
Abstract
Objectives:
Tracheobronchial foreign body (TFB) extraction in premature neonates poses unique challenges due to their delicate respiratory system, making the TBF extraction a critical and high-stakes intervention. TFBs in this patient population are mostly iatrogenic. There are only a few reports in the literature describing the management of TFBs in premature neonates. To the best of our knowledge, this represents the first report using a flexible choledochoscope for TFB extraction.
Methods:
A retrospective chart review was conducted on a case of a preterm infant who underwent successful extraction of a tracheobronchial foreign body.
Results:
A premature neonate born at 25 weeks 2/7 days gestation with a birth weight of 780 g was intubated after delivery. Following extubation to non-invasive ventilation, a control chest radiograph revealed atelectasis of the right lower lobe and a TFB of tubular structure measuring 20 mm × 1.5 mm in the right main bronchus. Diagnostic flexible bronchoscopy was performed and extraction with graspers via rigid bronchoscope was attempted but failed. Subsequently, a bedside procedure in the Neonatal intensive care unit (NICU) was performed using a 7.5 Fr flexible choledochoscope through the endotracheal tube (ETT). TFB was successfully extracted with graspers and upon extraction, it was confirmed to be the distal 2 cm segment of the closed-circuit endotracheal suction system. The infant made full recovery.
Conclusion:
We report a method that provides a safe means of TFB extraction with a successful outcome. The insights gathered from this review are intended to contribute valuable knowledge that can enhance the management of TFBs in preterm infants.
Keywords
Introduction
Tracheobronchial foreign body (TFB) extraction in preterm infants poses unique challenges due to their delicate respiratory system and the potential for rapid cardiorespiratory deterioration, making the TBF extraction a critical and high-stakes intervention. The use of standard bronchoscopy equipment may be inadequate in ensuring safe and effective extraction. 1 There are only a few reports in the literature describing the management of TFBs in preterm infants.
We present a case of an extremely low birth weight infant that underwent a successful TFB extraction via flexible choledochoscope. To the best of our knowledge, this is the first report of a TFB extraction via flexible choledochoscope.
This report aims to underscore the necessity for alternative approaches in addressing TFB extraction within the delicate population of preterm infants. Furthermore, this report seeks to comprehensively review the literature and to search for techniques that have demonstrated successful outcomes. The insights gathered from this review are intended to contribute valuable knowledge that can enhance the management of TFBs in preterm infants.
Case Presentation
An extremely low birth weight female neonate was born at 25 weeks 2/7 days gestation with a birth weight of 780 g. The pregnancy was complicated by preterm labor and chorioamnionitis. Apgar scores were 4, 6, and 7 at 1, 5, and 10 minutes, respectively. The baby was hypotonic, apneic, and bradycardic after delivery, necessitating intubation, surfactant administration, and invasive mechanical ventilation. After the initial recovery and extubation to non-invasive ventilation, the subsequent clinical course was complicated by sepsis and multiple surgeries for necrotizing enterocolitis. A control chest radiograph was performed after the first laparotomy at the 45th day of life and revealed atelectasis of the right lower lobe and a TFB of tubular structure measuring 20 mm × 1.5 mm in the right main bronchus (Figure 1). At this point, the baby weighed 1250 g. A multidisciplinary team comprising otorhinolaryngologists, pediatric surgeons, neonatologists, and anesthesiologists, gathered in the operating room less than 24 hours later. Under general anesthesia, flexible bronchoscopy was performed through the endotracheal tube (ETT) with an inner diameter of 3.5 mm, revealing a tubular TFB, 2 mm in diameter, in the right main bronchus. The ETT was then removed, a 3.5 mm rigid bronchoscope was inserted into the trachea, and extraction with graspers was attempted but failed. Three days later, another attempt was made. This time a bedside procedure in the NICU was performed under sedation with ketamine and midazolam. During the procedure, the infant was ventilated through a Superset micro mount connector 15M-15F (Intersurgical LTD, Berkshire, UK; REF: 3535000), connected to a 3.5 mm ETT (Figure 2a). A 7.5 Fr flexible choledochoscope was introduced through the opening at the top of the connector. After the TFB was visualized in the opening of the right main bronchus, it was successfully extracted with graspers. Upon extraction, it was confirmed to be the distal end of the closed circuit endotracheal suction system with Lock, size 6F (Avanos Medical Sales, Alpharetta, USA; REF: 196-5; Figure 2b). The infant remained stable throughout the procedure and was successfully extubated 12 hours after. The follow-up chest X-ray showed resolution of the right lung atelectasis. She was discharged home at 55 weeks corrected age achieving full enteral intake, complete respiratory recovery without the need for supplemental oxygen. Subsequent follow-up assessments at the age of 2.5 years revealed normal neurocognitive development and the child sustained respiratory well-being.
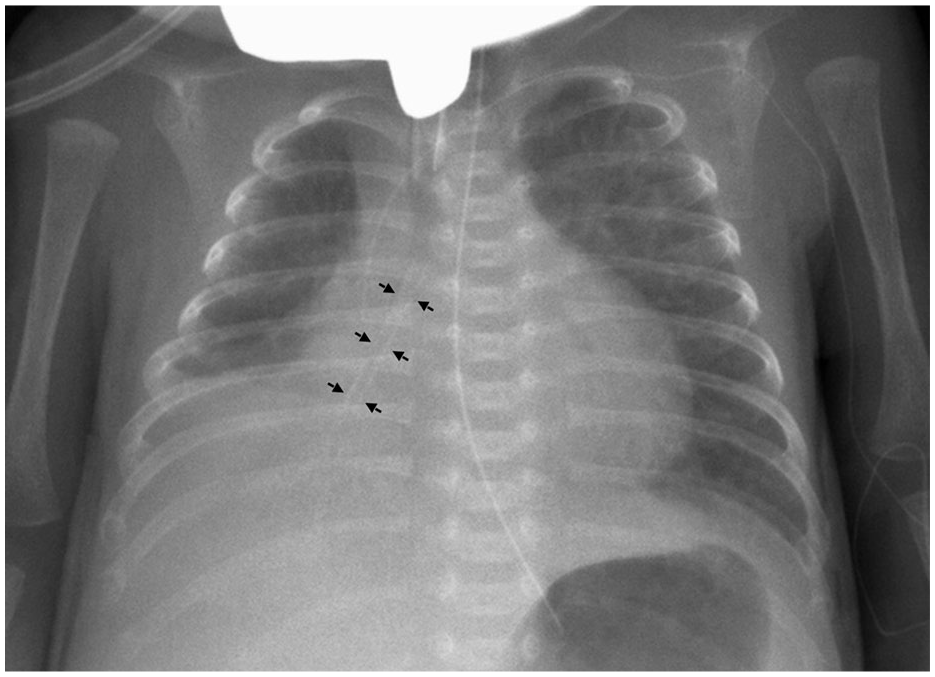
Chest X-ray showing right lower lobe consolidation and tubular foreign body (arrows) in the right main bronchus.
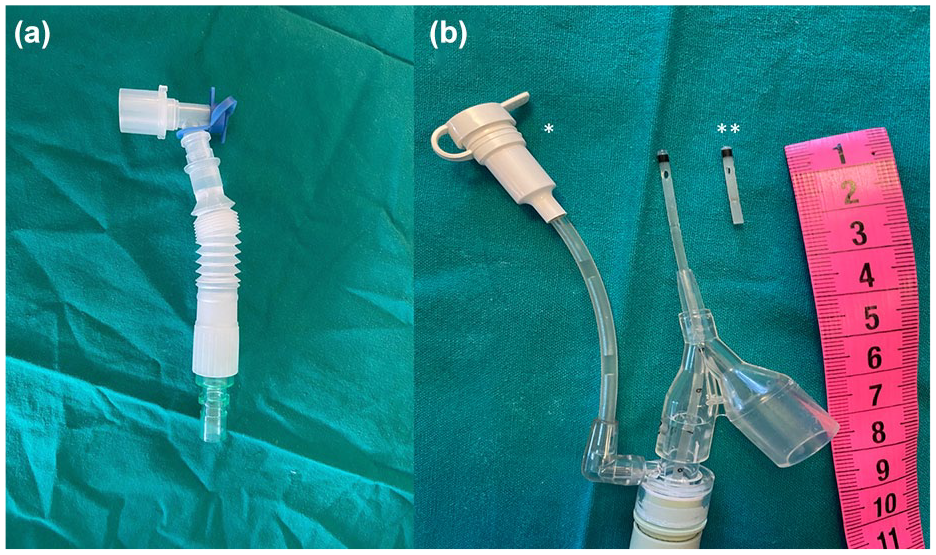
(a) Superset micro mount connector 15M-15F (Intersurgical LTD, Berkshire, UK; REF: 3535000). (b) Closed circuit endotracheal suction system (*); Extracted distal end of the closed endotracheal suction catheter, 2 cm in length (**).
Discussion
TFBs are rare in preterm infants, and there are a limited number of case reports. In this patient population, TFBs are mostly iatrogenic; suction catheter fragments and intubation stylet fragments have been reported. 2 Management presents a challenge that should be addressed by a multidisciplinary approach and thorough preoperative planning. 3
Standard bronchoscopy equipment is inapplicable because of the small airway diameter in preterm infants; therefore, other instruments may be selected for their small sizes. 1 Preterm infants are underdeveloped and at increased risk of respiratory failure; therefore, TFB extraction in this patient population may cause serious morbidity and mortality.4,5 Review of literature revealed a few anecdotal reports of TFB extraction in preterm infants using diverse tools and techniques.
Rigid bronchoscopy is the modality of choice in extracting TFBs in pediatric population, as it offers adequate visualization while oxygen and inhalational agents may be administered through the side arms. 6 Rahbin et al 7 described removing a TFB using alligator forceps via rigid bronchoscope. Another report by Jasinovic et al 2 described a TFB extraction with flexible urological cup forceps that was passed through a rigid bronchoscope. Similarly, Wei et al 8 reported extracting a TFB with a flexible ureteral biopsy cup forceps via rigid bronchoscope.
Although flexible bronchoscopy has been used primarily for diagnosis, during the past decade it has established its role in treatment. Flexible bronchoscopy is recommended as an additional tool for small and peripheral TFBs. Its growing popularity is due to wider availability and simpler handling when reaching peripheral TFBs. 6 Kho et al 5 reported removing a TFB with a urological basket that was passed through the suction port of a flexible bronchoscope.
Another approach was described by Viswanathan et al 9 , in which the TFB was removed under direct visualization using optical forceps. Similarly, Leonard et al 4 presented a case in which the airway was examined with a rigid and flexible bronchoscope, and eventually the TFB was removed using optical forceps. Chiou et al 10 described the use of optical forceps under telescopic vision to extract a sheared fragment of the stylet sheath. Although in previous cases laryngospasm was not reported, it remains the most significant potential risk of the technique. 2
Hodge et al 3 presented an innovative approach using sialoendoscopy forceps via sialoendoscope that was passed through the lumen of the patient’s ETT to extract a TFB. Urology equipment has been used in some cases of TFB extraction in preterm infants, as it was suitable due to its small diameter. Reed et al 1 described extracting a distal tip of a suction catheter using semi-rigid ureteral graspers via rigid ureteroscope.
It seems that in such rare and challenging clinical scenarios, creativity and multidisciplinary approach are crucial. We opted for a 7.5 Fr flexible choledochoscope provided by pediatric surgeons, as there were no small enough otolaryngology instruments available. In our case, a 7.5 Fr flexible choledochoscope was passed through the 3.5-mm ETT and had the advantage of maintaining continued ventilation, which posed no additional risks to the airway, as preterm infants are prone to rapid desaturation during extubation.
In addition, we would like to emphasize the importance of prevention strategies. Enhanced quality control in airway equipment manufacturing and visual inspection of every instrument or device before insertion and after its withdrawal from the ETT is mandatory.
Conclusion
We report a method that provides a safe means of visualizing and manipulating the TFB, with a successful outcome. This case report demonstrates efficiency in using a flexible choledochoscope, an instrument that was not designed or intended for use in the pediatric airway, but due to its small size it has proved to be a valuable asset.
Footnotes
Data Availability Statement
Data available on request due to privacy/ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patients legal guardian for publication of this case report and any accompanying images.