
Abstract
Dear Editor,
In the treatment of early-stage vocal fold carcinoma, transoral CO2 laser microsurgery (TLM) is an important therapeutic alternative. Maximum voice quality outcome is achieved 6 months after TLM, according to the findings of the vast majority of studies exploring the progression of voice quality. 1
In their recent paper, Kinberg et al 2 report the long-term voice outcomes following type I, II, and V cordectomy using objective and subjective voice quality evaluation tools. In particular, they emphasize that voice outcomes following type V cordectomy are similar to those following type I and type II cordectomy, and that superficial anterior or posterior commissure resection may not significantly affect voice outcome.
Although the authors present important findings, they omit information about their post-operative treatment protocol and especially with focus on speech-therapy. On the other hand, our research although validating their observation, provides an additional viewpoint that highlights the significance of postoperative voice therapy in cases with T1 laryngeal cancer that underwent type I, II, or V cordectomies.
We present the results of 40 patients that underwent transoral CO2 laser microsurgery. Approximately 21 of them underwent subepithilial (Type 1), 13 underwent subligament (Type 2) while the rest 6 underwent Type V cordectomy for early stage layngeal carcinoma (T1). Following a 24-hour hospitalization, all patients were discharged with instructions, including a 3-day voice rest regimen and 3 months of proton pump inhibitors to mitigate the effects of laryngopharyngeal reflux. Voice therapy was initiated on the second post-operative week and each patient underwent at least 8 sessions (1 session/week for an hour). The preoperative and 6-month subjective voice quality was evaluated with the Greek version of Voice Handicap Index (VHI) and Grade, Roughness, Breathiness, Asthenia, and Strain (GRBAS) scale, which was retrospectively evaluated by 2 raters.3,4
Twenty patients (Group A) underwent 8 sessions of voice therapy (1 time weekly; 2-month duration), while the rest (Group B) did not. A total of 34 males and 6 females participated. The mean age for each patients’ group was 62.9 ± 10.4 for Group A and 62.4 ± 8.7 years for Group B.
The initial VHI score, for group Α was 53.6 ± 26.9. Six months later, the score was 22 ± 26. A statistically significant decrease in the VHI score was observed (−31.5 ± 27.1, t = −5.195, df = 19, P < .001). In regard to group B, the initial VHI score was 32.4 ± 24.6 and 6 months later the score was statistically significant increased (+9 ± 6.9, t = 5.774, df = 19, P < .001). Moreover, a statistically significant difference was observed between the 2 groups, as those who received voice therapy appeared to improve their scores relative to those who did not (U = 383, N = 40, P < .001).
The initial mean GRBAS score for group Α was 1.7 ± 0.6 while 6 months later, the score was 0.6 ± 0.5, showing a statistically significant decrease (−1.1 ± 0.5, t = −10.7, df = 19, P < .001). In regard to group B, the initial mean GRBAS score was 1.7 ± 0.5, while 6 months later the score was statistical significantly decreased (1.4 ± 0.5). Furthermore, it was noticed that patients who received voice therapy appeared to improve their scores relative to those who did not (t = −7.092, df = 38, P < .001). The VHI scores and GRBAS scale comparison between groups A and B are shown in Table 1.
Descriptives and Comparison Between Patients With and Without Postsurgery Voice Therapy.
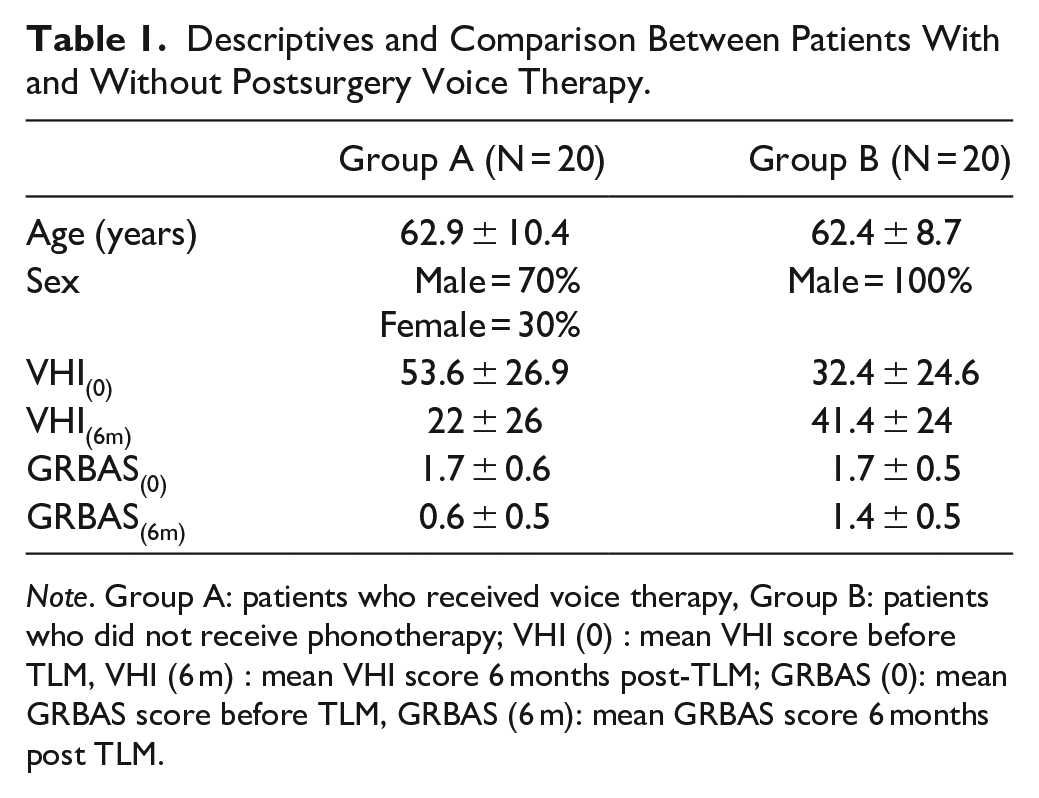
Note. Group A: patients who received voice therapy, Group B: patients who did not receive phonotherapy; VHI (0) : mean VHI score before TLM, VHI (6 m) : mean VHI score 6 months post-TLM; GRBAS (0): mean GRBAS score before TLM, GRBAS (6 m): mean GRBAS score 6 months post TLM.
While other studies report significant decrease of GRABS scale after type I and II cordectomies, 5 our data showed that 8 sessions of voice therapy lead to significant voice improvement after type I, II, and V cordectomies, with the voice attaining nearly normal parameters.
There is no doubt that the establishment of a glottic web favoring glottic closure in patients who have undergone more extensive Type II resections as a consequence of the Type Va resection procedure may contribute to improved glottic competence and voice outcomes according to the findings of Kinberg et al 2 We confirm this observation and add that voice therapy, should aim at the reduction of the glottic gap during phonation, as well as the reduction of vocal fatigue and vocal strain and the improvement of voice intensity. This provides an additional rationale for the improved scores on the VHI and GRABS scales observed in our patients who underwent voice therapy. Moreover, it highlights the importance of post-TLM voice therapy for all patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.