
Abstract
Objective:
To assess the efficacy and safety of simultaneous labyrinthectomy and cochlear implantation (CI) in patients with refractory Ménière’s disease (MD).
Methods:
A retrospective review of patients with definite refractory MD per American Academy of Otolaryngology—Head and Neck Surgery treated via simultaneous transmastoid labyrinthectomy and CI was performed at a tertiary referral center. Patients’ clinical and audiometric outcomes were assessed and analyzed.
Results:
Twenty-four patients underwent simultaneous transmastoid labyrinthectomy and CI between 7/2015 and 9/2023 (median age = 58 years [interquartile range (IQR) = 43.5-64.5], 54% female). Complete resolution of vertigo occurred in 23 patients (96%). Evaluating available data at ≥6 months postoperatively, both CNC (n = 9; 36% vs 40%, P = .76) and AzBio scores (n = 13; 40% vs 62%, P = .15) improved after surgery. When performing a sound localization task with the CI on, the median score in identifying the noise was 32% (IQR = 22%-56%) with a median degree error of 27.9 (IQR = 15.8-38.0) versus a median score with the CI off of 20% (IQR = 14%-42%) with a median degree error of 43.8 (IQR = 21.9-73.5) at a median of 9.8 months (IQR = 6.7-14.6) from surgery.
Conclusions:
The present study represents one of the largest cohorts of refractory MD patients undergoing simultaneous labyrinthectomy and CI. Combining these procedures appears safe, enables excellent control of vertigo, and expedites aural rehabilitation in appropriately selected candidates, but future study is warranted to continue to evaluate this treatment paradigm.
Introduction
Ménière’s Disease (MD) is a debilitating disease characterized by recurrent episodes of vertigo and fluctuating sensorineural hearing loss (SNHL) that can have a profound impact on patient quality-of-life given its variability and unpredictability.1
-3 Management is typically focused on control of vertigo, with data supporting more conservative medical therapy as the initial management for most patients.
4
Persistence of symptoms despite these medical interventions typically requires escalation toward more invasive and ablative therapies; however, these treatments notably increase the risk to hearing and are reserved for patients with more substantial degrees of hearing loss. Perhaps the most consistently effective destructive therapy is labyrinthectomy, which serves as the final step in the management algorithm proposed by the American Academy of Otolaryngology—Head and Neck Surgery (AAO
CI placement within the single-sided deafness (SSD) population has now become accepted practice with good audiometric and clinical results noted and the potential for re-establishment of binaural hearing.9 -11 Acknowledging this, post-labyrinthectomy MD patients represent an ideal population where this practice can further expand, with the hope that this can mitigate its largest drawback. To this point, some recent studies have explored the topic of labyrinthectomy and CI insertion. Overall, these largely consist of case series12 -17 or meta-analyses,18,19 but, considering the potential benefits and reported results in these publications, the practice of simultaneous labyrinthectomy and CI insertion has been adopted at the authors’ primary institution for patients with refractory MD. The present study seeks to describe a large cohort of patients that underwent this combined procedure and critically evaluate its success in disease control and aural rehabilitation.
Methods
Institutional Review Board approval was obtained (protocol #2023H0353). Potential patients treated during 7/2015 to 9/2023 at the authors’ primary institution were identified in the electronic medical record via diagnosis and procedure codes, and their charts were reviewed for candidacy. Patients were included if they carried a diagnosis of definitive primary MD as per AAO-HNS1,2 and international consensus guidelines 3 and had their disease managed via transmastoid labyrinthectomy with simultaneous CI placement. Patients were excluded if they did not carry this diagnosis, if they underwent labyrinthectomy for other indications, and if these procedures were performed sequentially rather than simultaneously.
Relevant data were extracted including demographic information, clinical history, pre- and postoperative audiometric testing, preoperative vestibular testing, surgical details, and postoperative course. All surgeries and care were performed by fellowship trained neurotologists at the primary institution. Decision-making regarding labyrinthectomy was made as a joint decision between patient and provider based on symptomatology, audiologic function, and prior treatments. Pure-tone average (PTA) was calculated as an average of the sound thresholds at 500, 1000, and 2000 Hz per institutional protocol. CI candidacy and postoperative testing was performed via Consonant-Nucleus-Consonant (CNC) word testing 20 and AzBio sentence testing 21 using recorded materials presented at 60 dB sound pressure level (SPL) from the 0° azimuth. For ear specific testing, contralateral masking was performed with sound and ear plugging. The appropriate masking sound level was calculated based on the level of hearing in the non-operative ear. Follow-up was recorded until the most recent available appointment, and inclusion of audiometric data in analysis only occurred if recorded 6 months or greater from the time of surgery. Sound localization was tested via a 7-speaker array producing a 500 ms pink noise stimulus with 100 trials per condition (Figure 1). Four different conditions were tested including tests with the CI off and on at 50 and 60 dB SPL, with a preference for 60 dB SPL in analysis. Patients were both assessed on percent correct and degree of error based on their assessment of the sound location. Assessment of vertigo control was based on subjective patient report during follow-up. To assess the impact of tinnitus on patient quality-of-life, the Tinnitus Handicap Inventory (THI) was administered in some cases. 22 Vestibular testing included a battery of tests assessing both ears independently via caloric testing and video head impulse testing to determine the presence of an ear specific peripheral vestibular deficit. Vestibular testing was only included if performed within 12 months of surgery without any intervening procedures to assure accurate preoperative representation of vestibular function.
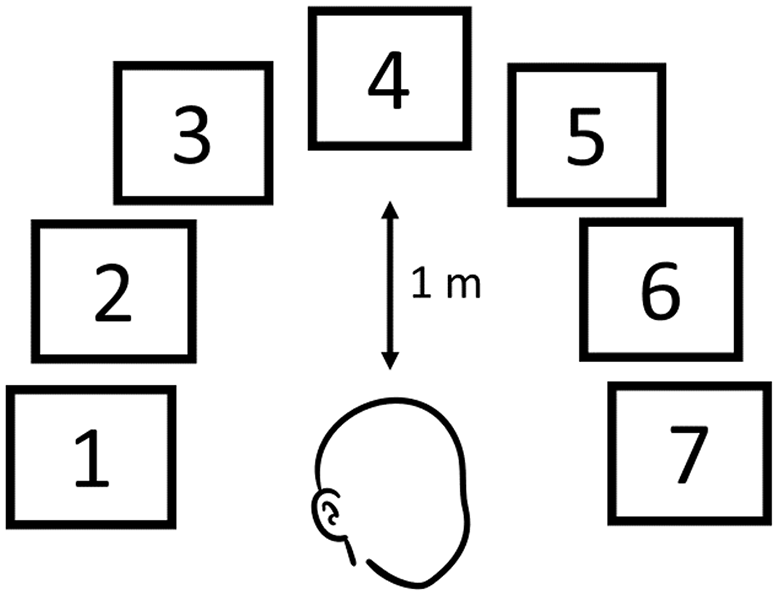
Schematic of the sound localization task utilized in this study.
All surgeries were performed through a postauricular incision. A wide mastoidectomy was performed. The facial nerve was skeletonized. After posterior tympanotomy, a labyrinthectomy was performed. The semicircular canals were entered and drilled with particular attention to their ampullated ends. The vestibule was entered, and all sensory neuroepithelium was then removed. The round window niche was drilled away, exposing the round window membrane, and a round window cochleostomy was performed. The CI electrode was inserted in the standard fashion, and the incision was closed in a multi-layered fashion. All surgeons utilized their electrode of choice, with both straight and peri-modiolar electrodes being used. Advanced Bionics (Valencia, CA) and Cochlear Limited (Sydney, Australia) did provide research support through device provision for a portion of this cohort.
Data were primarily analyzed through descriptive statistics, with categorical features summarized through frequencies and percentages and continuous features through medians and interquartile ranges (IQRs). To evaluate improvement in audiometric testing, paired student t-tests were performed to assess for statistical significance, with a P-value <.05 being considered statistically significant. All statistical analyses were performed on Microsoft Excel (Microsoft Corporation, Redmond, WA).
Results
During the study period, 24 patients underwent simultaneous transmastoid labyrinthectomy and CI insertion for management of definitive MD. Demographic information is listed in Table 1. All patients underwent this procedure as planned without immediate complication. All patients were prophylactically admitted after surgery for symptomatic control with a median discharge on postoperative day 1 (IQR = 1-2). One patient (4%) underwent a tympanoplasty at the time of surgery as well to repair their tympanic membrane perforation after prior intratympanic steroid injections. After appropriate healing, a persistent perforation was noted, leading to subsequent ear canal closure. No issues were noted with the implant despite the need for this additional surgery. After discharge, 1 patient (4%) was noted to have transient, incomplete postoperative facial nerve weakness that occurred after discharge but before the initial postoperative evaluation approximately 3 weeks after surgery. This patient was treated with steroids after evaluation was negative for a stroke. Given the timing, this likely represented delayed inflammation or viral reactivation after surgery, and function improved to House-Brackmann (HB) grade I in time. Two patients (8%) were noted to have electrode malpositioning identified through a combination of poor initial implant function and postoperative CT scan. One of these patients underwent revision with improved audiometric outcomes noted postoperatively, and the other has recently undergone revision with limited audiometric testing thus far. One patient (4%) required device removal due to infection 32 months after their initial surgery. Of note, this patient carried multiple complicating co-morbidities, including uncontrolled diabetes mellitus, at the time of infection. Unfortunately, given insurance difficulties, this patient has not been able to undergo re-implantation.
Demographics of Patients undergoing Simultaneous Transmastoid Labyrinthectomy and Cochlear Implantation (n = 24, unless otherwise noted).
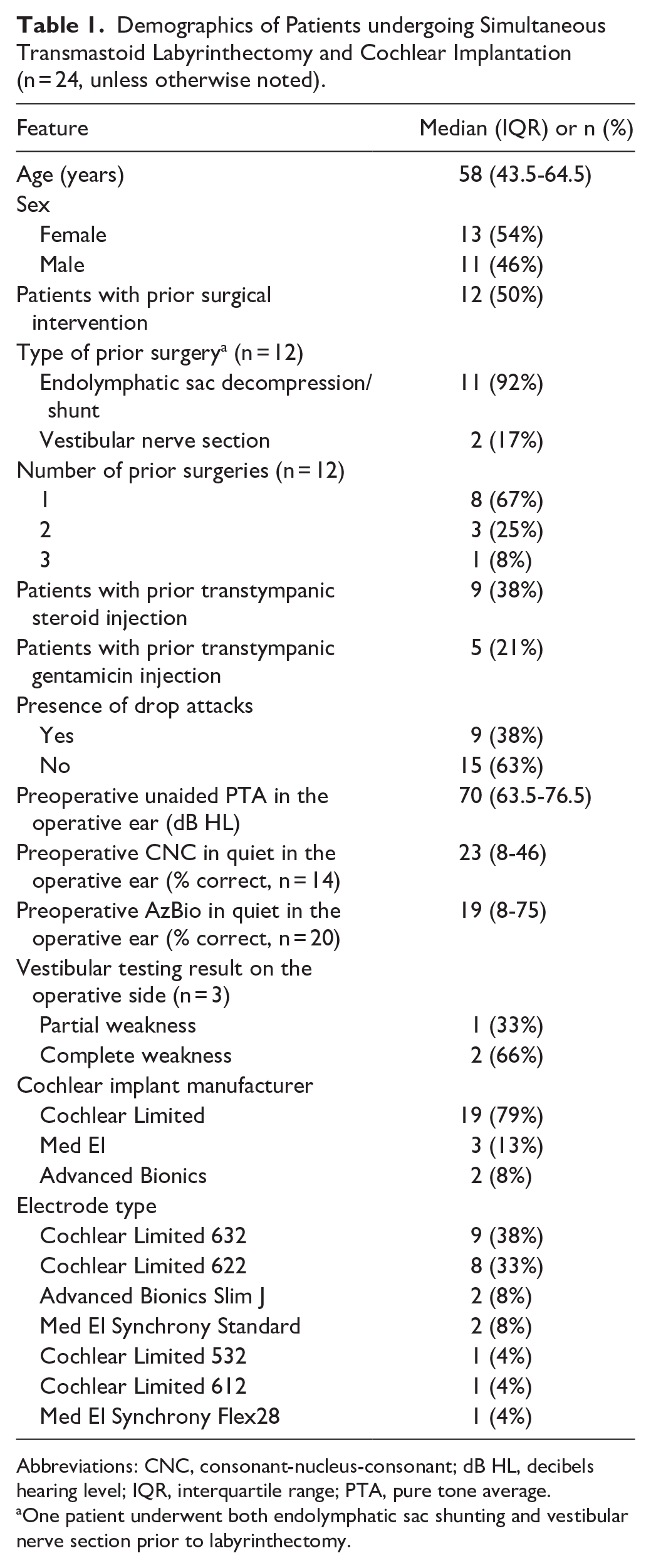
Abbreviations: CNC, consonant-nucleus-consonant; dB HL, decibels hearing level; IQR, interquartile range; PTA, pure tone average.
One patient underwent both endolymphatic sac shunting and vestibular nerve section prior to labyrinthectomy.
The median long-term follow-up of the cohort was 18.4 months (IQR = 7-26). At last evaluation, 23 patients (96%) were noted to have complete resolution of their vertigo, with the remaining patient experiencing only a singular reported episode of vertigo. Thirteen patients (54%) had complete resolution of all associated MD symptoms, and all patients experiencing debilitating drop attacks endorsed complete resolution. The median daily CI usage of those patients with recorded data at last evaluation (n = 11) was 10 hours (IQR = 6.1-13) with no patients being noted to be non-users—including those without daily usage data. Assessing audiometric outcomes in the implanted ear in patients with follow-up ≥6 months (median follow-up 16.8 months [IQR = 13-22.5]), patients had improved CNC in quiet (36% vs 40%, n = 9) and AzBio in quiet (40% vs 62%, n = 13) comparing pre- and postoperative testing, but neither achieved statistical significance (P = .76 and .15, respectively). However, when compared to a score of 0% on pre-operative testing as would otherwise be present after labyrinthectomy without a CI, both CNC and AzBio scores were significantly improved (P < .001). These results are summarized in Table 2. Sound localization data were available for 5 patients (21%) at a median of 9.8 months (IQR = 6.7-14.6) from surgery. When tested with the CI on, the median score in identifying the noise was 32% (IQR = 22%-56%) with a median degree error of 27.9 (IQR = 15.8-38.0) versus a median score of 20% (IQR = 14%-42%) with a median degree error of 43.8 (IQR = 21.9-73.5) with the CI off. Lastly, pre- and postoperative THI data were available for 5 patients (21%) with the most recent evaluation being a median of 12.8 months (IQR = 11.4-14.3) from surgery. Preoperatively, the median THI score was 64 (IQR = 25-81) compared to a postoperative median score of 14 (0-23) with the CI turned on at the last available assessment.
Audiometric Outcomes of the Implanted Ear ≥6 months after Simultaneous Labyrinthectomy and Cochlear Implantation.
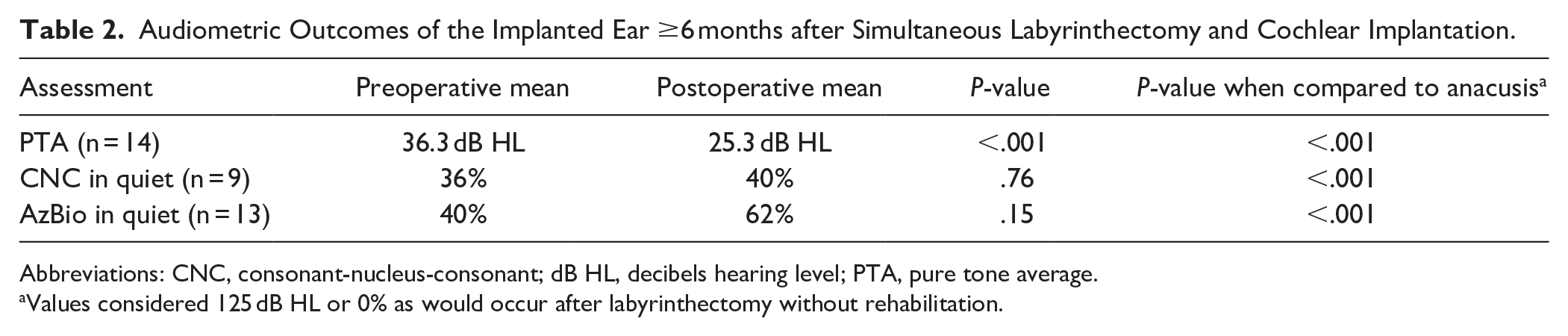
Abbreviations: CNC, consonant-nucleus-consonant; dB HL, decibels hearing level; PTA, pure tone average.
Values considered 125 dB HL or 0% as would occur after labyrinthectomy without rehabilitation.
Discussion
MD is a condition that can lead to debilitating vertigo and progressive hearing loss despite consistent care and effort from patient and provider alike. Management is focused on control of vestibular dysfunction, and it seeks to strike a balance between maintaining function and control of vertigo, with most providers managing this disease in a stepwise fashion. Acknowledging this balance,6 -8 labyrinthectomy is viewed by most as a last-resort procedure to curb severe vestibular dysfunction in MD given that it sacrifices remaining ipsilateral balance and hearing function. However, aural rehabilitation through CI placement has the potential to fundamentally change this paradigm through re-establishment of functional binaural hearing.
The present study represents one of the largest contemporary cohorts to date of patients that underwent simultaneous labyrinthectomy and CI insertion. All patients did well, with limited hospitalization (median discharge on postoperative day 1 [IQR = 1-2]) after the procedure and no substantial immediate complications. One patient (4%) experienced delayed incomplete facial nerve weakness, potentially secondary to viral reactivation or inflammation, but this patient experienced a return to baseline HB grade I function during follow-up. Two patients (8%) had malpositioning of their implants, and 1 patient (4%) had a delayed infection necessitating device removal over a year removed from primary surgery. Of note, one of the patients with a malpositioned implant was found to have a tip fold-over despite having a straight electrode, highlighting the importance of a post-insertion X-ray or device testing algorithm. These events do not appear to be related to the combination of labyrinthectomy and CI placement procedures, but, at present, one cannot exclude potential altered anatomy in MD or more extensive surgery being the cause of these observed complications.
Long-term, these patients had excellent control of their vertigo, with most patients (96%) experiencing complete relief from this symptom. Complete resolution of MD symptoms was noted in over 50% of patients as well, with continued non-specific imbalance being observed in most of the patients that did not experience this relief. This point underlines the commonality of additional comorbid dizziness conditions with MD. 23 THI scores were also found to be improved when considering pre- and postoperative values. Although formal statistical analysis could not be performed given a limited number of patients with available data, this showcases the potential improvement of non-vertiginous symptoms in MD patients after this intervention. Prior literature on labyrinthectomy has primarily dealt with resolution of vertigo and drop attacks rather than other symptoms such as tinnitus, as highlighted in the AAO-HNS clinical practice guideline. 4 Further study on the potential benefits of complete MD symptomatic resolution after combined labyrinthectomy and CI compared to labyrinthectomy on its own is warranted. Furthermore, this excellent disease control is paired with objective audiometric improvement. The observed values may be modest in their improvement and do not achieve a statistically significant threshold, but this could be reflective of the good hearing of some patients prior to surgery (Tables 1 and 2). Importantly, one must additionally consider that rather than the standard pre- and postoperative comparison of testing, a more appropriate comparison may be to anacusis, which these patients would otherwise have without implantation. As noted in Table 2, the results were significantly different when analyzed in this manner. In effect, any amount of rehabilitation provided by a CI is better than one would otherwise have after this procedure. Lastly, although few patients performed sound localization testing, there was improvement when tested with the CI on versus off in both percent correct and degree error. Further studies of such testing could show that this intervention does provide effective binaural input for these patients, even if single ear auditory rehabilitation is more limited; however, more formal statistical analysis could not be pursued in the present study given these data limitations precluding further evaluation of this concept.
To date, limited studies have reported on this management strategy. A retrospective study by Sykopetrites et al 17 represents one of the largest studies to date consisting of 22 patients. These patients experienced improvement in both PTA and speech discrimination scores, with only the former achieving statistical significance—although the specific open-set speech test was not reported. Furthermore, good vestibulopathy control was reported with most patients (67%) experiencing resolution of vertigo symptoms, which interestingly is lower than what is reported in the present report and could represent differences in patient selection as well as surgical technique. Also of note, localization assessment after implantation was not performed in this cohort, which is a critical limitation when compared to our study. A meta-analysis from Selleck et al 19 that identified 14 patients provides additional data supporting this practice while also acknowledging the paucity of reported cases in the literature. Statistically significant improvements were noted in aided audiometric testing, including CNC word scores in quiet, with a higher reported improvement being noted in CNC testing when compared to the present cohort (23% vs 4%). This finding could be due to lower preoperative CNC scores in this meta-analysis, which was reported to be 18%. Interestingly, there was also noted to be improvement in sound localization with the device in this prior piece, but this was not statistically significant when comparing the CI on versus CI off conditions. Given variability in the literature and limited available cases, assessment of vertigo control could not be reliably determined in the Selleck et al 17 study. An additional meta-analysis by Villavisanis et al 18 provides an overview of all MD patients undergoing CI placement, noting improved audiometric outcomes and vertigo control after implantation even without labyrinthectomy; however, they notably combine all patients in their analysis, including any patient with MD that underwent CI placement no matter their treatment history, potentially confounding the results and precluding direct comparison to the present work. Similar positive audiometric and vertigo control results have further been noted in prior smaller case series as well.12 -16 Acknowledging the limitations of the current work, the authors view it as working in concert with these prior publications to further augment our understanding of this treatment strategy, showcasing its ability to provide disease control while providing some rehabilitative potential with limited hearing downtime.
Management of MD through simultaneous transmastoid labyrinthectomy and CI insertion has potential to be a paradigm-shifting therapeutic option for debilitated patients. In part due its destructive nature, other less efficacious therapies are recommended initially for vertigo control 4 ; however, there remains a portion of patients who remain symptomatic despite more conservative treatments. Now, instead of only pursuing labyrinthectomy in cases when a patient is profoundly deaf, the threshold for considering this treatment could be lowered when combined with CI placement, instead being pursued when patients cross the non-functional threshold which is typically associated with open-set speech testing <50%. Another valid consideration is the potential for bilateral MD, which can happen in a fraction of patients, 24 leading to bilateral non-functional hearing. One could argue that this is yet another reason to strongly pursue aural rehabilitation through implantation if a patient elects to undergo labyrinthectomy for disease control. However, considering the limited presented retrospective data and the modest audiometric improvement observed here, it is evident that further study is warranted prior to wholesale implementation of this strategy.
Another salient point to consider within this treatment paradigm is insurance coverage. Despite being well-supported in the literature, SSD at large remains unsupported by various insurance carriers, including the Centers for Medicare and Medicaid Services (CMS), which precludes some medically eligible patients from undergoing implantation. This same situation is common within the MD population, and this serves as a major barrier to widespread implementation of this practice. For instance, CMS patients were not included in this study unless they qualified through standard bilateral criteria, additional secondary insurance was provided, or their device was furnished through research support. Notably, this support from the aforementioned companies permitted more patients to receive a CI at the same time as labyrinthectomy than may have otherwise been possible, with 5 patients (21%) receiving implants courtesy of the device manufacturers. The remaining patients received their implant after insurance approval, but financial barriers and insurance hurdles were nonetheless common in the present study. It is the authors’ practice to seek approval through standard means in all patients and proceed with peer-to-peer meetings if required. If denial occurs and labyrinthectomy is still desired, CI placement can occur in a delayed fashion, acknowledging that cochlear ossification is possible. Placement of a dummy electrode at the time of initial labyrinthectomy could circumvent this issue.
Limitations in the present study include its retrospective nature, which prevents certain assessments from being collected, such as quality-of-life measures. Vestibular evaluation within the cohort was limited in part due to this not being recommended in the AAO-HNS clinical practice guideline 4 as well as the majority of patients undergoing this testing well before labyrinthectomy if it was performed. Furthermore, vertigo control was assessed via patient report rather than more objective criteria. Future prospective studies could ameliorate these issues. Also pertaining to this issue is the potential for variable follow-up. Although last recorded appointments noted good disease control and improved audiometric outcomes, the possibility of worsening disease status or implant function being missed due to less follow-up is possible. It is also possible that the reported outcomes, including audiometric results, could be affected by current undetected or later overt non-use of the implant. An additional consideration within the present study is the implant type. In part due to the retrospective nature of the study as well as the support from certain manufacturers, there was an uneven distribution of electrode types. It is possible that longer electrodes allow better performance in these patients, but the limited number of patients with such electrodes in this cohort precludes further analysis. Lastly, despite the volume of patients and resources available at the authors’ primary institution, the number of patients who have undergone simultaneous labyrinthectomy and CI insertion remains limited. This small cohort size could bias the results or not capture a potential complication of this procedure. Some of the reported analyses, such as the audiometric outcomes, localization testing, and THI results, are also affected by this low cohort size, which restricts more substantial analysis or conclusion, and, again, could introduce bias into the results through loss to follow-up as well as limit generalizability of these results to the overall MD population. Future evaluations of larger cohorts are underway to thoroughly assess this management strategy.
Conclusion
Simultaneous transmastoid labyrinthectomy and CI placement has the potential to be a safe, efficacious procedure that provides excellent vertigo control and can rehabilitate binaural hearing in patients with refractory MD. Taken together with the literature to date, this potentially paradigm shifting management strategy may be considered in patients who otherwise would not be eligible for more definitive vestibular control therapies, but further study is warranted prior to wholesale implementation.
Footnotes
Author’s Note
This study was presented as an oral presentation at the American Neurotology Society Annual Meeting 2024 (Chicago, IL).
Data Availability
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ACM—Research funding from Cochlear Americas. On Board of Directors and is CMO for Otologic Technologies. OFA—Ownership interest in Advanced Cochlear Diagnostics, royalties from Advanced Bionics Inc., advisory board membership with Advanced Bionics Inc. and MED-EL Corporation, and research funding from Cochlear Americas.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research support was provided by Advanced Bionics Inc. and Cochlear Americas Corporation for a portion of the presented cohort.
Institutional Review Board Approval
The Ohio State University IRB Protocol #2023H0353.