
Abstract
Background:
The role of fine-needle aspiration (FNA) in diagnosing parotid tumors remains debated due to varying accuracy. This study evaluates FNA’s accuracy in diagnosing Warthin’s tumor (WT) and its safety in guiding observational management.
Study design:
Retrospective cohort study.
Setting:
Single institution, Tertiary referral center.
Methods:
Data from 2010 to 2022 including demographics, cytology, pathology, and surgical outcomes were extracted. Accuracy was assessed using sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
Results:
Among 808 patients with parotid tumors, 234 were WTs. Seventy-eight patients underwent surgery with pathology while 156 underwent observation. FNA sensitivity, specificity, PPV, and NPV for WTs were 98.2%, 98.1%, 91.8%, and 99.6% respectively. No observational patients developed clinical signs of malignancy, and the median change in tumor size was 0 cm (range −3.1 to 2.1).
Conclusions:
FNA is highly specific for WT but limited by nondiagnostic results. Observation is a safe approach with minimal risk of growth, malignancy, or infection.
Keywords
Introduction
Warthin tumors (WT) are the second most common benign tumors of the parotid gland, after pleomorphic adenomas, and account for approximately 15% of all parotid tumors.1 -3 Also known as papillary cystadenoma lymphomatosum or adenolymphoma, WTs commonly occur in Caucasian men in their 60s or 70s and typically presents as a painless, slow-growing mass in the inferior tail of the parotid gland. 2 WTs can be firm or fluctuant and may be multicentric (12%-20%) or bilateral (5%-14%).4,5 While the exact origin of Warthin tumors remains unclear, several risk factors have been associated with their development.2,4 Cigarette smoking is the most well-established risk factor, significantly increasing the likelihood of Warthin tumor formation. Additionally, other potential contributing factors include Epstein-Barr virus (EBV) infection, autoimmune diseases, exposure to radiation, and chronic inflammation, all of which may play a role in the pathogenesis of these neoplasms. Warthin tumors are FDG-avid, which makes them easily detectable on PET imaging. As a result, they are frequently found incidentally during the work-up of unrelated malignancies.
Fine needle aspiration (FNA) is a minimally invasive and inexpensive technique used to diagnose nodules and masses arising in the head and neck. 1 With a small bore needle, FNA allows for the preoperative estimation of malignancy, histology, and grade of a lesion. 6 Providing a preoperative pathologic diagnosis, FNAs may be able to dictate the type of treatment and extent of potential resection. 7 Though widely used to obtain cytology results, FNA accuracy varies among operators, pathologists, and tumor type and may lead to sensitivity and specificity rates as low as 52% and 48%. 8
Given that many WTs occur in elderly patients who may prefer to avoid surgery, the diagnostic accuracy of FNA is crucial for guiding management. While reports on FNA sensitivity vary from 72% to 93%, a reliable diagnosis can provide confidence in opting for observation over surgical intervention.9-11 The primary aim of this study was to evaluate the accuracy of FNA in diagnosing WTs. Additionally, we aimed to assess whether FNA results guide appropriate management decisions, particularly in selecting observation over surgical resection, and to describe the natural history of observed WT. We hypothesize that FNA demonstrates high accuracy for WTs due to their distinct cytologic features and that this method is appropriate in facilitating the decision to opt for observational management.
Materials and Methods
After institutional review board approval (IRB # 22-000296), we conducted a 12-year retrospective cohort study of diagnostic accuracy and natural history of observed WTs. Clinical data including demographics, cytology and pathology results, and surgical outcomes were extracted from a departmental clinical parotid tumor registry at a tertiary care referral center queried from 2010 to 2022. Inclusion criteria consisted of patients at least 18 years old who had a WT diagnosis either cytologically on FNA or surgically on permanent pathology. Patients were separated into 2 cohorts: those who had surgery and those who underwent observation only. Among the observation-only cohort, patients were diagnosed by cytology, and oncologic outcomes were reviewed to assess any changes in size of the tumor or malignant development. Among the surgical cohort, FNA accuracy using permanent pathology was calculated.
Accuracy of FNA in diagnosing WT was described using sensitivity (TP/(TP + FN)), specificity, (TN/(TN + FP)), positive predictive value (PPV: TP/(TP + FP)), and negative predictive value (NPV: TN/(TN + FN)). True positives consisted of WTs diagnosed both on FNA and permanent pathology. Patients with paired FNA and permanent pathology results that were not WTs served as the true negatives in this study. False positives consisted of tumors that were diagnosed as WTs on FNA but confirmed not be WT on permanent pathology, while false negatives consisted of tumors that were not diagnosed as WTs on FNA but confirmed to be WTs on permanent pathology.
Statistical analysis was done using an independent t-test. Statistical significance was defined as a P-value below .05.
Results
Among a cohort of 808 parotid tumors, we identified 543 patients with preoperative FNAs, and 234 patients with either a cytologic or histopathologic diagnosis of WT (Figure 1). Of the 234 patients with a cytologic or pathologic diagnosis of WT, 78 patients underwent surgical resection of their tumor with confirmed pathology, and 156 patients underwent observation alone after FNA diagnosis of WT. Another 255 patients were identified with preoperative FNAs and permanent pathology diagnostic of other parotid tumors, and these patients served as true negatives in this study.

Flow chart demonstrating inclusion and exclusion criteria in determining the final study cohort.
Among the surgical group, the average age was 64 years (SD 8.7) and 69% were male. Of the 78 surgical patients with paired FNA and permanent pathology results, 16 had a non-diagnostic FNA (12%). Of the remaining 62 patients, 56 (true positives) had a correct positive FNA diagnosis of WT confirmed on final pathology, 1 (false negative) had a pathologically confirmed WT with an initial FNA diagnosis of squamous cell carcinoma, and 5 (false positives) had a diagnosis of WT on cytology that was changed on permanent pathology to be 4 oncocytomas and 1 mucoepidermoid carcinoma (Table 1). Among the total FNAs obtained, the sensitivity and specificity of FNA in the diagnosis of WTs was thus 98.2% and 98.1%, while positive predictive value and negative predictive value were 91.8% and 99.6%, respectively. Among patients undergoing surgical resection, all 78 patients underwent a superficial parotidectomy. Median length of follow up was 1.4 years (range 0-7.8). Postoperative complications included hematomas (3.8%), seromas (3.8%), sialoceles (2.6%), and wound infections (2.6%). Frey syndrome developed in 1 (1.3%) patient, 2 (2.6%) developed first bite syndrome, and 15 (19%) reported ear numbness. One (1.3%) postoperatively had a visit to the emergency department and 1 (1.3%) had an unplanned return to the operating room for a post-operative hematoma. Seventy-six (97%) patients had a House Brackmann (HB) of I at 1 year follow up, while patients with a HB of II and III occurred in 1 (1.3%) each.
FNA Accuracy of the Surgical Cohort.
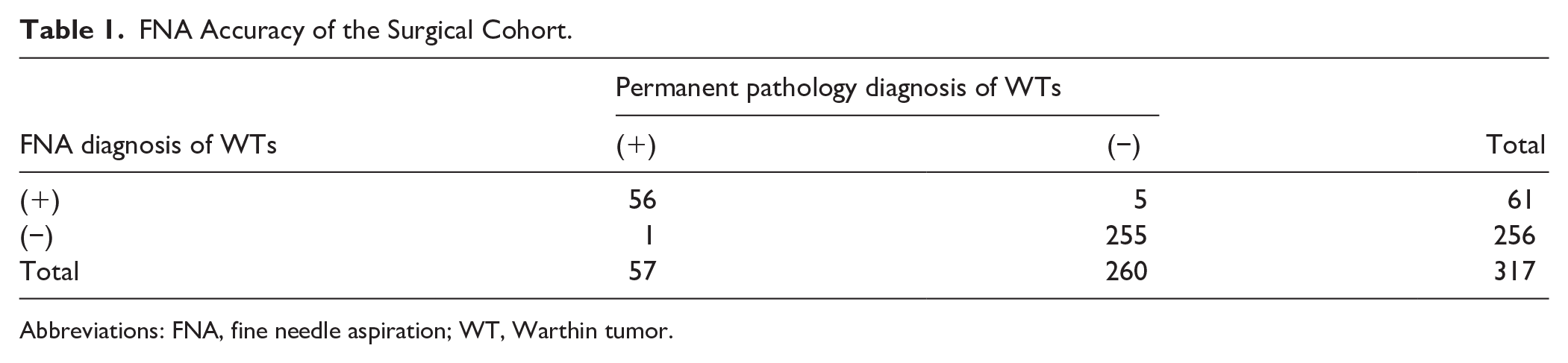
Abbreviations: FNA, fine needle aspiration; WT, Warthin tumor.
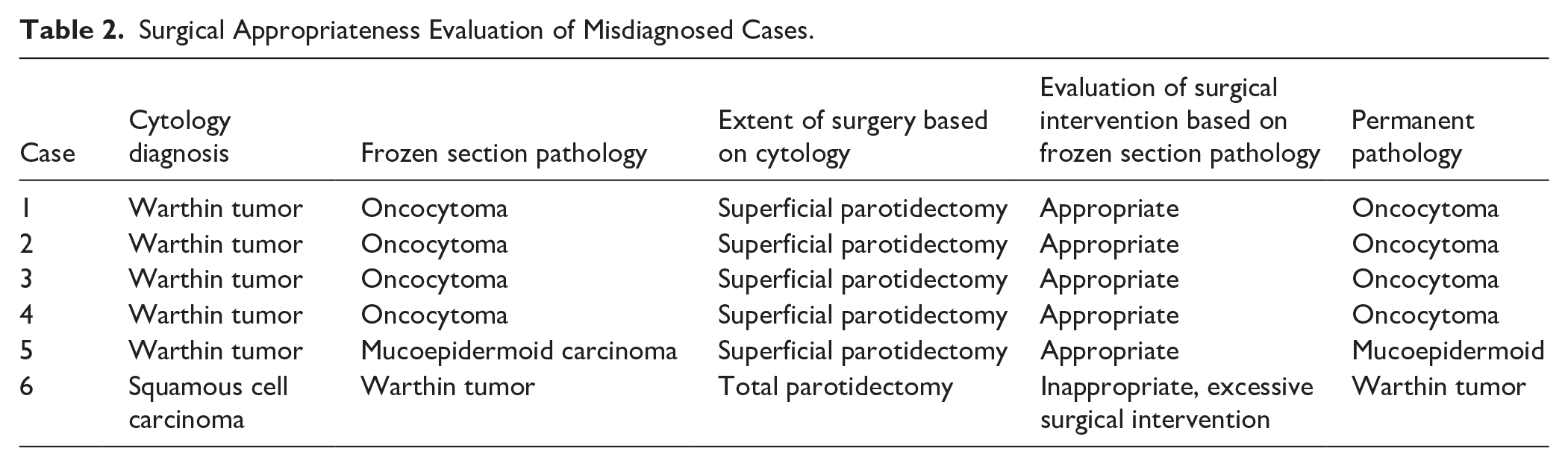
The extent of surgical intervention was determined based on patients’ FNA results and frozen section pathology. Cases with discordant cytology, frozen section, and final pathologic diagnosis are displayed in Table 2. One patient had an FNA that was suggestive of squamous cell carcinoma, but frozen section pathology showed WT, and only a superficial parotidectomy was performed. Final pathology confirmed WT. One patient was diagnosed with low grade mucoepidermoid carcinoma on frozen section who was originally diagnosed as a WT on FNA. A superficial parotidectomy was performed and permanent pathology confirmed the frozen section diagnosis. At 6.2 years of postoperative follow up, there was no indication of recurrence nor development of a parotid malignancy in the surgical group.
Surgical Appropriateness Evaluation of Misdiagnosed Cases.
An observation-only cohort was assessed to investigate the natural history of patients diagnosed with WT who underwent conservative management based off their FNA. Of the 156 patients included in this cohort, the average age was 71 years (SD 10; P-value <.01 compared to the average age of the surgical group) and 62% were male. Median follow up time was 2.4 years (range: 0-12 years) and no patients in this cohort went on to develop clinical signs or symptoms suggesting malignancy. Parotiditis occurred in 2 (1.3%) patients within the time from diagnosis to date of last follow up. In 1 patient, a bacterial infection stemmed from the parotid gland while in another, the infection was localized to their WT. Both patients were treated with antibiotics and their symptoms resolved.
We identified 80 patients in the observational cohort who underwent imaging both around the time of diagnosis via FNA and at their last follow-up. Imaging consisted of head and neck ultrasound (US), computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography CT (PET CT). Median time to last follow up of imaging was 2.5 years (range 0-14). The average change in tumor size was a decrease in 0.25 cm (SD 1.7 cm) per year and a median of 0 cm (range −13.2 to 2.5) per year. Among the 80 patients, there were 58 who had at least 1 year of follow up imaging, with a median time of 3.7 years (range 1-14). In this cohort of 58 patients, the average change in size was 0.3 mm (SD .23 cm) per year and the median 0 cm (range −1.0 to 0.7 cm). The median total change in size among all observed patients was 0 cm (range −3.1 to 2.1 cm).
Discussion
We retrospectively reviewed 234 patients who had been diagnosed with WTs by either cytology or permanent pathology with 78 having undergone surgery and 156 observed. FNA was found to be an accurate and reliable tool in diagnosing WTs with high sensitivity (98.1%) and specificity (98.2%). No patients who were observed went on to develop signs of malignancy or misdiagnosis, suggesting FNA diagnosis of WT is adequate to safely observe patients who are not candidates for surgery or who wish to delay surgery. There were 58 patients who were observed with follow-up imaging at least 1 year after diagnosis, and in this group, growth was minimal with an average growth of 0.3 mm/year suggesting a very indolent course for patients who elect for observation. Notably, there was 100% concordance between frozen section diagnosis and permanent pathology, suggesting frozen section remains a reliable intraoperative diagnostic tool guiding decision making.
WTs are cytologically diagnosed based upon a cellular triad of lymphoid cells, oncocytes, and proteinaceous material.12,13 When all 3 components are available, the diagnosis is easily made. Misdiagnoses occur when the cytologic smear contains less than the 3 components, inexperience of the pathologist, or insufficient cytologic material obtained. The most common tumors misdiagnosed histologically by FNA as WTs are low-grade mucoepidermoid carcinomas and acinic cell carcinomas, both malignant neoplasms.2,12 -14 In a meta-analysis by Fisher and Ronen, 2 among the false positives reported initially as WTs on cytology, 55% were considered malignant. Among our study, there were 6.4% false positives for WT and 1.3% false negatives that were diagnosed as WT after surgery. False positives, patients that were incorrectly diagnosed with WT on FNA, consisted of 4 oncocytomas and a mucoepidermoid carcinoma. There was 1 false negative, which was incorrectly diagnosed as squamous cell carcinoma by FNA and later confirmed to be a WT on permanent pathology. Thus, only 1 of the 5 false positive patients ultimately received a malignant diagnosis, and even in this case, superficial parotidectomy was sufficient treatment for a low grade mucoepidermoid carcinoma. While relying on a FNA for diagnosis for treatment decisions can be a challenge and may require a discussion between the patient and physician, in the case of WT, it appears that reliance on the FNA result can be a safe strategy in surgical counseling when frozen section is not available.
Recent reports on parotid FNA accuracy have been promising, showing FNA sensitivity rates of 93% to 96%.2,15,16 However, there have been some reports of lower accuracy with a meta-analysis from Schmidt et al 17 showing 80% sensitivity. The discrepancy between studies may be due to small study sample sizes and experience of the pathologists and physicians collecting the cytology samples in some of the studies.8,18,19 In most cases, discrepancy between the cytology and histopathology results would not have changed the extent of surgery, as WTs were rarely misdiagnosed as higher-grade tumors on FNA. Fortunately, while the overall accuracy and utility of FNA in the diagnosis of parotid tumors remains under debate, our results suggest that FNA results suggestive of a WT appear to have a higher accuracy, with a sensitivity and specificity of 98.2% and 98.1% in this study.
Because WTs are more common in older patients, progress slowly, and have a low malignant potential, observation only without surgery may be a reasonable option. 16 Malignant transformation of WTs has been reported to be around 0.3% but it is controversial among pathologists whether this represents a true “transformation” from a WT. 13 In our cohort of 156 patients who underwent observation with a long follow-up period, no patient developed a malignancy and there was a low rate of infection. Additionally, we noted a very minimal change in size of the neoplasm throughout the follow up period. Often WTs are diagnosed incidentally as an FDG avid mass during the work-up for other more aggressive malignancies, and expeditious treatment of the underlying malignancy is critical. In older patients with comorbidities, delaying surgery for an extended period of time, or until the lesion starts to affect quality of life, is a valid and safe option supported by the results of this study. The observational cohort in this study coincides with other studies reporting conservative management outcomes of WTs in smaller cohorts. 19 With the reliability and high PPV of FNA, it can be used as a diagnostic tool to confirm WT tumors in patients whose current age or state of health do not permit surgery. Patients who opt for observation should be counseled to follow up for any changes in tumor size, symptoms of pain and discomfort, infections, or any detriment the tumor may pose on their quality of life. Surgical resection of WTs in this cohort was also safe with few complications.
Our study was limited in its retrospective nature and relatively small sample size. Additionally, this study is subject to some selection bias in that data was captured in patients who preferentially sought care. Recall bias may also be present, specifically regarding patient complaints of symptoms between follow up visits. Strengths of this study include inclusion of the largest cohort of observation alone patients with a diagnosis of WT on FNA, which helps contribute to the literature on the natural history of WTs and affirms the safety of this conservative approach in patients with FNAs suggestive of WT. Future directions for this study would be to compare radiologic diagnosis based on classic findings compared to FNA to perhaps negate the need for FNA in the future.
Conclusion
FNA is an accurate and reliable tool in the initial diagnosis of Warthin tumors. In deciding whether a patient should undergo surgical resection or observation, it is reasonable to trust FNA results suggestive of a Warthin tumor. In patients with an FNA diagnosis of Warthin’s, observation is a safe approach with little risk of a missed malignancy or future infection. Patients should seek follow-up for any changes in tumor size or impacts on their quality of life.
Footnotes
Acknowledgements
None.
Ethical Considerations
This study received ethical approval from the Mayo Clinic’s IRB (approval #22-000296) on January 25th, 2022. This is an IRB-approved retrospective study and thus patient consent was waived. This has been also stated in the methodology section of the manuscript.
Consent to Participate
This study received ethical approval from the institution’s IRB (approval #22-000296) on January 25th, 2022. This is an IRB-approved retrospective study and thus patient consent was waived. Patient informed consent was waived as it was deemed by the institution’s IRB as impractical to obtain.
Consent for Publication
Not applicable.
Author Contributions
HB contributed to the conceptualization, investigation, methodology, investigation, formal analysis, writing original draft, and writing – review & editing; HA contributed to the conceptualization, data curation, investigation, supervision, and writing – review & editing;; KS contributed to the investigation, conceptualization and writing – reviewing & editing; LY contributed to the investigation, conceptualization and writing – reviewing & editing; KT LY contributed to the investigation, conceptualization and writing – reviewing & editing; KVA contributed to the investigation, conceptualization and writing – reviewing & editing; EM contributed to the acquisition of data, validation and resources, supervision, writing – reviewing & editing; DP contributed to the conceptualization, data curation, validation, investigation, writing – review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated during and/or analyzed during the current study are not publicly available due to sensitive content but are available from the corresponding author on reasonable request.