
Abstract
Objectives:
Fungal tissue invasion in the setting of sinonasal malignancy has been rarely described in the literature. Only a handful of studies have discussed cases of suspected chronic and acute IFS (CIFS and AIFS, respectively), having an underlying undifferentiated sinonasal carcinoma, sinonasal teratocarcinosarcoma, and NK/T-cell lymphoma.
Methods:
Here, we describe 3 cases of carcinoma mimicking IFS from a single institution.
Results:
Each of our patients presented with sinonasal complaints as an outpatient in the setting of immunosuppression. Intranasal biopsies consistently were predominated by necrotic debris, with and without fungal elements, ultimately leading to a delay of oncologic care. The final pathologies included NK/T-cell lymphoma and SNEC. All patients were followed by radiation and chemotherapy, with 1 case of mortality.
Conclusions:
We aim to emphasize the importance of obtaining viable tissue as pathology specimens as the presence of necrosis with fungal elements may limit the diagnosis and ultimately delay the care of an underlying sinonasal carcinoma.
Introduction
Opportunistic invasive fungal infections mimicking malignant processes have been described in various areas of the body; however, few reports exist in the rhinology. Sinonasal malignancies are rare, making up less than 5% of head and neck neoplasms and are associated with a poor prognosis. Symptoms are often nonspecific and include nasal blockage, nasal drainage, epistaxis, or headache, resulting in late presentation. 1 Radiologic features suggestive of a sinonasal malignancy include unilaterality, a distinct mass or soft tissue hyperattenuation, sinus wall destruction, or necrotic elements. These findings are also seen in invasive fungal sinusitis (IFS), making differentiation a challenge. There is a paucity of literature describing acute IFS masquerading an underlying sinonasal carcinoma. Here, we describe 3 cases of sinonasal malignancies mimicking IFS from a single institution.
Methods
We received IRB-exemption for this study.
Case Report
A 75-year-old female with poorly controlled diabetes presented with symptoms concerning for sinusitis. She had significant swelling along the nasolabial fold and upper lip and nasal crusting bilaterally on nasal endoscopy. She was treated with amoxicillin but developed symptom progression despite treatment. A sinus CT showed facial edema with pansinusitis without bony erosion or necrotic elements. Endoscopic sinus surgery (ESS) and palatal biopsies were performed, and histopathology showed nonviable tissue except for fungal elements consistent with Candida species (Figure 1). Despite intravenous micafungin and topical clotrimazole, the disease progressed leading to obvious necrosis of the nasolabial fold and hard palate (Figure 2). After 2 additional operative debridements, pathology showed fungal elements and atypical lymphoid tissue. Molecular testing revealed NK/T cell lymphoma, 11 weeks after initial consult. She was transitioned to radiation and chemotherapy for definitive treatment but subsequently succumbed to her disease.
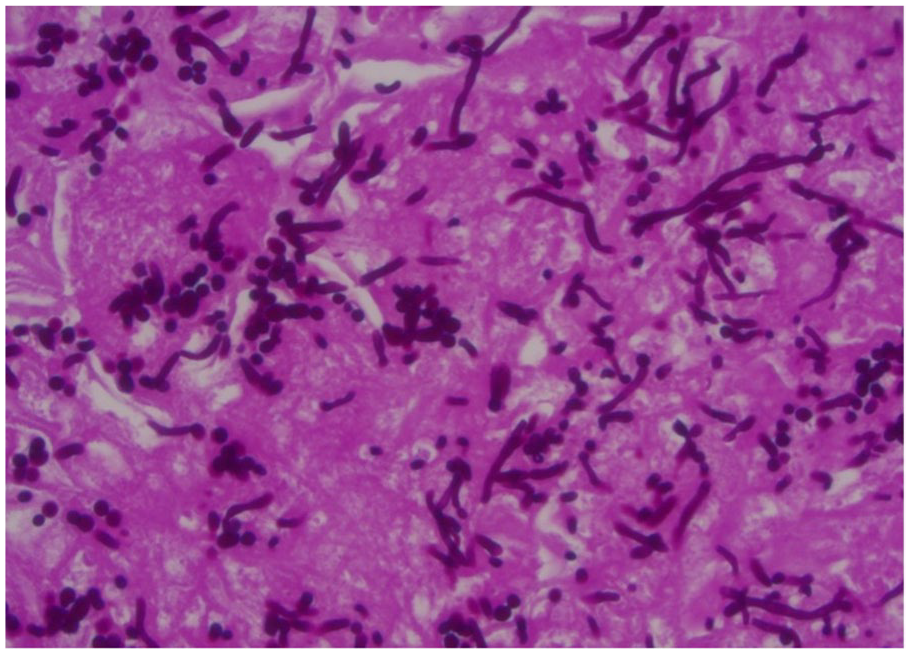
Histopathology illustrating fungal and necro-inflammatory elements on an initial biopsy without viable tissue to differentiate normal or neoplastic cytology.

Extensive nasolabial and palatal involvement in this patient who was found to have NK/T cell lymphoma.
A 70-year-old male with a history of immunosuppression after an organ transplant presented with clinical symptoms concerning for sinusitis with extension into the nasal soft tissues. Cultures were obtained and were consistent with MRSA. The patient was treated with Bactrim without response. He was subsequently admitted for IV antimicrobials and underwent a sinonasal debridement with biopsy. Histopathology showed necrotic debris with fungus morphologically consistent with candida. After clinical improvement, he was discharged with voriconazole and ceftriaxone; however, was readmitted within 1 month with an apparently worsening soft tissue infection. Repeat debridement led to diagnosis of NK/T cell lymphoma; 8 weeks after consult. His care was transitioned to radiation and chemotherapy. Patient is doing well 5 years out from treatment.
A 42-year-old female with chronic rhinosinusitis was referred from an outside otolaryngologist for a possible sinonasal tumor. A sinus CT showed bilateral pansinusitis with a soft tissue mass with orbital and skull base erosion. By the time she presented to clinic, she had about 5 months of worsening symptoms including pressure, discharge, anosmia, and upper lip and dental numbness. Initial biopsy showed abundant dematiaceous fungus and necrotic tissue. Given the lack of an immunocompromised state, a repeat biopsy was performed. Final pathology revealed sinonasal neuroendocrine carcinoma (SNEC), 4 days after initial clinic visit. Endoscopic resection and bifrontal craniotomy were performed with gross total resection followed by adjuvant radiation and chemotherapy. Patient is doing well without evidence of recurrence 1 year out from treatment.
Discussion
As imaging may not rule in or out a sinonasal malignancy in suspected IFS, we rely on histopathology for a definitive diagnosis. In its acute form, IFS requires identification of fungal organisms within tissue, almost always with angioinvasion, often with invasion of bone and other mucosal structures. In addition, tissue infarction and necrosis are invariably present, hence viable tissue may not be seen in these cases. Difficulty arises when histopathology reveals both necrotic and fungal elements without viable tissue to represent the underlying normal versus neoplastic cells. In the described cases, opportunistic fungal superinfection occurred over the necrotic tissue caused by the underlying sinonasal malignancy. There are few similar reports of suspected IFS having an underlying SNUC, sinonasal teratocarcinosarcoma, and NK/T-cell lymphoma.1 -5 We hope to highlight this importance of retrieving viable tissue for histopathology to sufficiently rule out a diagnosis of sinonasal carcinoma. Biopsies of aggressive sinonasal pathologies should include the margin between diseased and non-diseased mucosa, similar to sampling for skin cancer.
While the management of acute IFS involves antifungals, aggressive surgical debridement, and control of the underlying illness, treatment of sinonasal malignancy often involves a different protocol which may include surgery with or without radiation and chemotherapy. As seen in our cases, the delay in diagnosing a sinonasal carcinoma can potentially led to a substantial delay of care.
Conclusion
It is important to hold a high index of suspicion for an underlying sinonasal malignancy in cases of acute IFS until explicitly ruled out. Obtaining viable tissue on biopsy specimens is critical as the presence of necrosis with fungal elements may limit the diagnosis and delay the care of an underlying sinonasal malignancy.
Footnotes
Authors’ Note
Presented at ARS Meeting 2023 in Boston, Massachusetts, USA on May 4, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dennis M. Tang, MD Consultant for Acclarent, Aerin Medical, and 3-D Matrix.