
Abstract
Objectives:
An association between COVID-19 and olfactory dysfunction has been reported worldwide. It has been recognized that olfactory dysfunction may be the only sign of COVID-19. Reports demonstrate an increase of the nasal calcium levels in the patients with olfactory dysfunction. Disodium orthophosphate is a calcium chelating agent which may be associated with improving olfactory function. The main objective of this study is to investigate the effect of intranasal disodium orthophosphate on reducing the increase of calcium in the mucus of patients with olfactory dysfunction post COVID-19, thereby improving the olfaction process.
Methods:
Fifty-two patients with a history of COVID-19 and olfactory dysfunction persisted more than 6 months were enrolled in prospective randomized blinded double controlled clinical trial. They received a nasal spray containing either 0.9% sodium chloride or 1% disodium orthophosphate. Olfactory function was assessed before treatment and 2 months later using the Sniffin’ Sticks test. Quantitative analysis of calcium level in the nasal secretions was performed using a prepared screen-printed ion-selective electrode.
Results:
Compared to sodium chloride, intranasal disodium orthophosphate resulted in a reduction in nasal calcium concentrations. Clinically, 81% of patients in this group demonstrated improvement in olfactory function, with a shift from anosmia to hyposmia based on TDI score classification.
Conclusions:
Intra-nasal disodium orthophosphate is beneficial in improving olfactory dysfunction post COVID-19.
Introduction
Olfactory dysfunction commonly occurs after a variety of upper respiratory tract infections. The pathogenesis of olfactory dysfunction remains unclear. 1 Recently, an association between COVID-19 and olfactory dysfunction has been reported worldwide. It has been demonstrated that olfactory dysfunction may be the only sign of COVID-19 without presence of other clinical symptoms. There is an urgent need to test possible treatment alternatives for olfactory dysfunction associated with COVID-19 infection.2-4
In recent years, calcium has been shown to play an essential role in the downstream signaling cascades of olfactory receptors, including inhibitory feedback. The inhibitory role of calcium is thought to occur through 2 mechanisms. 5 First, calcium-calmodulin interacts directly with channels controlled by cyclic nucleotides, resulting in decreased sensitivity of the channel to cyclic nucleotides and thus decreased positive current influx. The second mechanism is thought to be related to calcium-dependent phosphorylation and consequent inhibition of adenylyl cyclase, leading to a decrease in intracellular cyclic adenosine monophosphate and thus decreased activation of cyclic nucleotide-gated channels. The latter of these 2 mechanisms may be important for the adaptation of the olfactory response to prolonged stimulus exposure. 6 During COVID-19 infection, inflammation and epithelial disruption in the olfactory cleft may impair calcium regulation, resulting in elevated extracellular calcium concentrations in the nasal mucus. These increased calcium levels are hypothesized to enhance inhibitory feedback on olfactory receptor neurons, contributing to persistent olfactory dysfunction. More specifically, an increase in the mucosal calcium levels may lead to desensitization of the olfactory receptor neurons. So. it is hypothesized that the changes in odor sensitivity caused by small changes in mucosal calcium levels can significantly alter the sensitivity of cyclic nucleotide-gated channels and thus the excitability of receptor neurons in vivo, leading to an improvement in the sense of smell.7-9 Disodium orthophosphate, a calcium chelating agent, has the ability to bind free calcium ions in the nasal mucus and could somehow modulate these inhibitory effects, thereby improving the olfactory function. 10
The main objective of this work is to test the efficacy of disodium orthophosphate in reducing the rise of calcium in the mucus of patients with olfactory dysfunction post COVID-19. This is the first published clinical trial testing disodium orthophosphate as a topical treatment to improve the olfactory dysfunction post COVID-19.
Methods
Study Design
A prospective, randomized, double-blinded, double-controlled clinical trial was conducted. The study was approved by the relevant ethical committee (IRB 00012367-23-01-018). Written informed consent was obtained from all patients prior to their inclusion. Participants were randomly assigned to 1 of 2 groups—sodium chloride or disodium orthophosphate—using unstratified block randomization with a block size of 4. A computerized randomization plan was employed to ensure blinding.
To preserve blinding, both the physicians and patients were unaware of group assignments. The allocation process and the organization of treatment groups were managed by a designated team member who was excluded from direct patient care and did not interact with the patients or the investigators. All protocol details were securely handled to prevent unblinding during the trial.
Sample Size
Recent reports demonstrated that 79.5% of the patients with olfactory dysfunctions post COVID-19 may have complete recovery through the first 2 months. 11 So 300 patients were screened for the eligibility recommendations. Fifty-two patients 28 women and 24 men, participated from January 2023 to August 2023. Complete characterization and examination of the patients were recorded. The study design was shown in Figure 1.
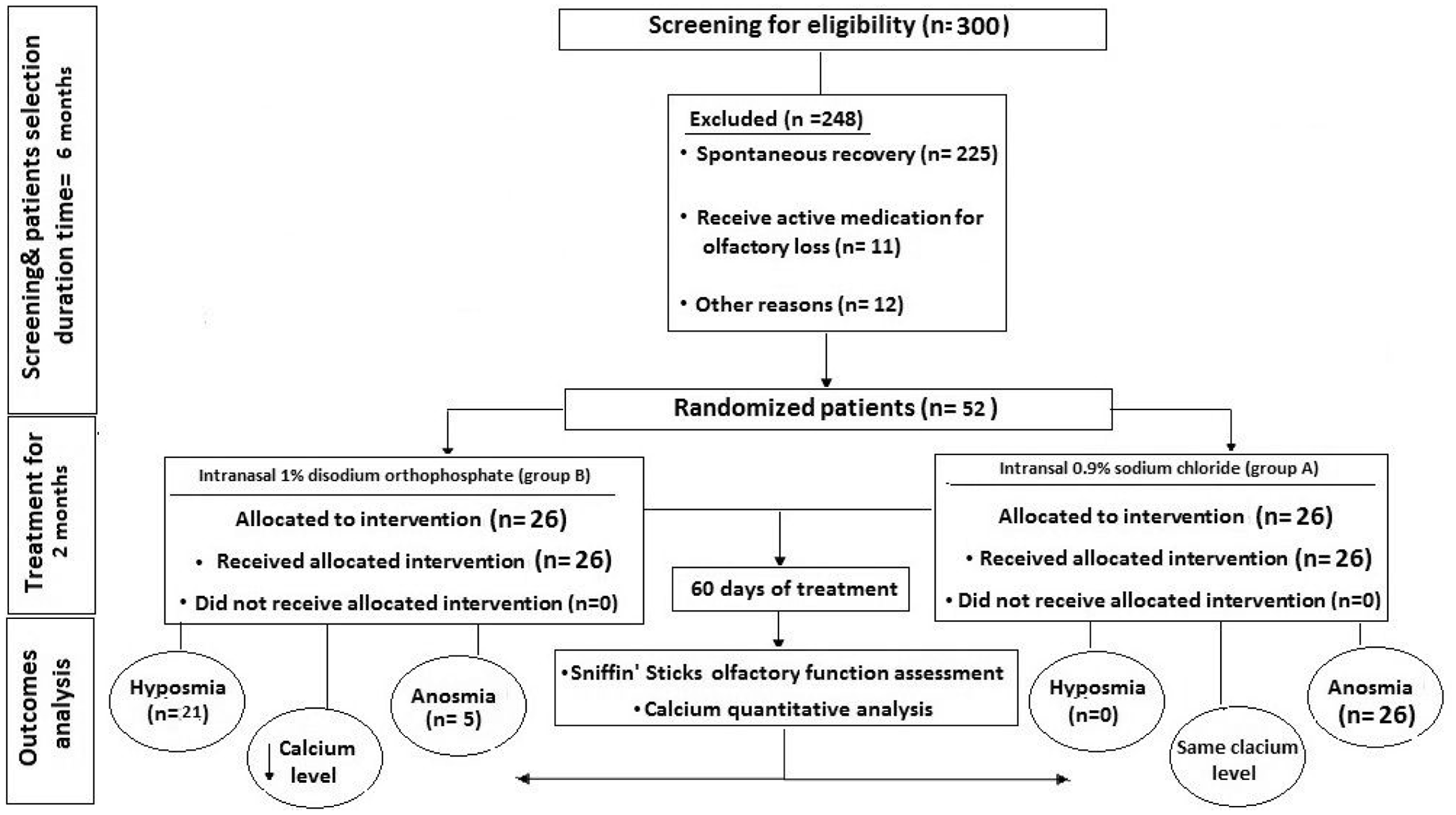
The flow diagram of the proposed study.
Inclusion Criteria
To be enrolled in the current study the patients had to meet the following inclusion criteria: adults with previous COVID-19 infection confirmed by reverse transcription polymerase chain reaction (RT-PCR) in nasopharyngeal swabs, recovery from infection confirmed by at least 2 negative nasopharyngeal swabs, clinically confirmed signs of olfactory dysfunction persisted more than 90 days after SARS-CoV-2 negative testing were included in the study.
Exclusion Criteria
The exclusion criteria included: (1) patients with a history of previous olfactory dysfunction related to trauma or surgery; (2) patients with congenital olfactory loss and neurodegenerative diseases;(3) patients with psychiatric or neurological diseases; (4) patients who had received any active treatment for olfactory dysfunction during the 6 months preceding study enrollment; (5) patients with a history of adverse reactions to sodium salts; (6) pregnancy; and (7) any patient with current participation in other COVID-19 trials.
Treatment Regimen
Patients were divided into 2 groups. The first group was treated with intranasal spray 0.9% sodium chloride (group A). The second group was treated with intranasal spray 1% disodium orthophosphate in borate buffer solution with a pH of 8 (group B). Regarding to FDA, it was determined that disodium orthophosphate is generally recognized as safe chemical compound and the commonly used concentration of phosphoric acid salts may be up to 10%, 12 so 1% disodium orthophosphate was appropriate and safe to be used as topical nasal solution. These formulations were filled into opaque nasal spray bottles to deliver 100 µL of the formulated spray solutions. The bottles were labeled with a specific sealed code that was not accessible to team members involved in the study. They remained sealed unless there was a need to detect secrecy due to adverse effects presented by a participant. Patients received the assigned bottle and instructed to administer 2 sprays for every nostrils 3 times daily for 2 months. To test the precision of the proposed treatment, a control group was included. Participants were instructed on treatment administration during their initial visit and explicitly advised not to engage in any form of structured smell training during the 2-month treatment period. Additionally, questionnaires at each evaluation point documented any additional treatments or interventions. Patients were monitored for side effects throughout the study. In addition, the patients’ nasal secretions were collected before treatment and 2 months later. This was used for quantitative analysis of calcium level in the nasal secretions.
Assessment of the Olfactory Performance
The “Sniffin” Sticks’ test (Burghardt®, Wedel, Germany) is a clinical assessment of olfactory function based on pen-like odor dispensers. 13 It includes 3 tests of olfactory function, odor threshold (T), odor discrimination (D), and odor identification (I). By measuring the 3 tests, the TDI value could be determined.14-16 A TDI score below 16.75 points was considered to represent anosmia, and a TDI score between 16.75 and 30.50 points was considered to represent hyposmia. A TDI score of 30.75 points or more signified normosmia. The patient was considered improved when the TDI value had increased by 6 points. 17
Quantitative Analysis of Calcium Cations of the Nasal Secretions
Patients’ nasal secretions were collected before treatment and 2 months later immediately after sneezing. For this purpose, a small stainless-steel clamp (approximately 10 mm × 5 mm × 2 mm) was clamped on the septum between the nostrils to allow the secretions to drain into a special 1.5-mL tube. 18 Collected nasal secretions were diluted by addition of 2 mL borate buffer solution. Protein layers were denatured by addition of 3 mL acetonitrile. It was evaporated to dryness, and the residues were diluted with borate buffer solution in 10-mL volumetric flasks. Design of the screen-printed calcium cation-selective electrode was done to quantitatively analyze the calcium level of the collected nasal secretion samples before treatment and 2 months later.
Statistical Analysis
All statistical analyses were performed with SPSS v23 statistical software (SPSS, Inc, Chicago, Illinois). Differences in sample size frequencies were tested with Fisher’s exact probability test. In general, results were expressed as mean ± standard deviation. A paired t-test, dependent t-test, was used to compare the means and standard deviations before and after medication within the same group. On the other hand, unpaired t-test, an independent t-test, was used to compare and test the significance of the results of the 2 groups. Statistical significance was assigned when P < .05.
Results
Fifty-two patients who had exhibited signs of an olfactory dysfunction post COVID-19 for more than 6 months were included in this prospective study. The age of the patients ranged from 18 to 51 years. There were 28 women and 24 men. The complete characteristics of the study participants were described in Table 1. Fisher’s exact probability test was used to assess the sample size. No significant difference was found between the sodium chloride control group and the disodium orthophosphate group, as shown in Table 1. Intra-nasal use of disodium orthophosphate had the ability to form a complex and decrease the concentrations of calcium in the nasal secretions of the patients.10,11
Patient’s Characteristics.
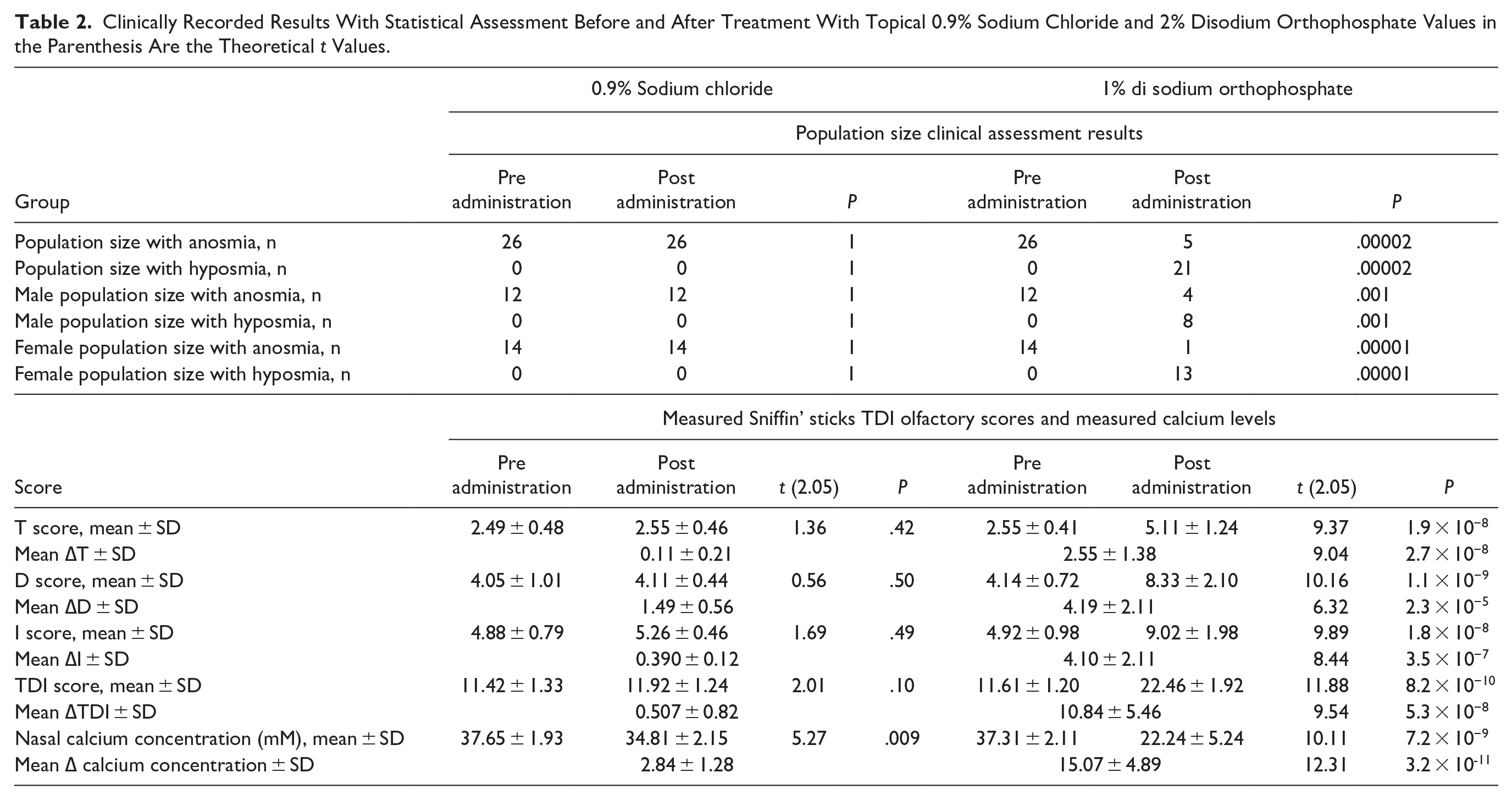
Full monitoring of T, D, I also the TDI values were done. Mean T, D, I, and TDI values before treatment and 2 months later were presented in Table 2. The change of the measured olfactory scores, T, D, I, and TDI, (∆T, ∆D, ∆I, and ∆TDI) following treatment with sodium chloride and disodium orthophosphate, Figure 2, was calculated as following: (the measured score post treatment—the measured score pretreatment). Mean ± SD of ∆T, ∆D, ∆I, and ∆TDI values for sodium chloride and disodium orthophosphate was shown in Table 2. In general, TDI values were compared to the reported reference values for the studied groups. The results of the sodium chloride group revealed no improvement in the measured olfactory scores. In contrast, the disodium orthophosphate group showed a mean increase in TDI scores that exceeded the minimal clinically important difference (MCID) of 6 points, indicating a clinically relevant improvement in olfactory function. Furthermore, the measured olfactory scores of disodium orthophosphate group revealed that 21 patients (81%) showed an improved olfactory function from anosmia to hyposmia and 5 patients (19%) did not show improvement, Table 2. The female scores were higher than male scores, Table 2. This could be due to females more carefully matching the medical counseling and instructions. So, an improvement in the olfactory function was demonstrated after intranasal treatment with disodium orthophosphate.
Clinically Recorded Results With Statistical Assessment Before and After Treatment With Topical 0.9% Sodium Chloride and 2% Disodium Orthophosphate Values in the Parenthesis Are the Theoretical t Values.
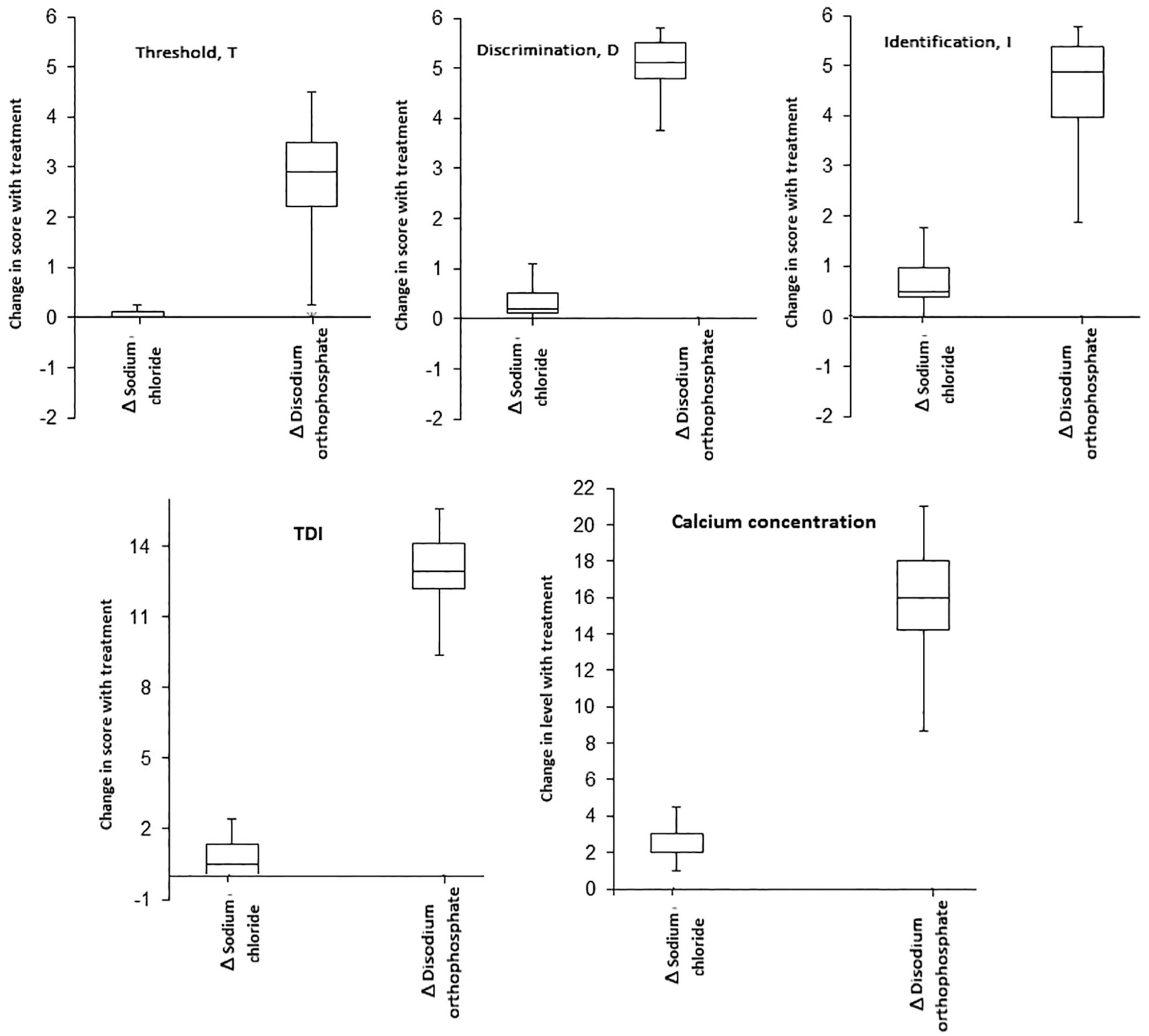
Box and whisker plots showing the change in the measured olfactory scores and the change in calcium concentration levels for group received sodium chloride (Δ sodium chloride) and group received disodium orthophosphate (Δ disodium orthophosphate).
Calcium level in the nasal secretions was quantitatively analyzed using a screen-printed ion-selective electrode. 19 Electromotive force values were recorded over a calcium concentration range of 100 to 0.001 mM to obtain a calibration plot relating the electromotive force values to calcium concentration values. The designed electrode showed a Nernst slope of 28.65 mV/decade with a detection limit of 0.0001 mM in a linear range of 100 to 0.001 mM calcium cation concentration. The calcium level in the collected nasal secretions was successfully analyzed using the prepared electrode. The change of the measured nasal calcium concentration, ∆ calcium concentration, following treatment with sodium chloride and disodium orthophosphate, Figure 2, was calculated. Mean ± SD ∆ calcium concentration was shown in Table 2. The results showed calcium level decrease in only patients received disodium orthophosphate.
Paired t test was provided for statistical testing the means and standard deviations of the measured olfactory scores (T, D, and I) and the measured calcium level values before and after treatment with sodium chloride and disodium orthophosphate. Non-significant difference was observed for the measures of the sodium chloride group except for the measured calcium levels. On the other hand, there was an observed significance for the all measures of the disodium orthophosphate group as indicated by the calculated lower P values, Table 2.
To test whether using intra nasal disodium orthophosphate resulted in statistical significance improvement of the olfactory function in comparison to sodium chloride group, the change in the olfactory scores, ∆T, ∆D, ∆I, and ∆TDI, and the change of the measured nasal calcium concentration, ∆ calcium concentration, of the patients treated with disodium orthophosphate were compared to the corresponding calculated values of sodium chloride group using unpaired t test. Results were shown in Table 2. The significant difference between sodium chloride and disodium orthophosphate groups was indicated by the results obtained. It could be concluded that the results of patients receiving intranasal disodium orthophosphate revealed a significant difference with a relevant clinical improvement in the olfactory function from anosmia to hyposmia.
Disodium orthophosphate was generally well tolerated. Nasal discharge was the commonest side effect seen. However, mild burning sensation in either the nose or throat were also reported. No patients reported experiencing parosmia either at baseline or at any point during the 2-month treatment and follow-up period.
Discussion
Olfactory dysfunction is one of the most common symptoms associated with many cases of coronavirus. Some reports revealed that human strains of coronavirus have been shown to enter the central nervous system via the olfactory neuro epithelium and replicate from the olfactory bulb, affecting olfactory performance.20-23
Many reports have described that an increase in the calcium level in the nasal mucus with negative effects on the olfactory function. During the response to odorants, there is an increase in cyclic adenosine monophosphate and calcium cations. The increase in cyclic adenosine monophosphate is due to activation of adenylate cyclase. The increase in intracellular calcium cations is also due to the influx into the cyclic nucleotide channels.7-9 Subsequently, it is speculated that decreasing the rise of free calcium cations may reduce feedback inhibition and lead to improved receptor response and olfactory function.
The current prospective randomized blinded controlled trial tested intra-nasal administration of disodium orthophosphate for the treatment of olfactory dysfunction post COVID-19. Disodium orthophosphate, a calcium chelating agent, has the ability to bind free calcium ions. 10 The chelation process is mainly influenced by pH and the presence of other competing cations. At pH 8, disodium orthophosphate selectively forms the corresponding complex with calcium even in the presence of sodium, potassium, or magnesium cations. This chemical reaction leads to a decrease in the concentration of calcium in the nasal secretions of patients.
The “Sniffin” Sticks’ test is a useful tool for clinical testing of the chemical senses of the nose. This test is currently used worldwide due to the reliability, reproducibility, and high degree of precision. The “Sniffin” Sticks’ test provides the ability to evaluate olfactory function by testing odor threshold, odor discrimination, and odor identification. This capability makes the test better than other olfactory function assessment tests.14-17 The results of intra-nasal administration of disodium orthophosphate indicated a significant improvement in the olfactory performance, as evidenced by the increase in calculated “Sniffin” Sticks’ test results.
The ion-selective electrode provides an accurate method for quantitative analysis of calcium cations based on the design of a specific screen-printed electrode.24,25 In the proposed work, quantitative analysis of calcium level in the nasal secretions was performed. Using the developed sensor, it was possible to quantify the calcium level before treatment and 2 months later. The results obtained showed a sharp decrease in calcium level in the patients who received intra-nasal disodium orthophosphate. This can be explained by the sequestering effect of disodium orthophosphate for the calcium with subsequent formation of the corresponding complex product. 10 It is worth mentioning that the results indicate a correlation between the reduction of calcium level by disodium orthophosphate and the increase in the calculated odor test results with a subsequent improvement in the olfactory performance.
This study had several limitations. The major limitation of this study is the small sample size, which may lead to an underpowered analysis. A formal power analysis was not conducted prior to enrollment; instead, the sample size was determined based on the availability of eligible patients during the recruitment period. This limitation is acknowledged, and larger, adequately powered studies are needed to confirm the findings. There is a need for additional studies to confirm the association between the changes of the nasal calcium concentration and the olfactory function. Actually, it will be important to extend this study for more studied populations. Furthermore, testing the use of disodium orthophosphate for olfactory dysfunction due to various factors rather than COVID-19 infection should be provided.
Conclusion
In this work, the effect of intranasal disodium orthophosphate to decrease the elevated nasal calcium in the patients with olfactory dysfunction post COVID-19 was demonstrated. Regarding to the measured olfactory scores of disodium orthophosphate group, 81% showed an improved olfactory function and 19% did not exhibit clinical olfaction improvement. After comparison of results from patients who received intranasal disodium orthophosphate to those who received sodium chloride, a statistically significant difference was observed, with the disodium orthophosphate group showing a clinically relevant improvement in olfactory function from anosmia to hyposmia. Based on the results of this study, it could be concluded that there could be an association between the decrease of calcium level in the nasal secretions by the disodium orthophosphate and the increase in the measured olfactory score with a subsequent improvement in the clinical olfactory function.
Footnotes
Acknowledgements
None.
Authors’ Note
Jasmine N. A. Albukhari is also affiliated to Department of Pharmacy, Saudi National Hospital, Makkah, Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Committee of Damietta Faculty of Medicine, Al-Azhar University (IRB 00012367-23-01-018).
Trial Registration
IRB 00012367-23-01-018.