
Abstract
Objectives:
Olfactory dysfunction (OD) is a common symptom of SARS-CoV-2 infection. This study aimed to determine the prevalence and clinical characteristics of OD, evaluate its recovery trajectory, and identify predictors of its onset and persistence.
Methods:
We conducted a prospective cohort study of 3477 participants recruited through an online questionnaire between December 1 and 31, 2022. Follow-up surveys were conducted over a 12-week period ending on March 31, 2023.
Results:
Among 3010 eligible participants aged 14 to 40 years, 373 (12.39%) reported new-onset OD following COVID-19 infection. Multivariable logistic regression identified older age, a history of sinusitis or nasal polyps, prior nasal surgery, and symptoms including fatigue, rhinorrhea, dyspnea, ageusia, and pruritus as independent risk factors for OD. Conversely, fever and arthralgia were negatively associated with OD. The cumulative spontaneous recovery rates were 43.70%, 23.86%, 11.26%, 8.04%, 5.63%, and 1.88% at weeks 1, 2, 3, 4, 8, and 12, respectively. No demographic or clinical variables were significantly associated with recovery time.
Conclusions:
COVID-19 related OD occurred in 12.39% of young and middle-aged individuals in China. Several demographic and clinical factors were predictive of OD, although none were associated with recovery duration. Most patients experienced spontaneous resolution within the first month of symptom onset.
Introduction
Infection of the nasal epithelium by SARS-CoV-2 in patients with COVID-19 may lead to olfactory dysfunction (OD). 1 Although many upper respiratory viruses can cause OD, SARS-CoV-2-related OD appears to be more severe than that caused by other viruses 2 and can significantly impair patients’ quality of life. Given the increasing number of individuals affected by OD and its possible association with neurological impairment in COVID-19 patients, SARS-CoV-2-induced OD warrants significant clinical attention.3,4
OD is one of the most common symptoms of COVID-19; however, its reported prevalence varies widely across different regions.5 -7 Butowt et al. 8 reported that the prevalence of OD in COVID-19 patients was 22.4% in East Asian countries versus 48.4% in Western countries, likely due to differences in viral variants and study populations. Epidemiological studies suggest that the Omicron variant is associated with the lowest prevalence of OD, followed by the Delta and Alpha variants.5,9 -12 However, some studies have reported a reduction in symptom severity rather than prevalence. 13 Other contributing factors may include patient age and disease severity. Older age has been associated with a lower prevalence of OD,14 -17 and several studies suggest that OD occurs more frequently in mild COVID-19 cases.18 -20 However, since most studies relied on self-reported olfactory assessments, these results may be subject to reporting bias.
Following the lifting of lockdown measures in China in December 2022, COVID-19 cases surged, marking a new phase of the pandemic in the country. Although previous studies have primarily focused on older or severely ill patients, data on COVID-19-related OD in younger and middle-aged populations remain limited. The first 4 weeks following SARS-CoV-2 infection are typically defined as the acute phase. 21 During this phase, most patients with OD recover either partially or completely.22,23 This study aimed to determine the prevalence of COVID-19-related OD among young and middle-aged patients in China and to characterize its clinical presentation. Additionally, we investigate the proportion of patients experiencing persistent OD. We also analyzed risk factors associated with OD in this population to inform effective management strategies. Finally, we assessed the early recovery rate of OD to help determine the optimal timing for referral to tertiary care for further evaluation and treatment.
Material and Methods
Study Population
We conducted a prospective cohort study involving young and middle-aged Chinese patients with COVID-19. A total of 3477 voluntary participants were recruited from a random sample of the general population between December 1 and 31, 2022. All participants were first-time COVID-19 cases diagnosed during this period. Patients who developed OD after infection were followed from December 1, 2022 to March 31, 2023. Follow-up data were collected at 6 time points: 1, 2, 3, 4, 8, and 12 weeks after enrollment.
Informed consent was obtained prior to participation, with parental consent required for individuals aged 14 to 18 years. Data were collected via structured questionnaires at multiple time points within the first 12 weeks after SARS-CoV-2 infection. All surveys were administered online without requiring in-person hospital visits. Collected information included demographics (age, sex, weight, height, and BMI), medical history (smoking, prior nasal, or neurosurgical procedures), and comorbidities (hypertension, diabetes, coronary artery disease, sinusitis/nasal polyps, rhinitis, and allergic conditions such as asthma). Clinical symptoms included respiratory (fatigue, cough, sore throat), gastrointestinal (loss of appetite, nausea, vomiting), musculoskeletal (myalgia, arthralgia), and neurological symptoms (headache, dizziness, confusion). Cardiovascular and dermatological manifestations were also documented. Objective olfactory testing was not performed; instead, self-reported OD was assessed by asking participants, “Have you noticed any loss of smell?” COVID-19 diagnosis was confirmed by either self-administered antigen tests or RT-PCR performed in community or hospital settings. All individuals with a confirmed positive result, regardless of symptom presence, were included. Inclusion criteria included confirmed COVID-19 infection in patients aged 14 to 40 years. Participants were stratified into 2 groups based on olfactory function: those with normal olfaction and those with OD. Individuals with a history of OD prior to COVID-19 infection were excluded from the study. Follow-up questionnaires gathered information on demographics, medical history, comorbidities, OD recovery time, and treatments. The study workflow is illustrated in Figure 1.
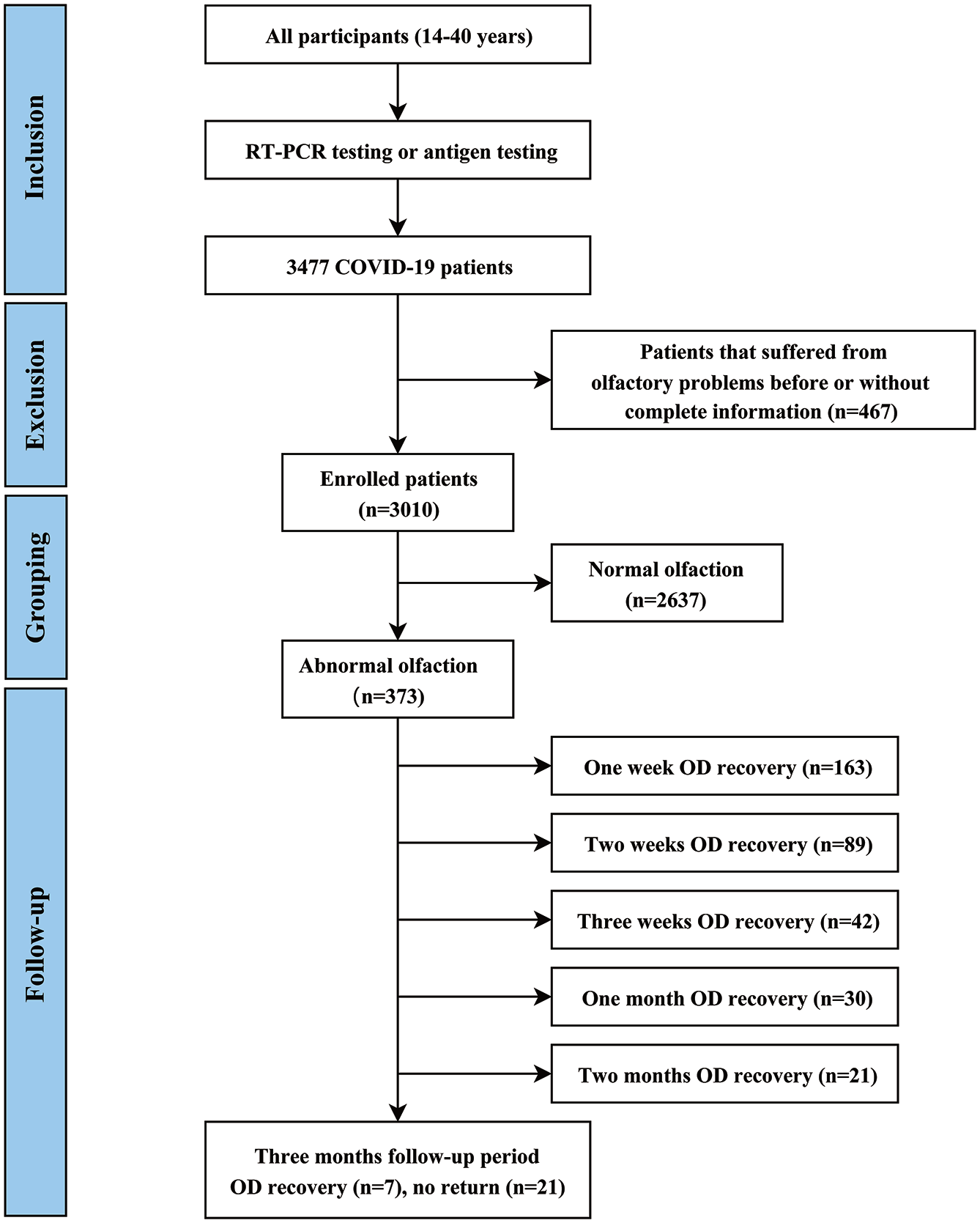
Study workflow diagram. Participants aged 14 to 40 years were enrolled. The flowchart shows inclusion and exclusion criteria, and OD recovery status during the 3-month follow-up.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics 26, GraphPad Prism 9, and Origin 2022. Results are presented as percentages or means ± standard deviations (SD). Statistical significance was defined as P < .05. Baseline characteristics, comorbidities, and symptoms between patients with and without OD were compared using logistic regression analysis. Associations between variables and OD incidence were assessed using odds ratios (OR). Among participants with OD, hazard ratios (HR) and corresponding 95% confidence intervals (CI) were calculated. A receiver operating characteristic (ROC) curve was constructed to evaluate the predictive performance of combined clinical factors. Additionally, Kaplan–Meier analysis was used to assess the timing of OD recovery.
Results
Baseline Characteristics
A total of 3477 participants aged 14 to 40 years completed the assessment, with 3010 included in the final analysis. None had a prior history of SARS-CoV-2 infection. Among them, 373 individuals (12.39%) reported developing OD following their initial SARS-CoV-2 infection. Among the 3010 patients (mean age, 18.59 ± 1.75 years), 40.0% (n = 1204) were male and 60.0% (n = 1806) were female. Females were more likely to report OD (69.17% [n = 258] in the OD group vs 58.70% (n = 1048) in the normal olfaction group, P < .001). The mean age was 18.54 ± 1.53 years in the normal olfaction group and 18.99 ± 2.84 years in the OD group (P = .003). Patients with a history of nasal surgery were significantly more likely to develop OD (2.41% vs .72%, P = .001), while variables such as weight, height, BMI, smoking history, and prior neurosurgical procedures showed no significant association. Table 1 summarizes the demographic characteristics and medical histories of the study participants.
Comparison of Baseline Characteristics Between COVID-19 Patients With and Without OD.
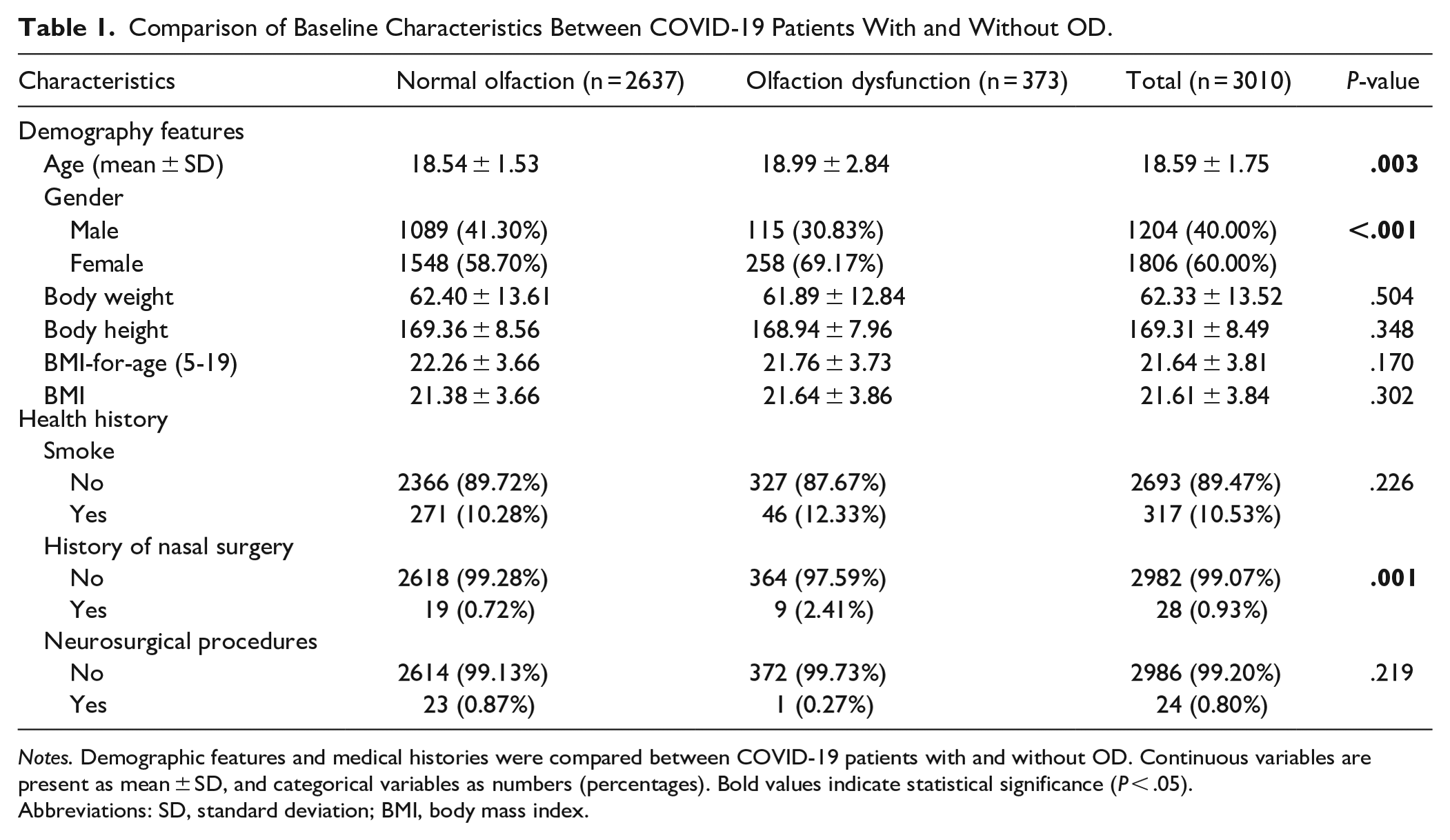
Notes. Demographic features and medical histories were compared between COVID-19 patients with and without OD. Continuous variables are present as mean ± SD, and categorical variables as numbers (percentages). Bold values indicate statistical significance (P < .05).
Abbreviations: SD, standard deviation; BMI, body mass index.
Comorbidities and Symptoms in Patients With and Without OD
We further compared comorbidities and symptom profiles between the OD and normal olfaction groups. Patients with a history of rhinological or allergic conditions—such as sinusitis, nasal polyps, allergic rhinitis, or asthma—were more likely to develop OD following COVID-19 infection. None reported prior OD. Patients who reported additional symptoms—such as typical respiratory, gastrointestinal, musculoskeletal, neurological, cardiovascular, or dermatological symptoms—were more likely to experience OD (Table 2).
Comparison of Comorbidities and Symptoms Between COVID-19 Patients With and Without OD.
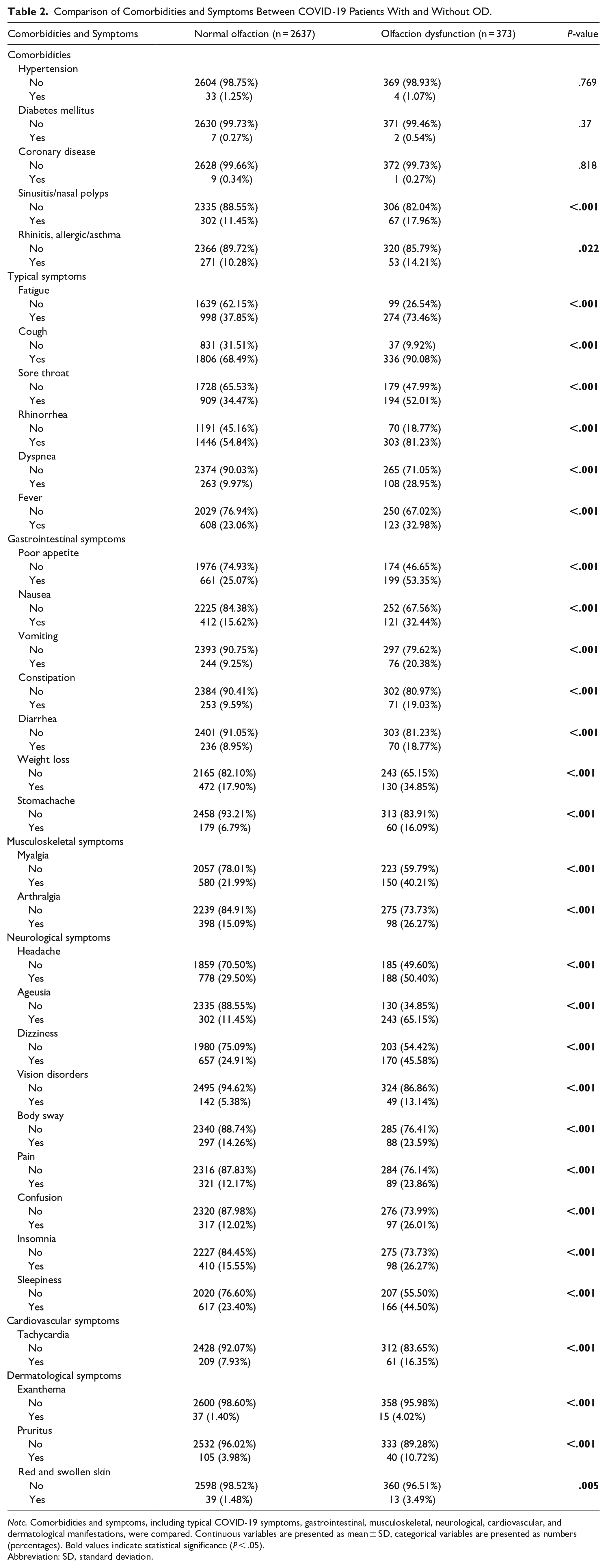
Note. Comorbidities and symptoms, including typical COVID-19 symptoms, gastrointestinal, musculoskeletal, neurological, cardiovascular, and dermatological manifestations, were compared. Continuous variables are presented as mean ± SD, categorical variables are presented as numbers (percentages). Bold values indicate statistical significance (P < .05).
Abbreviation: SD, standard deviation.
The Relationship Between Patients’ Characteristics and OD
Univariable logistic regression showed that older age (95% CI: 1.068-1.185, P < .001), female sex (1.250-1.992, P < .001), pre-existing nasal conditions such as sinusitis and nasal polyps (1.266-2.263, P < 0.001), and a history of nasal surgery (1.530-7.587, P = .003) were significantly associated with self-reported OD, all with 95% confidence intervals. In addition, all clinical symptoms included in the questionnaire were significantly associated with the presence of self-reported OD (Table S1).
Multivariable logistic regression was conducted using variables that were significant in the univariable analyses to identify independent predictors of OD (Figure 2A, Table S1). Independent predictors of OD included older age (1.014-1.152, P = .017), sinusitis or nasal polyps (1.018-2.105, P = .040), a history of nasal surgery (1.095-7.881, P = .032), fatigue (1.439-2.815, P < .001), rhinorrhea (1.201-2.363, P = .003), dyspnea (1.119-2.286, P = .010), ageusia (8.656-15.456, P < .001), and pruritus (1.099-3.410, P = 0.022). In contrast, fever (0.298-0.652, P < .001) and arthralgia (0.430-0.995, P = .047) were negatively associated. The area under the ROC curve (AUC) was 0.840 (0.816-0.863), indicating that the combined model had excellent discriminatory power in identifying patients with OD (Table S2). The corresponding ROC curve is shown in Figure 2B.
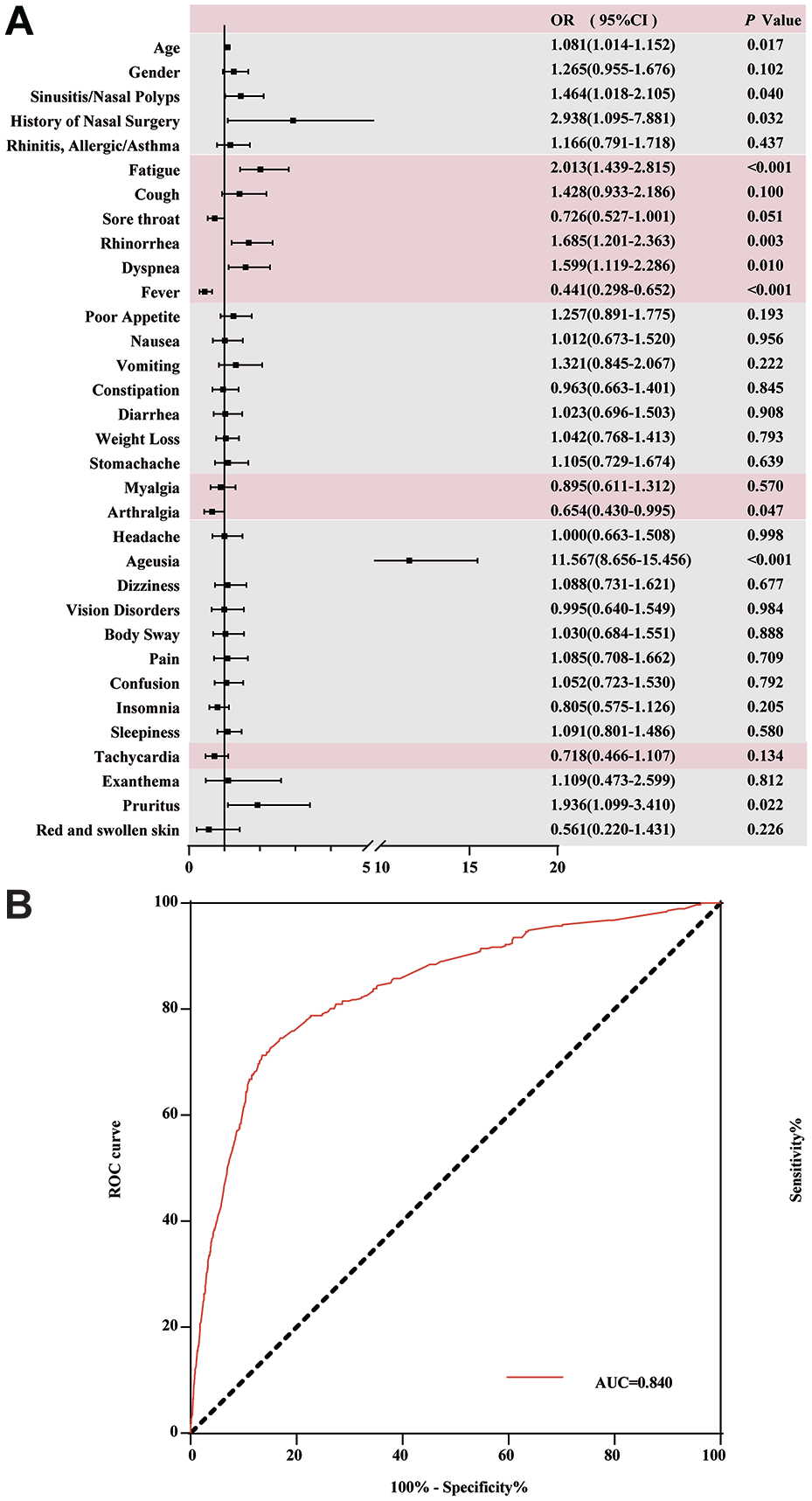
Significant baseline characteristics, comorbidities, and symptoms associated with OD. (A) Forest plot showing the association between OD and clinical variables. (B) ROC shows the predictive performance of combined clinical factors. The shaded area between the red and black lines represents the AUC (0.840; 95% CI: 0.816-0.863).
Recovery of Olfactory Dysfunction Over Time
During the 3-month follow-up, 352 of the 373 participants with OD (94.40%) recovered spontaneously without receiving any medication or medical intervention for OD. The spontaneous recovery rates among the 373 participants were 43.7%, 23.9%, 11.3%, 8.0%, 5.6%, and 1.9% at 1, 2, 3 weeks, 1, 2, and 3 months, respectively (Figure 3A). Despite the high recovery rate, 5.63% (n = 21) of patients continued to experience OD symptoms at the final follow-up.
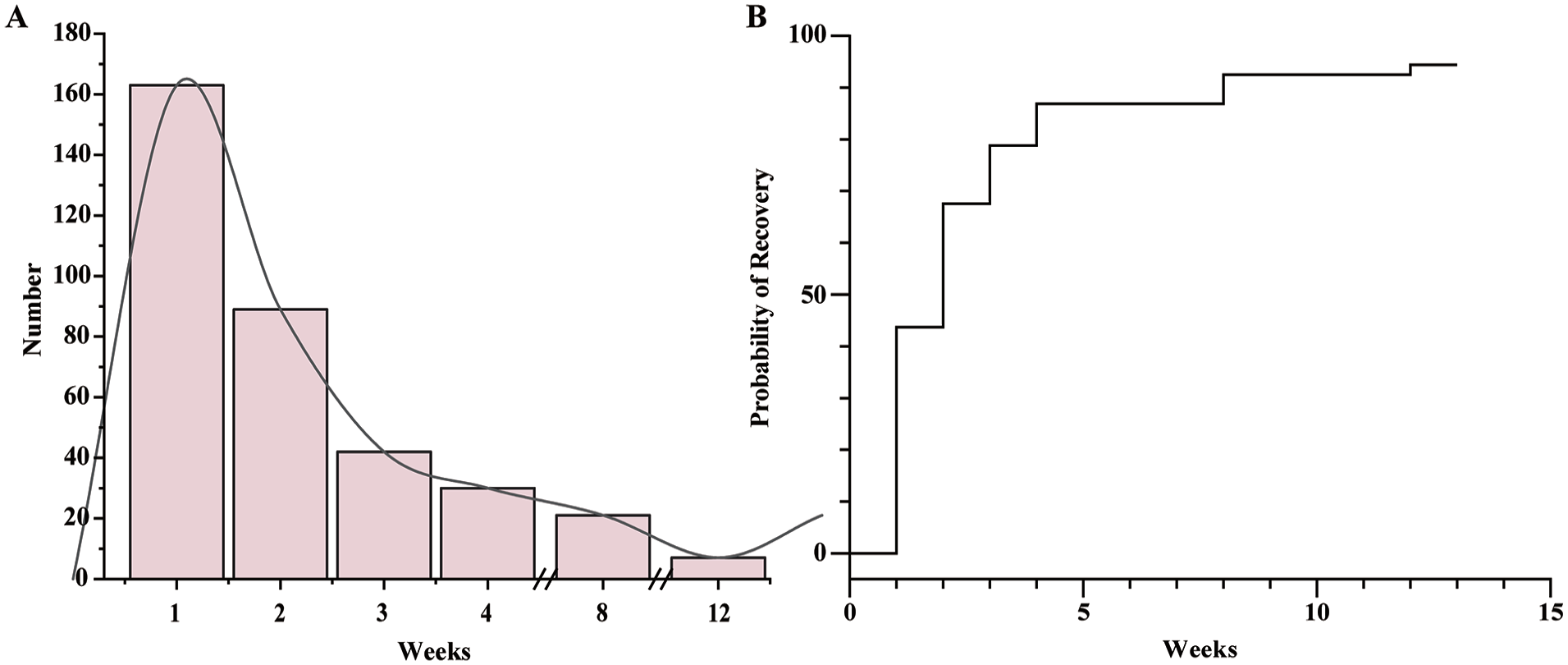
Time to complete recovery from OD. (A) Distribution of recovery times for OD. (B) Kaplan–Meier curve illustrating the pattern of OD recovery over time.
Kaplan–Meier analysis demonstrated a rapid recovery of OD within the first month, followed by a plateau in the recovery trend between the second and third months (Figure 3B).
Cox univariate analysis revealed no significant association between OD recovery and demographic characteristics, medical history, or comorbid conditions (Table S3).
Discussion
Further research on OD following SARS-CoV-2 infection is urgently needed, particularly in populations with predominantly mild symptoms during the post-reopening phase in China. This large prospective cohort study aimed to determine the prevalence and recovery rate of COVID-19-related OD. We also investigated the associations between clinical factors and the onset or resolution of OD. All participants were between 14 and 40 years of age and reported no prior history of OD before their COVID-19 infection.
In our study, the prevalence of self-reported OD was 12.39%, which is similar to the 12.5% reported in adolescents aged 10 to 18 years. 14 However, this rate is notably lower than the prevalence observed in adult populations, typically exceeding 20%, and in systematic reviews of pediatric cases, where estimates have reached up to 49%, depending on study design and population characteristics.16,17 Several factors may account for this discrepancy. First, our study primarily focused on young and middle-aged individuals. While many previous studies have suggested that the frequency of OD decreases with age,15,16,20,24 other studies have reported the opposite. Some studies have reported higher OD prevalence among older COVID-19 patients, 25 whereas those under 40 years show lower rates, 26 consistent with our findings. Second, differences in nationality and ethnicity1,27 may have contributed to the variation in OD prevalence. For example, Soh et al. 27 reported significant disparities in the prevalence of OD among COVID-19 patients of Bangladeshi, Chinese, Indian, and other national backgrounds. Third, the heterogeneity in sample sizes—ranging from fewer than 100 to tens of thousands6,28—may limit comparability. Smaller, less representative samples in some studies may have affected the reliability and generalizability of their findings. Fourth, the absence of objective olfactory assessments in our study may have contributed to the observed differences, particularly given the well-documented discrepancies between psychophysical testing and self-reported olfactory function. 29 Lastly, the rapidly spreading Omicron variant was the predominant strain in China during our study period,30,31 whereas most previous studies focused on earlier variants, such as Delta and Alpha.
In this study, we also found that female patients were more likely to experience OD, a finding consistent with several previous studies.17,22,29,31,32 For example, Awwad et al. 33 suggested that sex-related differences in inflammatory responses, as well as women’s heightened sensitivity to subtle sensory changes, may contribute to this observation.
Due to the relatively young age of the cohort, comorbidities such as hypertension, diabetes, and coronary artery disease were uncommon. For example, hypertension, diabetes mellitus, and coronary artery disease were infrequent. Nevertheless, previous studies have established that both diabetes mellitus and hypertension are associated with a higher risk of OD. 33 In our study, a history of sinusitis or nasal polyps, as well as allergic rhinitis or asthma, was identified as a risk factor for OD. This contrasts with previous research, which found no significant difference in OD prevalence between individuals with and without nasal disease. 34 Moreover, typical symptoms, gastrointestinal, musculoskeletal, neurological, cardiovascular, and dermatological manifestations were all significantly associated with OD. However, smoking history was not associated with OD in our study, which contrasts with the findings of Francesca Galluzzi et al., 35 who reported that COVID-19 patients with current smoking habits and allergic histories were more likely to experience OD. In our study, no significant clinical factors were found to be associated with the duration of OD recovery in this particular population. This may be partially attributable to the demographic characteristics of our cohort, which included only young and middle-aged individuals and excluded older adults, who are typically at greater risk for prolonged OD.
In cases of typical post-viral anosmia, more than 50% of patients experience permanent loss of smell. 36 However, 86.86% of OD cases recovered within 1 month, with recovery rates plateauing thereafter. A similar finding was reported by Parente-Arias et al., 37 who observed that nearly 80% of COVID-19 patients with OD achieved complete recovery within the first month. Another study similarly reported that 75% of individuals with OD experienced improvement in olfactory function within 1 to 4 weeks. 38 In cases of short-term OD following COVID-19, damage to the olfactory epithelium may be repaired through the activation of horizontal basal stem cells. In contrast, long-term OD may result from more complex mechanisms, including prolonged inflammation as well as both cell-autonomous and non-cell-autonomous processes. 39
It is widely accepted that COVID-19 symptoms lasting between 4 and 12 weeks are classified as persistent symptoms. 21 Systematic reviews have shown that the majority of patients recover olfactory function within 30 days. 40 Therefore, if OD persists beyond 4 weeks, referral to a tertiary care center is recommended for further evaluation and management. Moreover, COVID-19-related OD lasting more than 3 months should be considered clinically significant and warrant comprehensive evaluation by specialists, including otolaryngologists and neurologists.
Several limitations should be acknowledged. First, all data in this study were obtained through subjective self-reports, which may introduce unmeasured confounding. Additionally, since the study was conducted online, the lack of objective assessments—such as imaging or psychophysical testing—may have further contributed to bias. Second, it remains unclear whether the 5.63% of patients with OD at the final follow-up will develop persistent dysfunction, emphasizing the need for longer-term follow-up in future research. Third, although several factors—such as age and prior nasal surgery—reached statistical significance, the effect sizes were small (eg, only a .5-year age difference and a 1.7% difference in nasal surgery), limiting their clinical relevance. Thus, future studies with larger effect sizes or more robust clinical endpoints are needed to validate these findings. Finally, although our three-month follow-up captured the majority of recovery cases, future research should incorporate longer follow-up durations to better characterize risk factors for persistent OD and gain a more comprehensive understanding of the recovery trajectory.
Conclusion
We conducted a large-scale prospective study among young and middle-aged Chinese individuals with confirmed COVID-19. The prevalence of OD in this cohort was 12.39%. Independent risk factors for OD included older age, female sex, a history of nasal diseases or nasal surgery, and specific COVID-19-related symptoms such as fatigue, rhinorrhea, dyspnea, fever, arthralgia, ageusia, and pruritus. A combination of these clinical and demographic factors demonstrated good predictive value for the development of OD following SARS-CoV-2 infection. Importantly, most patients experienced spontaneous recovery within a short timeframe, and no significant associations were observed between baseline characteristics and recovery time. These findings underscore the distinct clinical profile of OD in younger populations and highlight the importance of age and symptom presentation in predicting and managing COVID-19-related OD.
Supplemental Material
sj-docx-1-aor-10.1177_00034894251363776 – Supplemental material for The Prevalence of Olfactory Dysfunction and Its Recovery in Chinese Young and Middle-Aged Group COVID-19 Patients
Supplemental material, sj-docx-1-aor-10.1177_00034894251363776 for The Prevalence of Olfactory Dysfunction and Its Recovery in Chinese Young and Middle-Aged Group COVID-19 Patients by Chunhao Li, Tianjiao Jiang, Jinfeng Luo, Yanyi Tu, Hongzhi Ji, Yuzhu Wan, Liang Yu and Li Shi in Annals of Otology, Rhinology & Laryngology
Footnotes
Author Note
Chunhao Li is now affiliated with Peking Union Medical College Hospital, Beijing, China.
Ethical Considerations
The Ethics Committee of Shandong Provincial ENT Hospital reviewed the study protocol and determined that formal ethical approval was not required, as the research involved anonymous, voluntary, and non-interventional data collection via online questionnaires.
Consent to Participate
All participants provided informed consent before participation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Natural Science Foundation of Shandong Province (No. ZR2021MH136) and Administration of Traditional Chinese Medicine of Shandong Province, China (No. Z-2023018).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to privacy restrictions, but de-identified data may be available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.