaluated by comparing the patient’s last follow-up audiogram with the audiogram obtained when SSNHL was diagnosed. The prognosis of SSNHL followed the criteria Committee of the Ministry of Health and Welfare in Japan, 2 which classes as complete recovery, marked recovery, slightly recovery, or nonrecovery. We further categorized the given grades of “complete recovery” and “marked recovery” to favorable prognosis, whereas patients with “slightly recovery” and “nonrecovery” were considered to poor prognosis.
Ethical Concerns
The study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-E(II)-20200379).
Statistical Analysis
Continuous variables were presented as means ± standard deviation, and categorical data were expressed as frequencies. Continuous variables were compared using Student’s t test, and categorical variables were compared using the chi-squared test. Multivariate logistic regression analysis was used to calculate the adjusted odds ratios (aORs) and 95% confidence interval (95% CI) of the SSNHL outcome factors. JMP 9.0 and Stat View 5.0 (SAS Institute, Cary, NC, USA) were used for statistical analyses. All statistical tests were two-sided, and P < .05 was considered statistically significant.
Results
Demographic Findings
This study included 422 (52.29%) male patients and 385 (47.71%) female patients. The mean age of all 807 patients was 52.49 ± 14.63 years, and the mean BMI was 24.89 ± 4.16 kg/m2. The mean WC was 86.49 ± 13.49 cm. The general characteristics of all subjects (N = 807) and the cases categorized by BMI are listed in Table 1. The nonobese group (BMI < 24 kg/m2) included 343 (42.50%) patients, and the overweight and obese group (BMI ≥ 24 kg/m2) included 464 (57.50%). The rates of favorable and poor prognoses were 45.48% and 54.52%, respectively, in the nonobese group, and 45.91% and 54.09%, respectively, in the overweight and obese group. No significant differences in prognosis were identified in the nonobese and overweight and obese groups (P = .9048). Significantly more male than female patients belonged to the overweight and obese group (P = .0285). More patients experienced symptoms of vertigo in the nonobese group than in the overweight and obese group (P = .0278). Significantly more patients had a history of DM and HTN in the overweight and obese group than in the nonobese group (P < .0001). The overweight and obese group had higher levels of triglycerides, total cholesterol, and low-density lipoprotein cholesterol than the nonobese group did. The overweight and obese group had lower levels of high-density lipoprotein cholesterol than the nonobese group did. Age, smoking habits, duration from onset to treatment, initial hearing loss, symptoms of tinnitus, history of CAD, and prognosis did not significantly differ between groups (Table 1).
General Characteristics of Total SSNHL Cases and Cases Categorized into Nonobese and Obese/overweight Groups According to BMI and the Criteria of the Taiwanese Ministry of Health and Welfare; N = 807.
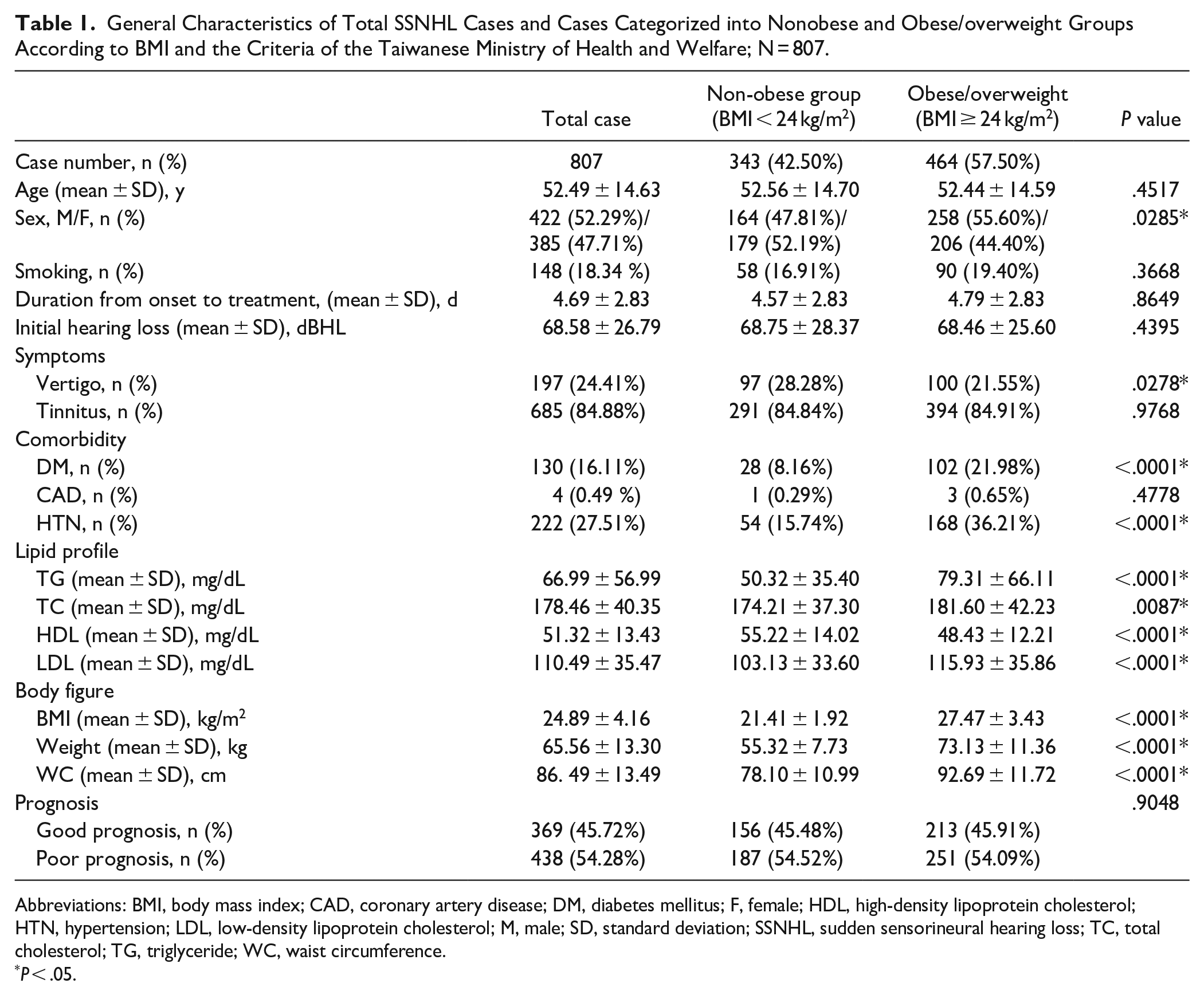
Abbreviations: BMI, body mass index; CAD, coronary artery disease; DM, diabetes mellitus; F, female; HDL, high-density lipoprotein cholesterol; HTN, hypertension; LDL, low-density lipoprotein cholesterol; M, male; SD, standard deviation; SSNHL, sudden sensorineural hearing loss; TC, total cholesterol; TG, triglyceride; WC, waist circumference.
P < .05.
The results of multivariate logistic regression analysis to evaluate the associations between all considered variables and prognosis (favorable vs poor) of SSNHL for all subjects (N = 807) are presented in Table 2. Only duration from onset to treatment (adjusted OR = 1.08, 95% confidence interval [CI] = 1.032-1.147, P = .0018) and vertigo (adjusted OR = 1.81, 95% CI = 1.288-2.570, P = 0.0007) were significantly associated with the prognosis of SSNHL; being overweight or obese (adjusted OR = 0.80, 95% CI = 0.522-1.277, P = .3087) and the other variables were not.
Multivariate Logistic Regression Analysis for Prognosis of All Patients With SSNHL (N = 807).
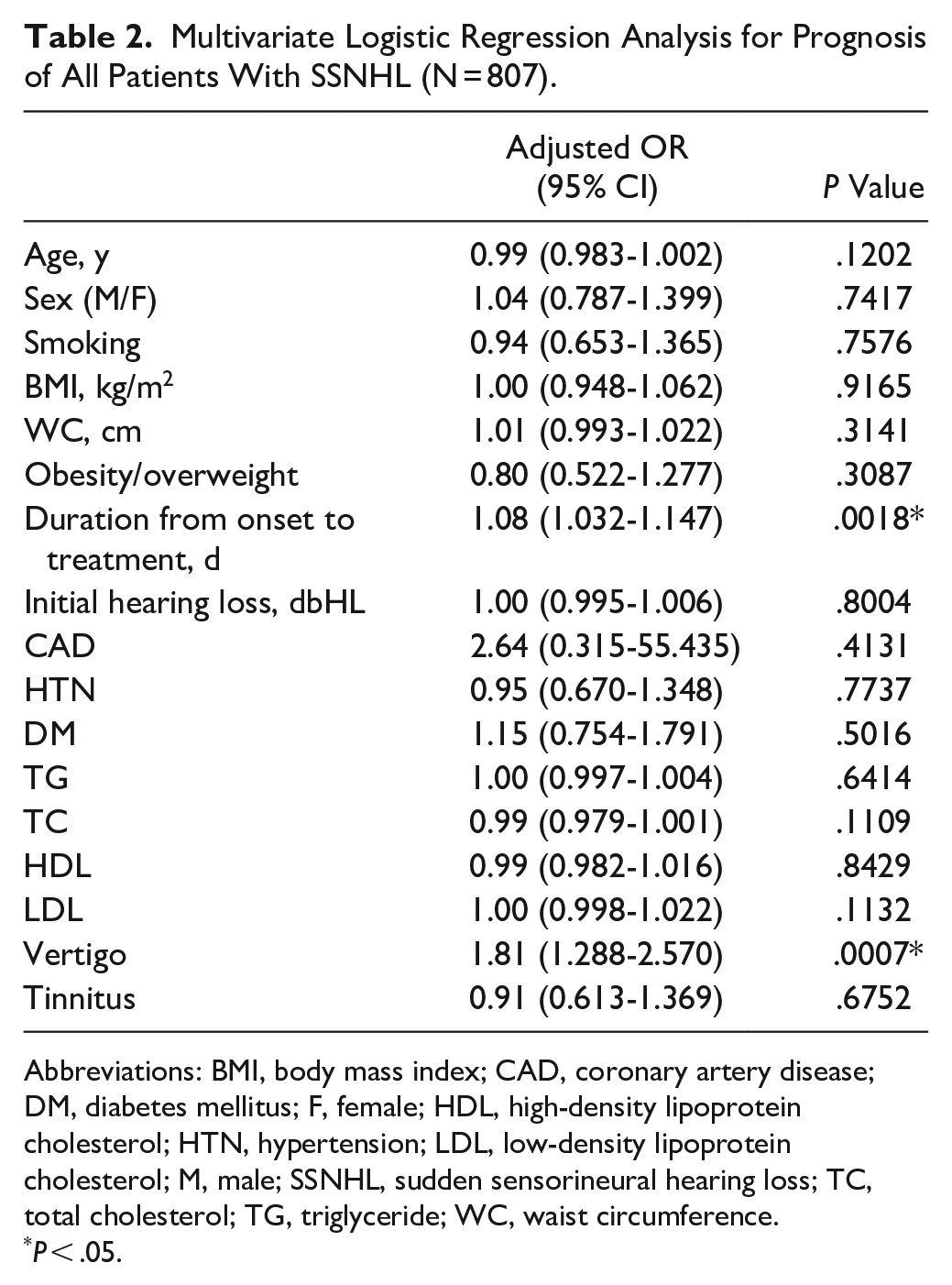
Abbreviations: BMI, body mass index; CAD, coronary artery disease; DM, diabetes mellitus; F, female; HDL, high-density lipoprotein cholesterol; HTN, hypertension; LDL, low-density lipoprotein cholesterol; M, male; SSNHL, sudden sensorineural hearing loss; TC, total cholesterol; TG, triglyceride; WC, waist circumference.
P < .05.
The BMIs of 343 patients (164 men and 179 women) were within the normal range. For these patients, the mean age was 52.56 ± 14.70 years, the mean BMI was 21.41 ± 1.92 kg/m2, and the mean WC was 78.10 ± 10.99 cm. The general characteristics of the 343 SSNHL cases with normal BMIs and the cases categorized into NWNCO and NWCO according to WCs are listed in Table 3. The NWCO group experienced significantly more severe initial hearing loss than the NWNCO group did (73.88 ± 30.18 dB vs 67.27 ± 27.71 dB, P = .0438). In addition, the NWCO group had significantly higher levels of TG (mg/dL, 61.13 ± 38.88 vs 47.19 ± 33.76, P = .0026), TC (mg/dL, 182.61 ± 38.12 vs 171.77 ± 36.77, P = .0144), and LDL (mg/dL, 110.14 ± 33.93 vs 101.11 ± 33.29, P = .0204) than the NWNCO group did. The percentage of poor SSNHL prognoses in the NWCO group was higher (64.94%) than that in the NWNCO group (51.5%). Furthermore, the patients with SSNHL in the NWCO group had significantly poorer prognoses than those in the NWNCO group did (P = .0371). Age, sex, smoking habits, duration from onset to treatment, symptoms of vertigo, comorbidities, and HDL levels did not significantly differ between the NWNCO and NWCO groups.
General Characteristics of Normal BMI (BMI < 24 kg/m2) SSNHL Categorized into Normal Weight Noncentral Obesity (NWNCO) and Normal Weight Central Obesity (NWCO) According to Waist Circumference and the Criteria of the Taiwanese Ministry of Health and Welfare (n = 343).
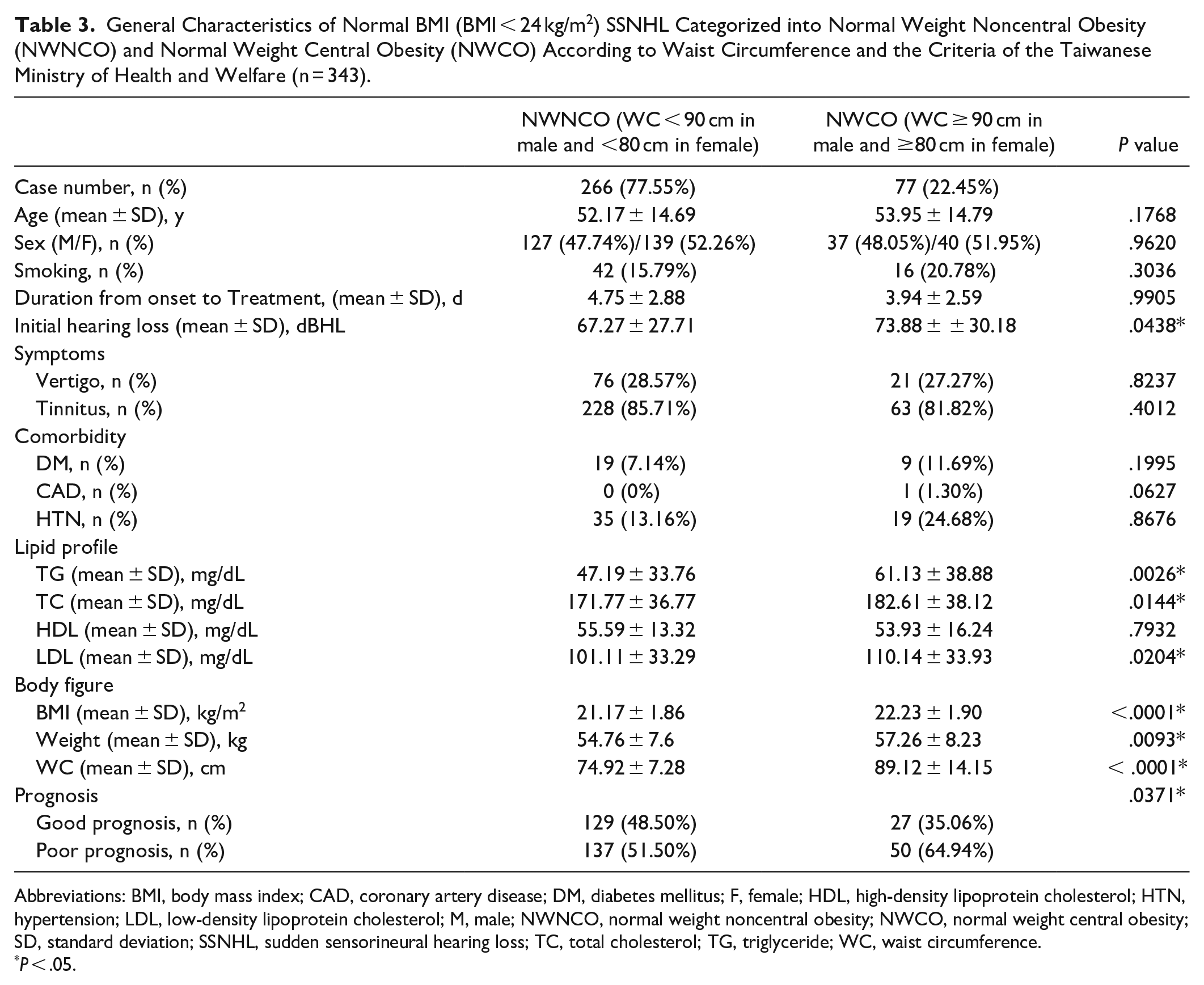
Abbreviations: BMI, body mass index; CAD, coronary artery disease; DM, diabetes mellitus; F, female; HDL, high-density lipoprotein cholesterol; HTN, hypertension; LDL, low-density lipoprotein cholesterol; M, male; NWNCO, normal weight noncentral obesity; NWCO, normal weight central obesity; SD, standard deviation; SSNHL, sudden sensorineural hearing loss; TC, total cholesterol; TG, triglyceride; WC, waist circumference.
P < .05.
The results of the multivariate logistic regression analysis to evaluate the associations between prognoses and patients with SSNHL with normal BMIs after adjusting for age, sex, smoking habit, duration from onset to treatment, initial hearing loss severity, comorbidities, lipid profile, and symptoms are presented in Table 4. Only NWCO (adjusted OR = 2.51, 95% CI = 1.292-5.019, P = .0075), initial hearing loss severity (adjusted OR = 1.01, 95% CI = 1.005-1.021, P = .0014), and vertigo (adjusted OR = 2.13, 95% CI = 1.253-3.688, P = .0058) were significantly associated with SSNHL prognosis. Patients with SSNHL who were in the NWCO group had significantly poorer prognoses than those in the NWNCO group after variable adjustment.
Multivariate Logistic Regression Analysis for the Prognosis of SSNHL Cases With Normal BMI.
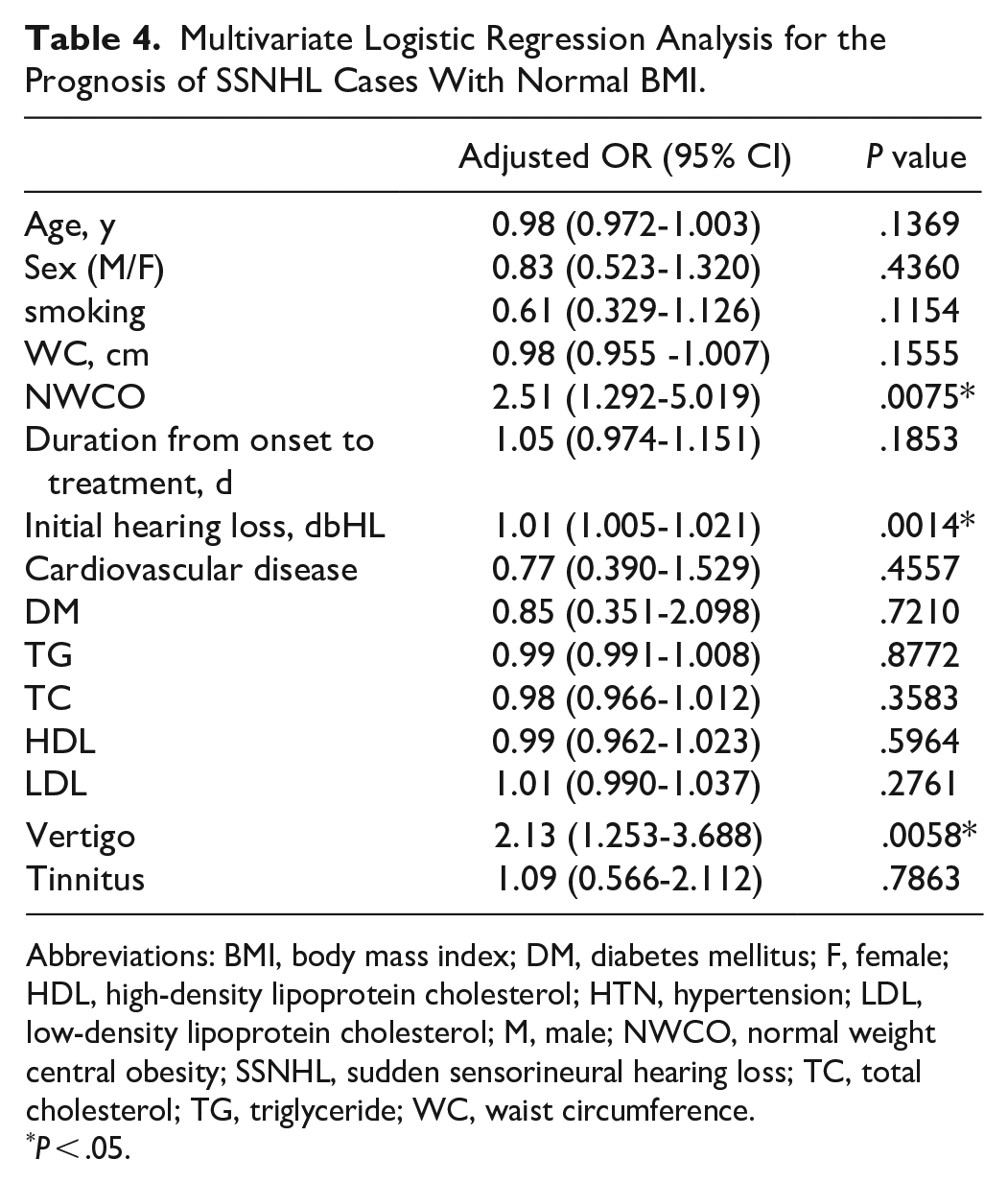
Abbreviations: BMI, body mass index; DM, diabetes mellitus; F, female; HDL, high-density lipoprotein cholesterol; HTN, hypertension; LDL, low-density lipoprotein cholesterol; M, male; NWCO, normal weight central obesity; SSNHL, sudden sensorineural hearing loss; TC, total cholesterol; TG, triglyceride; WC, waist circumference.
P < .05.
Discussion
In this retrospective study, we identified a novel prognosis factor for patients with SSNHL. The rates of favorable prognoses were 45.48% in the nonobese group and 45.91% in the overweight and obese group (P = .9048) and were 48.50% in the NWNCO group and 35.06% in the NWCO group (P = .0371). In isolation, overweight and obesity were not significantly and independently associated with the prognosis of SSNHL (P = .9048), and overweight and obesity with CO were not associated with the prognosis of SSNHL relative to overweight and obesity without CO (P = .6242). However, when we independently compared NWCO and NWNCO cases, the effect of NWCO on the prognosis of SSNHL was significant (P = .0371).
Chau et al 6 reported that the possible etiology of SSHL included idiopathic causes, infectious diseases, otologic diseases, trauma, vascular or hematologic problems, neoplastic diseases, and other causes. Among them, impaired cochlear microvascular circulation has also been proposed as a potential etiology of SSNHL, and because it may be preventable, an increasing number of studies have investigated this topic. Research indicates that the potential mechanism is excess adipose tissue potentially causing mechanical strain on the capillary walls, which then leads to hypoxic damage of the cochlea. 8 Obesity was defined as “abnormal or excessive fat accumulation that may impair health” and was labeled a major cardiovascular disease risk factor by the American Heart Association and the guidelines of the American College of Cardiology. An increasing number of articles have discussed the comorbidities associated with obesity, such as stroke, type 2 DM, hypertension, coronary heart disease, and hearing loss. 21 Studies have demonstrated that a higher BMI correlates with more severe hearing loss.10,22 Hwang et al discussed the role of obesity in the prognosis of SSNHL and reported a nonsignificant odds ratio (95% CI) of 1.04 (0.964-1.131) for the association between BMI and SSNHL recovery for all patients. 13 This negative result may have been due to Hwang et al not employing a BMI cutoff specific to Asian populations; even when patients with the same amount of body fat and the same age and sex are considered, Asian patients generally have a lower BMI than White patients do. This is partly due to differences in body build and muscularity. Moreover, the cutoff points for overweight and obesity among different ethnic groups have different metabolic risks.17,23,24 However, in this study, when only overweight and obesity were considered as influencing factors for SSNHL prognosis, we obtained similar findings to those of Hwang et al. Furthermore, in this study, we were unable to demonstrate a positive relationship between overweight and obesity and SSNHL prognosis, which indicates that evaluating obesity with BMI alone may not be the most significant factor associated with SSNHL prognosis. Although BMI is the most common measure of overall obesity, studies have suggested that use of BMI alone may lead to underestimations of health risks. People with normal BMIs may have higher proportions of body fat distributed primarily as visceral fat, which is strongly associated with cardiometabolic risk. Researchers have come to a consensus that an anthropometric measure of body fat distribution (ie, CO) would be a more favorable predictor for cardiometabolic risk, diabetes risk, and all-cause mortality than BMI and that combining the 2 factors may be an even more favorable predictor. Therefore, NWCO has been proposed as a predictor of such risks.19,20,25 Several studies have demonstrated that the mortality risk for individuals with CO at a normal BMI is similar to or greater than the risk for individuals with CO who are overweight or obese.26-28 Moreover, the literature has demonstrated that visceral adipose tissue is strongly associated with the hearing threshold and that a larger WC is independently associated with hearing loss. Although the underlying mechanisms linking CO and hearing loss are unclear, they are believed to involve a complex network, including macroangiopathy and microangiopathy, redox status imbalance, and neuropathy secondary to metabolic effects.10,29-31
Also, abdominal obesity is a frequently observed component of metabolic syndrome. The incidence of metabolic syndrome has been predicted to increase to approximately 53% by 2035, and metabolic syndrome has been reported to increase the risk of SSNHL.32,33 Chien et al. reported that patients with metabolic syndrome have a 3.54-fold increased risk of developing SSNHL. 34 Therefore, we independently analyzed our cases of SSNHL with normal BMIs that met the criteria for NWCO classification (n = 77, 22.44%). The results indicated significantly poorer prognoses for the NWCO group (adjusted OR = 2.51, P = .0075) than for the NWNCO (n = 266, 77.55%). This finding may indicate a potential novel factor for the prognosis of SSNHL.
To our knowledge, this is the first study to report NWCO as a potential factor in the prognosis of SSNHL. However, this study has several limitations. First, we were unable to collect data on occupational ototoxins, head injuries, and medications, which can affect blood supply and hearing; our data comprised only that recorded during history taking during admission. Furthermore, the self-reporting of lifestyles during history taking is a limitation. Second, findings may differ with ethnicity and race. Finally, the study was limited by its retrospective nature; multicenter studies are warranted to verify the findings of this study.
Conclusion
In this retrospective cohort study, we demonstrated that NWCO was significantly associated with the recovery of SSNHL relative to NWNCO. The findings of our study indicate that medical staff should remain alert in treating cases with NWCO and provide a novel prognostic factor for patients with SSNHL. Understanding the prognostic factors is essential for crafting effective health policies and clinical guidelines for patients with SSNHL. Future studies may expand their scope to other areas related to obesity, such as obstructive sleep apnea and thyroid dysfunction, and their associations with hearing loss. Additional prospective studies including more cases and conducted in different countries are warranted.
Footnotes
Acknowledgements
We would like to thank the audiologists of Kaohsiung Medical University Hospital for their assistance in all the audiology data.
Availability of Data and Materials
The data presented here are available upon reasonable request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Ministry of Science and Technology (Taiwan) for supporting this study with the grant MOST 108-2314-B-037-087; Kaohsiung Medical University Hospital for the grant KMUH109-9M45; Kaohsiung Medical University Hospital for the grant KMUH111-1M41; and Kaohsiung Municipal Siaogang Hospital for the grant Kmhk-111-02 and S-111-15.
Ethics Approval and Consent to Participate
Approval for retrospective data collection/secondary use of health information was obtained from Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-E(II)-20200379).