
Abstract
Objective(s):
To quantify and compare pre-procedure worry versus the experience of pain, gagging, and dyspnea during in-office laryngoscopy procedures in patients who did or did not receive pre-procedure anxiolytics, and to explore patient perception of intra-procedure interventions.
Methods:
Patients undergoing awake laryngology procedures at a quaternary care center were enrolled. The State-Trait Anxiety Inventory (STAI) Y1 and Y2 questionnaires were administered to establish baseline levels of state anxiety and trait anxiety, respectively. Pre-procedure and post-procedure surveys assessed patient perception of select interventions.
Results:
34 patients were enrolled (35.3% female, 91.2% white, mean age 60 years). Pre-procedure, 51.5% of patients reported some degree of worry about pain, 61.8% about gagging, 52.9% about dyspnea, and 55.9% about having something in their nose/throat. Post-procedure, 54.5% reported experiencing pain to some degree, 63.6% had gagging, 39.4% had dyspnea, and 78.7% were bothered by having something in their nose/throat. Patients who received a pre-procedure anxiolytic were significantly more likely to report more pain compared to those who did not. The highest rated interventions were pre-procedural education (97.0% “Very helpful”), verbal reassurance (96.9%), provider communicating steps of the procedure (96.9%), and reminders to breathe (87.5%).
Conclusion:
For patients undergoing awake laryngology procedures, the anticipation of gagging, pain, trouble breathing, and scope-related discomfort are worrisome factors. Of these, scope-related discomfort and gagging are the most often-reported sources of intraprocedural discomfort. The interventions patients found most helpful were based on preprocedural education and clear intraprocedural communication, which suggests that purposeful communication has a role in relieving anxiety.
Level of evidence:
Level 4
Introduction
Recent technological and medical advancements have encouraged the increase of in-office medical procedures, which offer many advantages including lower procedural risks and cost. 1 Overall, awake laryngeal procedures are safe and well-tolerated by patients,1 -6 and have high procedural completion rates.7,8 However, preprocedural and intraprocedural anxiety remains an important clinical concern. In one study of patients undergoing awake in-office laryngeal procedures, 81% experienced some degree of anxiety, with 49% of those reporting moderate levels and 14% reporting severe or unbearable levels of anxiety. 7 Moreover, patients undergoing laryngoscopy for the first time reported significantly higher levels of fear compared to those undergoing repeat exams, 9 indicating that certain subsets of patients may require additional interventions to create a positive experience.
Patient-centered care requires physicians to seek a deeper understanding of the patient experience. Current research has quantified the intensity of anxiety and fear when it comes to awake laryngoscopy9 -11 and related procedures, 7 yet little is known regarding the specific factors driving these symptoms. Additionally, there is a need to identify specific interventions most effective at addressing patient anxiety. To address these gaps in the literature, we are seeking to identify aspects of in-office laryngology procedures that contribute to patient anxiety and to discern which interventions patients find most helpful.
Materials and Methods
Approval for this study was obtained from the institutional review board at the Mayo Clinic. This was a prospective, observational study based on a laryngology practice at a quaternary care center. Between June 15, 2023, and December 15, 2023, consecutive patients planning to undergo 1 of 3 common awake laryngoscopy procedures (vocal fold injections with hyaluronic acid gel, flexible laryngoscopy with KTP laser of the vocal cords, and flexible laryngoscopy with transcervical injection of triamcinolone for subglottic stenosis) were evaluated for enrollment in the study. Patients were approached by a clinical research coordinator not involved in their medical care and were informed that study participation status would be blinded to the direct care team. In all, 45 patients consented to enroll in the study. Of these, 11 ultimately did not need their anticipated procedure, leaving 34 patients who completed the study. All patients were at least 18 years old.
On the day of the procedure, subjects completed a pre-survey designed to examine their level of worry about several pre-identified factors that could impact patient comfort via 5-point Likert scale. There was an additional free-response section. The STAI Y1 and Y2 forms were also administered, designed to assess state anxiety and trait anxiety, respectively. The STAI questionnaire is an established clinical tool for the measurement of anxiety 12 and is commonly used in ENT research.13 -21 State anxiety describes how the patient feels at that moment, while trait anxiety refers to habitual feelings at baseline.
Pre-procedure anxiolytic medications were prescribed and administered at the discretion of practitioner performing the procedure and were taken after completion of the above surveys. The decision to administer an anxiolytic is a shared decision-making process based on patient preference, tolerance of past procedures and the diagnostic scope exam, and subjective levels of anxiety assessed by the practitioner during the preoperative office visit. Prescribed anxiolytic included diazepam 2 to 5 mg depending on patient’s body habitus and level of alcohol use.
Procedures were performed by 2 fellowship-trained laryngologists at a single institution. As part of standard care, all patients received verbal preprocedural education from a physician prior to the procedure day. During the procedure, patients were given the option of having music of their choice played in the room and the option of having the lights dimmed. A family member or friend, if present, was invited to stay in the room during the procedure at the patient’s discretion. Topical anesthesia was instilled, including 2 to 3 cc of phenylephrine/2% lidocaine spray intranasally, 1 application of 20% benzocaine to the oral cavity for any transoral procedure, up to 8 cc of 4% nebulized lidocaine, and 2 to 3 cc 4% topical lidocaine applied directly to the vocal cords. The laryngoscope was advanced transnasally. During vocal fold injections, a transoral injector was inserted into the patient’s mouth simultaneously. Throughout the procedure, the physician communicated each step with the patient and cued relaxed breathing. Verbal reassurances and physical touch to the upper back and shoulders (with patient permission) were used.
Total duration for each of the procedures (including preparation time and the procedure itself) generally range from 30 to 40 minutes for KTP laser of the vocal folds and 20 to 35 minutes for vocal fold and subglottic injections.
Immediately after procedure completion, a post-survey was administered, also designed by the research team. Levels of discomfort related to pain, gagging, and other factors were assessed via 5-point Likert scale, and patients were asked to rate the helpfulness of selected interventions. A free-response section was included.
Due to small numbers per group, transoral vocal fold injections and percutaneous transcervical triamcinolone injections were grouped together as “injection-type” procedures. This decision was based on previous findings suggesting that patient-reported discomfort did not differ significantly between transoral and transcervical approaches. 7
Explicit responses to specific survey items are shown summarized by the number and percent of respondents choosing each category. Continuous responses were summarized with mean and standard deviation (SD), while categorical responses were summarized with median and IQR. Due to small numbers of responses in many item categories, comparisons between the 2 levels of anxiolytic use and features of interest were performed using non-parametric approaches. Fisher’s exact test for categorical or Likert style responses and Kruskal-Wallis tests was used for continuous measures. Statistical analyses were performed using SAS version 9.4 (SAS Institute; Cary, NC). All tests were 2-sided and P-values less than .05 were considered significant. Qualitative data was analyzed manually by the authors. Responses were coded and grouped according to keywords using a thematic analysis framework. 22
Results
Demographics/Overview
A total of 34 patients were enrolled in the study and subsequently underwent awake, in-office procedures, performed by 2 laryngologists at a single institution during a 6-month period. In all, 12 (35.3%) subjects were female, 31 (91.2%) were white, and the mean age was 60 years (median 64; range 25-82 years). In all, 21 patients (61.8%) underwent a repeat procedure, and 13 (38.2%) underwent a first-time procedure. In total, 21 patients (64.7%) received KTP laser treatment of the vocal folds, 10 (29.4%) received vocal fold injections with hyaluronic acid gel, and 2 (5.9%) received transcervical subglottic injection with triamcinolone. These data are summarized in Table 1.
Demographics.

Note. (%) unless stated otherwise.
State-Trait Anxiety Inventory (STAI)
The mean overall STAI Y1 (state anxiety) score was 32.7 (range 20-56, SD 10.8). In the literature, a STAI Y1 score >39 to 40 is considered clinically significant anxiety. 12 For patients prescribed a pre-procedure anxiolytic (n = 10), mean STAI Y1 was 37.1. For patients who were not prescribed an anxiolytic (n = 24), mean STAI Y1 was 30.9.
The mean overall STAI Y2 (trait anxiety) score was 33.3 (range 20-53, SD 8.8). For the group who later received an anxiolytic, the mean STAI Y2 was 35.6. The no-anxiolytic group had a mean STAI Y2 score of 32.3. Normative STAI Y1 and Y2 values vary according to population, but for the average working adult tend to fall between 34 and 35. 23
STAI scores were not significantly different (Y1, P = 0.16; Y2, P = 0.23) between the anxiolytic and no-anxiolytic groups (Table 2).
STAI Results.

Kruskal-Wallis P-value.
Pre-Procedure Survey
Pre-procedure, 51.5% (n = 17) of patients reported some degree of worry about pain, 61.8% (n = 21) about gagging, 52.9% (n = 18) about trouble breathing, and 55.9% (n = 19) about having something in their nose/throat (Figure 1). There was no significant difference in reported degree of worry between the anxiolytic and no-anxiolytic groups.
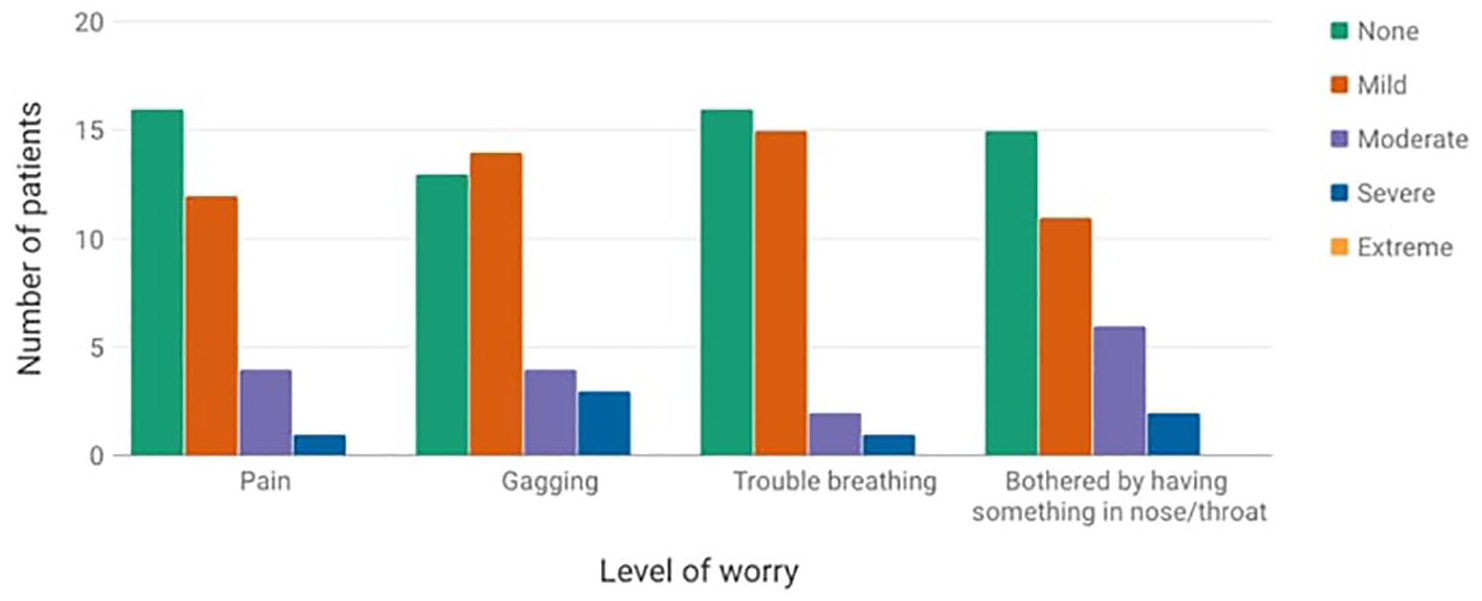
Pre-survey results for patient-reported level of worry regarding specific aspects of procedure.
Post-Procedure Survey
Post-procedure, 54.5% (n = 18) of respondents reported experiencing pain to some degree, 63.6% (n = 21) had gagging, 39.4% (n = 13) had dyspnea, and 78.7% (n = 26) were bothered by having something in their nose/throat (Figure 2). Patients who took a pre-procedure anxiolytic were significantly more likely to report higher levels of pain during the procedure (P = .04, Table 4).
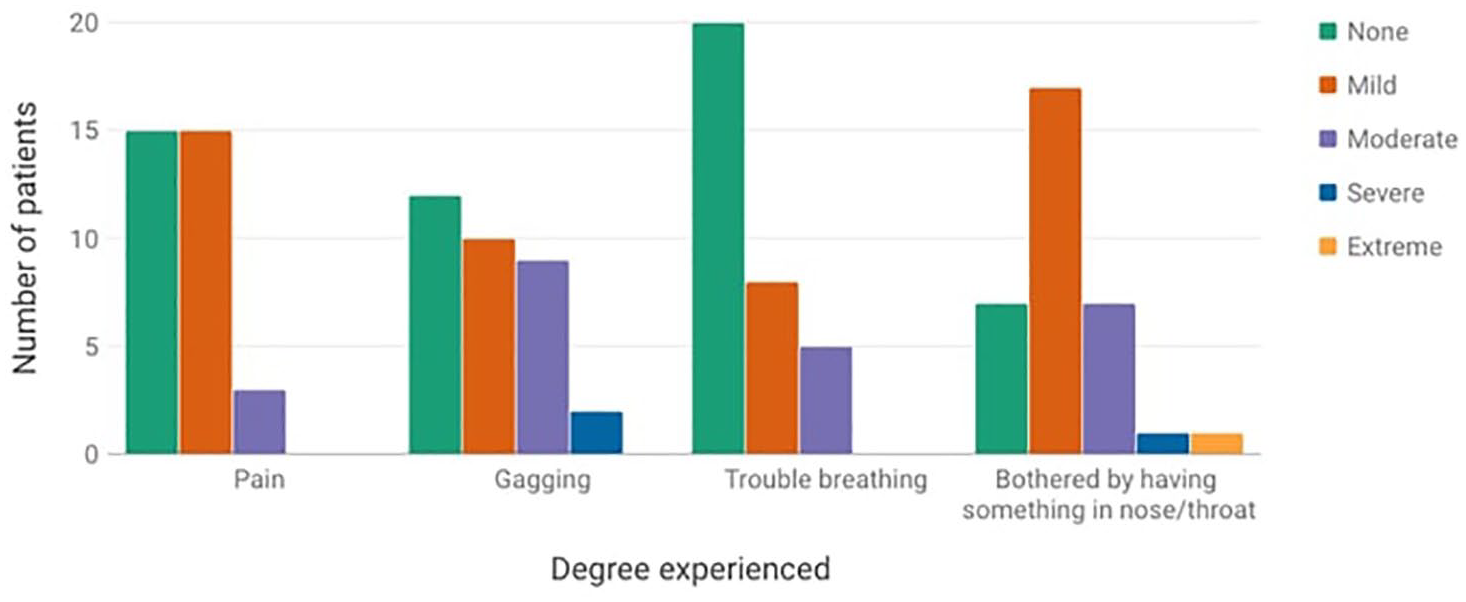
Post-survey results for patient-reported degree of experience of specific aspects of procedure.
33 of 34 patients (97.1%) answered that they would repeat the awake procedure if it were medically recommended.
Interventions were overwhelmingly rated as “very helpful.” Highest rated interventions were “education about the procedure” (97.0% rated “very helpful”), “verbal reassurance” (96.9%), “provider communicating steps of the procedure” (96.9%), and “reminders to breathe” (87.5%). The interventions perceived as less helpful were “music played” (70.4%) and “having a family member or friend stay in the room” (69.6%).
Those undergoing injection-type procedures (as opposed to KTP laser) reported higher pre-procedure anxiety about having trouble breathing (P < .01, Table 3) and reported experiencing more trouble breathing during the procedure (P < .01, Table 4). Subjects taking regular anti-anxiety medication were significantly more likely to report experiencing trouble breathing during the procedure than those not on regular medication (P < .01, Table 4). Females reported higher levels of pre-procedural anxiety about trouble breathing (P = .05, Table 3) and experienced more subjective trouble breathing (P = .03, Table 4). Those undergoing repeat procedures reported experiencing more discomfort at having the scope in the nose/throat compared to those undergoing first-time procedures (P = .01, Table 4).
Pre-Procedure Survey Results.
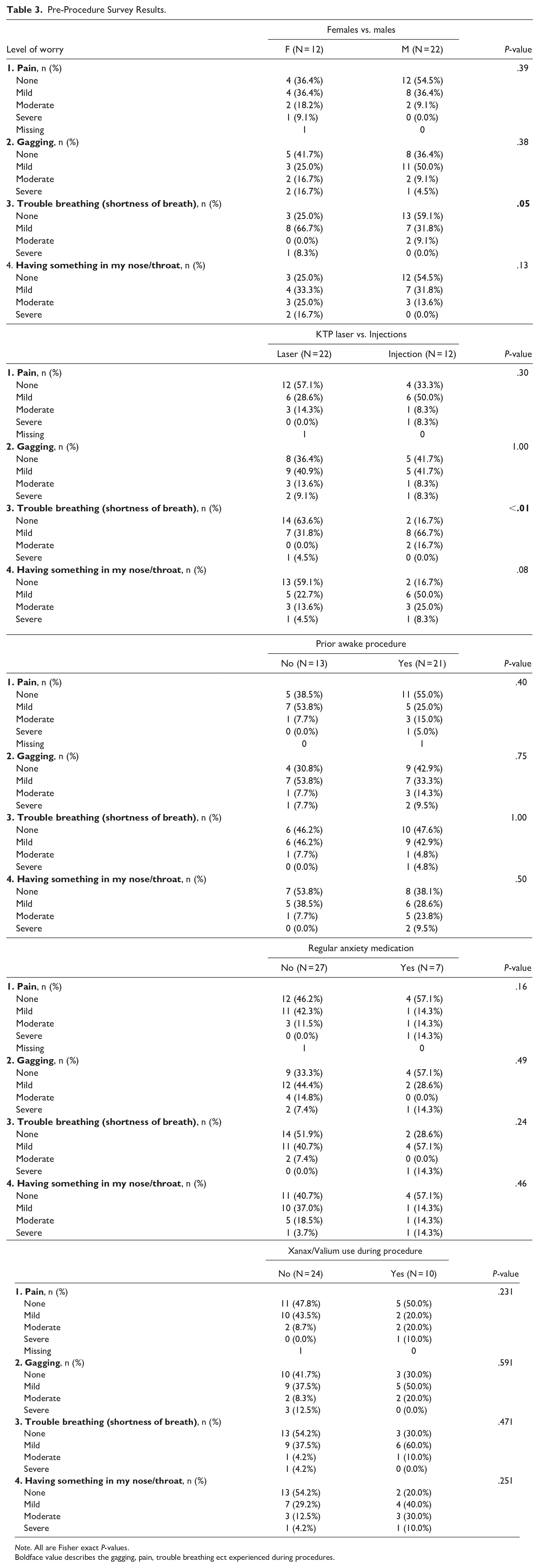
Note. All are Fisher exact P-values.
Boldface value describes the gagging, pain, trouble breathing ect experienced during procedures.
Post-Procedure Survey Results.
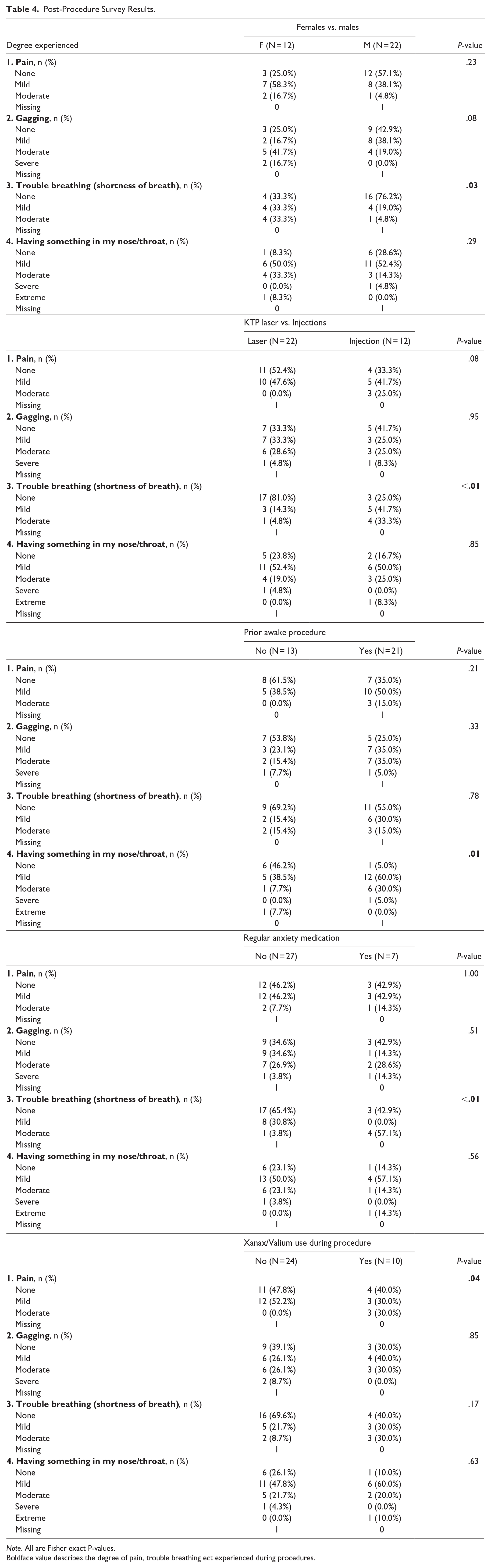
Note. All are Fisher exact P-values.
Boldface value describes the degree of pain, trouble breathing ect experienced during procedures.
Qualitative Data
Open-ended responses to the pre-procedure question “Is there anything else about the procedure today that worries you or causes you stress or anxiety?” were analyzed. Some participants endorsed anxiety regarding the outcome of the procedure (n = 8) and cited fear of the needle involved in their procedures (n = 2). Concern was expressed about needing to swallow saliva but not being able to during the procedure (n = 2). Additional concerns included use of the laser (n = 2), length of the procedure (n = 2), and potential for airway closing during the procedure (n = 1).
Similarly, responses to the post-procedure question “Was there anything unexpected about the procedure that caused you stress, anxiety, worry, or concern?” were analyzed. Patients mentioned pain (n = 3) and 1 patient cited a sensation of airway swelling.
The post-procedure question “Is there anything else your doctor or care team could have done to improve your experience?” elicited the following responses: use of a smaller scope (n = 1), saliva management (n = 1), and lying down rather than sitting up for the procedure (n = 1).
Discussion
Previous studies have found that awake office-based laryngeal procedures are well-tolerated overall, and that anxiety and pain levels are generally mild.5 -8 Our study is the first to investigate the specific factors causing anxiety for patients undergoing awake laryngeal procedures. Additionally, this study is novel in assessing patient perception of interventions that target procedure-related anxiety.
Our study demonstrates that when it comes to awake laryngeal procedures, the possibility of pain, gagging, trouble breathing, and scope-related discomfort are worrisome factors to half of patients. The median pre-survey response for all 4 factors (pain, gagging, trouble breathing, and scope-related discomfort) was “2,” representing “a little worried.” Similarly, Young et al 7 found that anxiety levels tend to be mild-to-moderate before awake laryngeal procedures.
A study done by Paul et al 9 found that patients undergoing awake flexible laryngoscopy (without a procedural component) for the first time reported higher levels of fear compared to those undergoing repeat laryngoscopy. Our study did not demonstrate a difference in levels of fear between those undergoing first-time awake laryngeal procedures versus repeat procedures. We hypothesize this is because patients undergoing laryngeal procedures have already undergone diagnostic scope examination, unlike the first-time scope cohort in Paul et al.’s study, thus much of the unknown (e.g., what the scope will feel like) is eliminated. Regardless, the repeat-procedure cohort experienced more scope-related discomfort than the first-time cohort.
Two factors, gagging and having the scope in the nose/throat, caused (1) the most pre-procedural anxiety and (2) the most discomfort during the procedure. Having a scope in the nose/throat was rated as the most bothersome intraprocedural aspect to patients, which aligns with Paul et al.’s 9 findings.
There were several groups who reported experiencing trouble breathing at significantly higher rates than their counterparts: females, patients undergoing injection-type procedures, and patients regularly taking antianxiety medication.
For females, the levels of both pre-procedural worry and intraprocedural experience of trouble breathing were greater than male counterparts. This finding may warrant that the treating laryngologist pay close attention to the female patient’s subjective experience of breathing difficulty and consider providing additional breath coaching during awake laryngeal procedures.
Of the 12 patients who underwent injections, 10 were vocal fold injections which are commonly performed for underlying vocal fold paralysis. This disorder can manifest with dyspnea at baseline, 6 which we propose could account for the increase in experienced trouble breathing. Further, vocal fold injection involves 2 proceduralists standing in front of the patient with both transnasal placement of the scope and transoral placement of an injector device. Additionally, the patient’s tongue is lightly grasped and held in protrusion with gauze. This additional equipment, personnel, and manipulation of the airway could account for a perceived increase in trouble breathing during the procedure. It is notable that for both females and those undergoing injection, the anticipation of trouble breathing was associated with greater subjective breathing difficulty. Thus, the laryngologist might identify patients for whom subjective dyspnea is a concern and provide additional counseling and support accordingly.
Lastly, patients who reported regularly taking an anti-anxiety medication were significantly more likely to experience shortness of breath during the procedure. Shortness of breath can be a symptom of anxiety, and thus could potentially explain this finding. However, further study in this population is warranted.
Our study corroborated many others showing that patient-reported pain levels after awake laryngeal procedures is low.4,5,11 Interestingly, patients who took a pre-procedure anxiolytic reported statistically higher levels of pain on average (P = .04). We would expect the opposite relationship, as anxiolytics are understood to blunt pain perception.24 -26 A reasonable hypothesis would be those requiring an anxiolytic may have higher baseline levels of anxiety, which could then be associated with higher perception of pain during the procedure. However, neither STAI Y1 (state anxiety) nor Y2 (trait anxiety) differed significantly between the anxiolytic and no-anxiolytic groups (Table 2). Our findings in this regard are contradictory and warrant further study on the utility and decision-making process of prescribing a pre-procedure anxiolytic in patients undergoing awake in-office laryngeal procedures.
The single patient from our study who would not undergo the awake procedure again commented in the free-response section that they “would rather be knocked out.” This patient also reported relatively high preprocedural anxiety (“a little worried” about pain and trouble breathing, “moderately worried” about having the scope in the nose/throat, and “very worried” about gagging). Additional free-response answers indicated fear of the needle used in vocal fold injection, length of the procedure, and how long the results of the procedure would last. In the post-survey the patient reported mild pain, no trouble breathing, moderate scope-related discomfort, and moderate gagging. It was this subject’s first awake procedure. The patient did not receive a pre-procedure anxiolytic and was not on regular antianxiety medication. STAI Y1 score was 41, where >39 to 40 is considered clinically significant anxiety 12 ; Y2 score was 34, which is average according to normative data from the STAI manual. 23
It is worth asking whether this patient would have benefitted from a pre-procedure anxiolytic. Decisions to administer an anxiolytic are at the treating laryngologist’s discretion, and considerations include patient preference, tolerance of the scope on diagnostic exam, and the practitioner’s subjective assessment of anxiety levels. Again, currently it is not well understood whether there is any benefit to prescribing pre-procedure anxiolytics in this setting, and there is no standard procedure to predict appropriate candidates for this therapy. Our study highlights the need for further studies on this topic.
The qualitative data reveals that patients are often anxious about procedural outcomes, including efficacy, longevity of results, and the potential for complications. Patients should be encouraged to explore their concerns related to these topics, and pre-procedural education should be tailored accordingly. Another potentially addressable concern was salivation and needing to swallow during the procedure. Patients may benefit from education regarding this possibility, along with supportive measures like providing suction as needed.
Most interventions were perceived positively by patients. Interventions that patients rated as most helpful were education about the procedure, verbal reassurance, and the provider communicating steps of the procedure. This is noteworthy, as these interventions are based on the provider providing clear verbal communication to the patient.
Overall, our study suggests that purposeful communication from the provider has a role in relieving anxiety for patients undergoing awake laryngology procedures. Prior to the procedure, there is an opportunity for the physician to address specific fears related to intraprocedural discomfort, gagging, and difficulty breathing. These conversations could help dispel some of the associated anxiety and lead to a better patient experience. Further, our findings show that patients find intraprocedural communication from the physician helpful in decreasing anxiety.
Limitations
One notable limitation to our study is its small sample size, which may limit its generalizability to broader populations. Additionally, the ethnic breakdown of our cohort reflects the patient population in the clinic location where this study was performed, but it is not racially diverse. Further studies should aim to include a larger and more diverse sample for results to be widely generalizable.
There is likely an element of response bias especially with the method used to rate the helpfulness of interventions. Given the survey-style approach, some patients may have felt compelled to select positive responses (“e.g., very helpful”) due to acquiescence bias. Additionally, patients might have believed that their responses would be visible to the physicians or care team, despite being informed before enrolling in the study that their responses would be kept confidential from the care team.
Conclusion
In-office awake laryngoscopy procedures generally produce mild levels of anxiety. The possibility of pain, gagging, trouble breathing, and scope-related discomfort are worrisome factors to half of patients. Patients frequently worry about procedural outcomes, the length of procedure, and the potential for complications, and a smaller proportion of patients are fearful of needle and laser usage. We can target specific factors that cause anxiety through patient education and clear intraprocedural communication, both of which are well-received and valued highly by patients.
Our data was inconclusive regarding the benefit of preprocedural anxiolytics in a subset of patients. Further studies are warranted to explore the efficacy of preprocedural anxiolytics in this population and to help identify patients who might benefit most from anxiolytic therapy.
Scope-related discomfort tends to be the most bothersome factor overall to patients undergoing awake laryngeal procedures. Gagging, pain, and trouble breathing are also commonly cited. Additionally, patients should be proactively counseled regarding saliva production and the need to swallow during the procedure.
Footnotes
Acknowledgements
None
Author’s Note
Presented at the 104th Annual Meeting of the American Broncho-Esophagological Association At the Combined Otolaryngology Spring Meetings Chicago, IL, USA
May 15th, 2024
Consent to Participate
Written informed consent was obtained from all participants involved in this study. Participants were provided with detailed information about the study’s purpose, procedures, potential risks, and benefits before giving their written consent to participate. All participants were assured of their right to withdraw from the study at any time without penalty. The confidentiality and anonymity of participants were maintained throughout the study, with personal data stored securely and accessible only to authorized research personnel.
Consent for Publication
Not applicable.
Data Availability
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was conducted in accordance with the ethical standards outlined by the Institutional Review Board (IRB) at the Mayo Clinic. The research protocol was reviewed and approved by the Mayo Clinic IRB (Approval Number: 23-005492), ensuring that all procedures adhered to ethical guidelines and standards for the protection of human subjects.