
Abstract
Objectives:
To evaluate extended outcomes up to 6 years following bipolar-cautery inferior turbinate reduction (ITR) in a large pediatric cohort.
Methods:
Retrospective case series of 326 children (mean age 9.0 ± 4.1 years) who underwent 12-W bipolar-cautery ITR between December 2017 and May 2024 at a single-surgeon tertiary practice. Concurrent procedures were performed in 82% of patients; 59 underwent ITR alone. Parent-reported nasal breathing improvement was assessed at regular intervals up to 6 years. Statistical analyses included Cochran’s Q tests and generalized estimating equations (GEE).
Results:
In the full cohort, nasal breathing improvement rates were: 95.4% at 3 months, 91.7% at 6 months, 90.2% at 1 year, 88.1% at 2 years, and 78.7% at 3 years. Sample sizes decreased beyond 3 years due to follow-up attrition. Cochran’s Q test showed significant changes over time through 3 years (Q = 60.101, P < .001). The ITR-only subgroup showed more marked decline: 98% improvement at 3 months to 69.0% at 3 years (P = .002), compared to more stable rates with concurrent surgery. GEE analysis confirmed significant time effects (P < .001). Compared to ITR alone, concurrent septoplasty (OR 0.39, P = .002) and sinus surgery (OR 0.34, P = .020) were each associated with significantly lower odds of reporting persistent symptoms (i.e., a greater likelihood of improvement). Complications remained low: minor bleeding (4.6%), major bleeding requiring intervention (1.2%), MRSA infection (0.3%), and synechiae (1.5%).
Conclusions:
Bipolar-cautery ITR provides safe, effective symptom improvement with excellent short-term results (>90% at 1 year). However, efficacy declines over time, particularly in ITR-only patients (78.7% overall at 3 years). Concurrent airway procedures may provide more stable outcomes. These findings emphasize the need for long-term follow-up and appropriate patient selection.
Keywords
Introduction
Nasal congestion in pediatric patients commonly results in sleep-disordered breathing, craniofacial abnormalities, and diminished quality of life.1-3 This condition often arises from chronic rhinitis, a persistent nasal inflammation triggered by allergens or irritants, or from anatomical narrowing of the nasal cavity. 4 While the prevalence of narrow nasal anatomy in pediatric patients is not well-defined, it is believed to play a significant role in chronic nasal congestion. 5
Medical therapy, including nasal sprays, antihistamines, and immunotherapy, can fail due to various reasons, including anatomical variances, severity of allergic rhinitis, failure of immunotherapy, inability to deliver nasal medications, and other unaddressed underlying causes. 4 In cases where medical management is ineffective, turbinate reduction surgery can alleviate symptoms by reducing the size of the inferior turbinates, improving airflow. 6 Among various surgical techniques, bipolar cautery turbinate reduction has shown success in adults,7,8 yet its application in pediatric patients is not well-documented. We report our method and extended outcomes up to 6 years postoperatively using 12 W bipolar cautery to reduce turbinate size while preserving mucosal integrity. 8 We describe one of the largest single-surgeon pediatric series to date, focusing on long-term symptomatic outcomes and the influence of concurrent airway surgery.
Methods
With IRB approval and waiver of written consent for chart review (oral consent obtained for phone follow-up; written informed consent obtained for use of nasal endoscopy images), we conducted a retrospective review of children aged 4 to 17 years who underwent bipolar-cautery inferior turbinate reduction (ITR) from December 2017 to May 2024. Patients with neurodevelopmental or chromosomal disorders, prior nasal surgery, craniofacial syndromes, incomplete follow-up, or who declined consent were excluded.
Of 370 patients screened, 44 were excluded (17 for neurodevelopmental/chromosomal disorders, 25 for incomplete follow-up or unreachable, and 2 who declined consent), resulting in a final cohort of 326 patients (see Figure 1). Indications for surgery included persistent nasal congestion due to allergic or non-allergic rhinitis with inferior turbinate hypertrophy unresponsive to medical therapy. Follow-up visits were scheduled at 1 to 3 months, 6 months, 1 year, and annually thereafter. Data on demographics, nasal breathing quality, symptom improvement, postoperative complications, and concurrent surgeries were collected from medical records and supplemented by telephone interviews using a standardized script for patients with missing follow-up. Due to the challenges of long-term pediatric follow-up, data collection was incomplete for many patients at later timepoints.
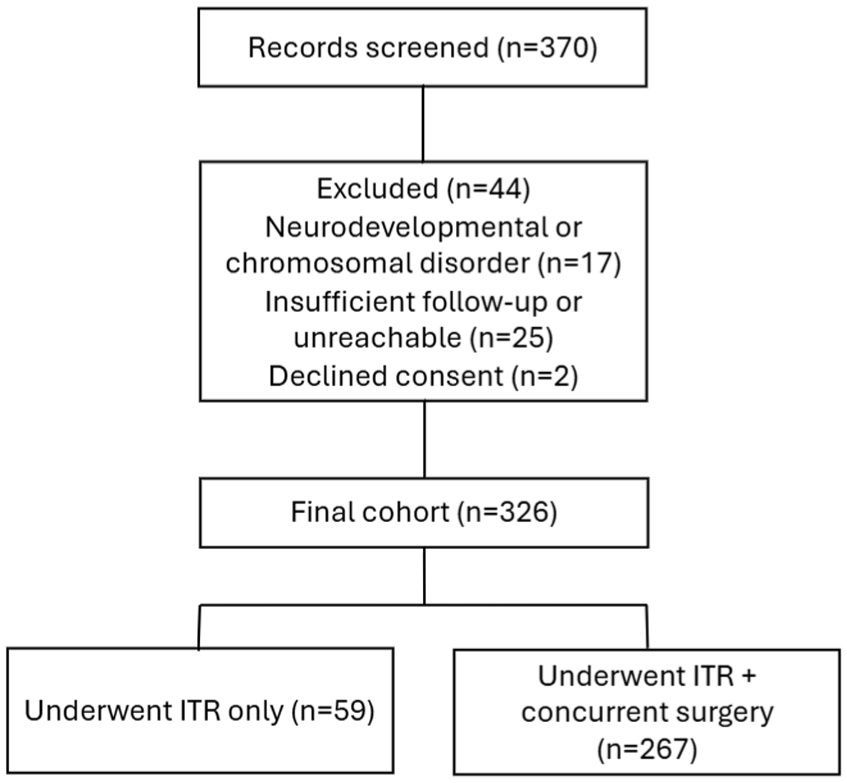
Flow diagram of patient screening and enrollment. A total of 370 patients were screened, of whom 44 were excluded for neurodevelopmental/chromosomal disorders (n = 17), insufficient follow-up or inability to contact (n = 25), or declined consent (n = 2), resulting in a final cohort of 326 patients who underwent inferior turbinate reduction (ITR), with or without concurrent procedures.
Surgical Technique
Patients underwent inferior turbinate reduction using bipolar cautery in an operating room setting. A local anesthetic of lidocaine with 1:100 000 epinephrine was injected into each inferior turbinate with a 25-gauge spinal needle. This solution was dispersed throughout the entire inferior turbinate under endoscopic guidance. The next step was to out-fracture the inferior turbinate bone. Finally, the bipolar prongs were placed on the superior and inferior aspects of the inferior turbinate, and at 12 W, the turbinate was reduced. Cauterization was completed when the mucosa blanched to avoid mucosal disruption. The procedure was repeated on the opposite side in most cases. This controlled reduction targeted the submucosal tissue, reduced turbinate volume while preserving the mucosal lining, and maintained the mucosal covering over the inferior turbinate bone (see Figure 2).
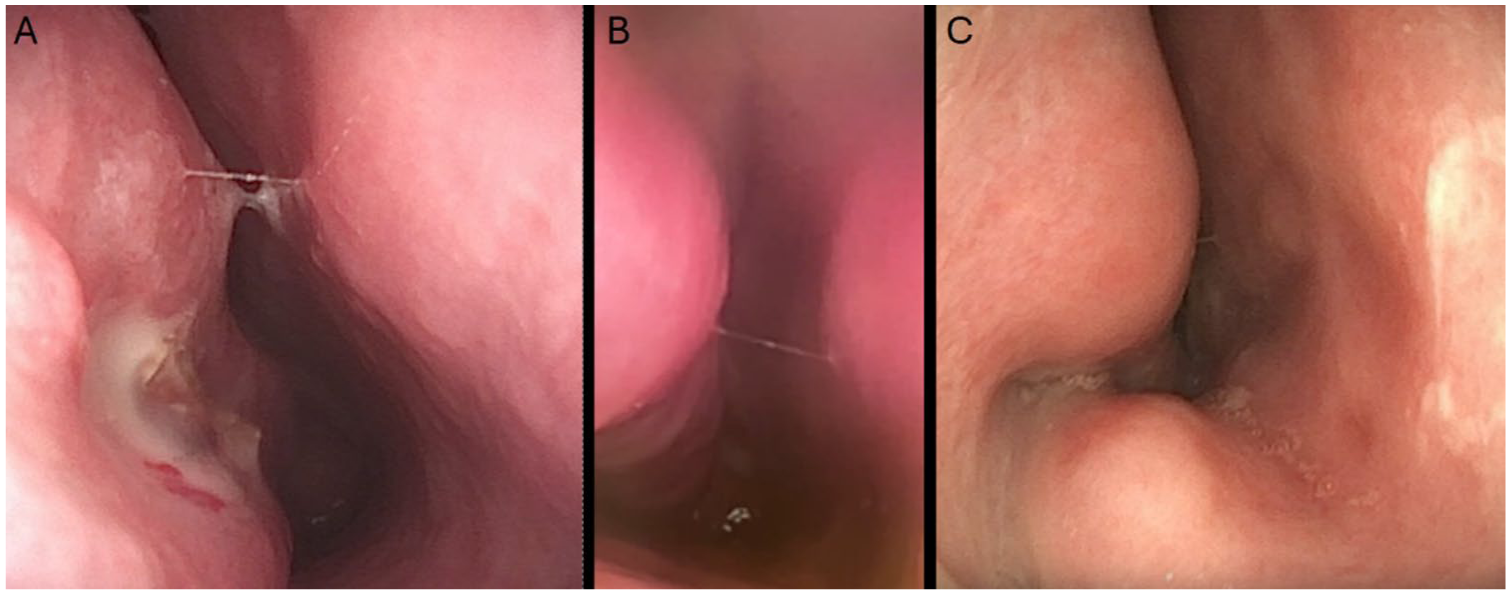
(A) Endoscopic view of the inferior turbinate 6 weeks post-op, showing mild residual crusting but overall reduction in turbinate size and improved airway patency. (B) Endoscopic view 1.5 years post-op, demonstrating resolution of crusting and maintained turbinate reduction with a well-healed mucosal surface. (C) Endoscopic view 4 years post op, illustrating persistent mucosal integrity and stable turbinate reduction without significant regrowth.
Statistical Analysis
Analyses were performed in SPSS 30 (IBM). Proportions of improvement across timepoints were compared using Cochran’s Q test for related samples. Pairwise differences between timepoints used exact McNemar tests with Bonferroni correction for multiple comparisons. For the McNemar analyses, some pairwise comparisons at later timepoints (particularly 4-6 years) had insufficient data in certain subgroups.
A binomial generalized estimating equations (GEE) model with AR(1) working correlation structure was used to assess the effects of time, concurrent surgery types, and their interactions on the probability of reporting no improvement. The model included TimePoint (categorical), concurrent surgery indicators (adenotonsillectomy, septoplasty, sinus surgery, other surgery), and ITR-only status. The GEE model used all available data points and handled missing data through the working correlation structure. Model fit was assessed using the Quasi-likelihood under Independence Model Criterion (QIC). Odds ratios (ORs) and 95% confidence intervals (CIs) are reported. Significance was set at α = 0.05, 2-tailed.
Results
Cohort Characteristics
A total of 326 children (mean age 9.03 ± 4.09 years; 65% male) underwent ITR. Of these, 59 patients (18%) had ITR only, while 267 (82%) underwent at least 1 additional airway procedure. The most common concurrent procedures were adenotonsillectomy (157 patients, 48%), septoplasty (97 patients, 30%), endoscopic sinus surgery (34 patients, 10%), and other procedures including laryngoplasty, supraglottoplasty, and lingual tonsillectomy (30 patients, 9%) (Table 1).
Symptom Improvement by Timepoint and Surgical Group.
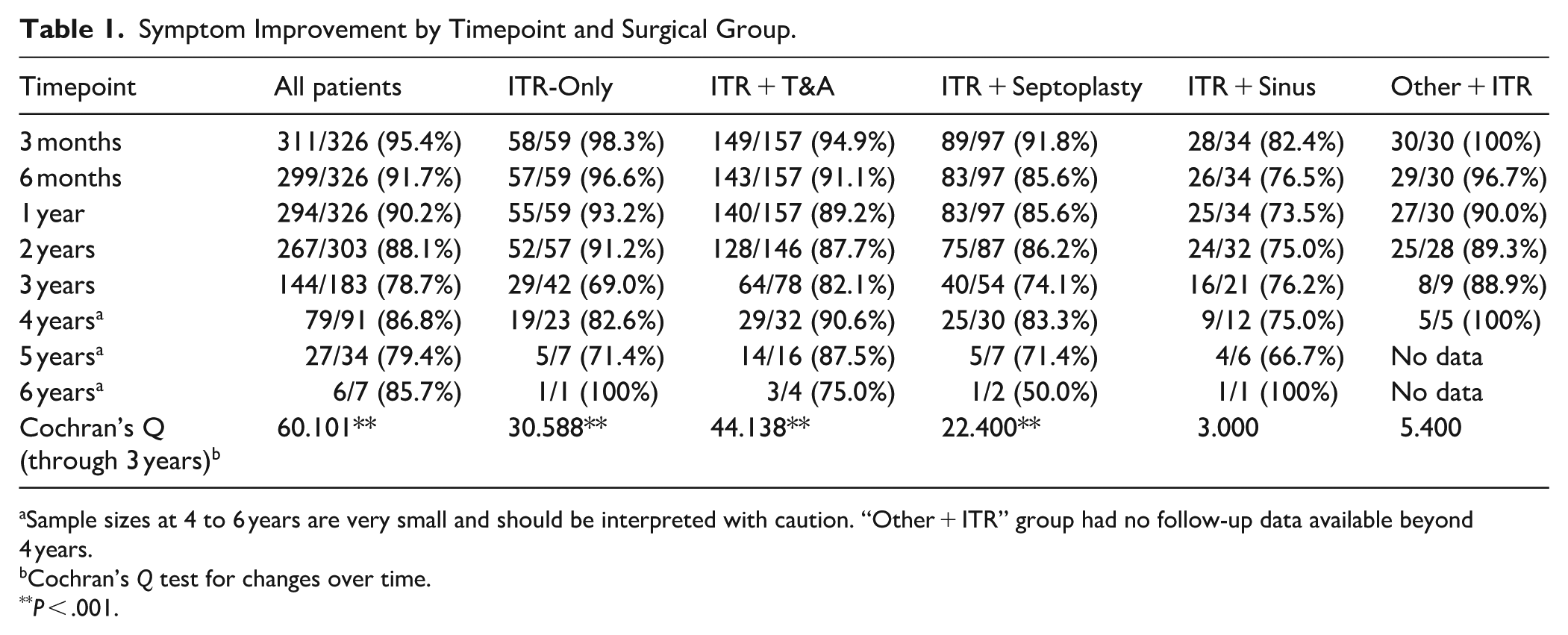
Sample sizes at 4 to 6 years are very small and should be interpreted with caution. “Other + ITR” group had no follow-up data available beyond 4 years.
Cochran’s Q test for changes over time.
P < .001.
Follow-up Retention
Follow-up retention decreased over time: 100% (326/326) at 3 months, 6 months, and 1 year; 93% (303/326) at 2 years; 56% (183/326) at 3 years; 28% (91/326) at 4 years; 10% (34/326) at 5 years; and 2% (7/326) at 6 years. This attrition substantially limits interpretability of results beyond 3 years.
Overall Symptom Improvement Over Time
Parent-reported nasal breathing improvement in the full cohort demonstrated a gradual decline over time (Table 1). At the initial 3-month follow-up, 95.4% (311/326) of patients showed improvement, which decreased to 91.7% (299/326) at 6 months and 90.2% (294/326) at 1 year. The decline continued through 2 years with 88.1% (267/303) reporting improvement, followed by a more marked decrease to 78.7% (144/183) at 3 years. Beyond 3 years, interpretation becomes limited due to small sample sizes, though improvement rates were 86.8% (79/91) at 4 years, 79.4% (27/34) at 5 years, and 85.7% (6/7) at 6 years. The apparent stabilization or improvement at 4 and 6 years likely reflects selection bias from the substantial loss to follow-up rather than true improvement in outcomes.
Statistical Testing Results
Cochran’s Q Test
Cochran’s Q test revealed significant changes in improvement rates over time for all analyzed timeframe combinations. When examining the first 3 timepoints (3 months, 6 months, 1 year), there was a significant decline (Q = 19.913, df = 2, P < .001). This pattern continued when extended to 2 years (Q = 15.447, df = 3, P = .001) and became more pronounced through 3 years (Q = 60.101, df = 4, P < .001). The ITR-only subgroup showed a similar significant pattern through 3 years (Q = 30.588, df = 4, P < .001).
McNemar Pairwise Comparisons
Pairwise comparisons using McNemar’s test identified significant declines from the 3-month baseline to multiple later timepoints. Improvement rates were significantly lower at 6 months (P < .001), 1 year (P < .001), and 2 years (P = 0.035) compared to 3 months. In the ITR-only subgroup, the most striking finding was the significant decline from 3 months to 3 years (P = .002).
Generalized Estimating Equations Analysis
The GEE model analyzed 1596 observations from 326 subjects and showed good model fit (QIC = 1043.651). Time was a significant predictor of treatment failure (Wald χ² = 54.063, df = 7, P < .001). Using 6 years as the reference point, patients were significantly less likely to report no improvement at earlier timepoints, with odds ratios of 0.133 (95% CI 0.033-0.533, P = .004) at 3 months and 0.252 (95% CI 0.065-0.973, P = .046) at 6 months.
Interestingly, concurrent procedures were associated with better outcomes compared to ITR alone. Using ITR alone as the reference group (OR = 1), the odds of reporting no improvement were significantly lower for patients who underwent concurrent septoplasty (OR 0.39, 95% CI 0.21-0.71, P = .002), sinus surgery (OR 0.34, 95% CI 0.14-0.84, P = .020), and for those with other concurrent airway procedures (OR 0.36, 95% CI 0.15-0.89, P = .027). Adenotonsillectomy showed a trend toward improved outcomes (OR 0.50, 95% CI 0.24-1.08, P = .078), while “other surgery” did not significantly affect the odds of persistent symptoms (OR 0.64, 95% CI 0.19-2.16, P = 0.470). Thus, lower odds ratios in these groups indicate a greater likelihood of sustained improvement in nasal breathing compared to ITR alone.
Subgroup Analysis: ITR-Only versus Concurrent Surgery
At the 3-year timepoint, distinct patterns emerged between surgical groups. The ITR-only subgroup showed the lowest improvement rate at 69.0% (29/42), while concurrent surgery groups maintained higher rates: other surgery + ITR at 88.9% (8/9), adenotonsillectomy + ITR at 82.1% (64/78), sinus surgery + ITR at 76.2% (16/21), and septoplasty + ITR at 74.1% (40/54).
Complications
Complications were infrequent over extended follow-up: minor epistaxis occurred in 15 patients (4.6%), major epistaxis requiring operative cauterization in 4 (1.2%), methicillin-resistant Staphylococcus aureus infection in 1 (0.3%), and synechiae formation in 5 (1.5%); no delayed complications were reported beyond the initial postoperative period.
Discussion
This study represents one of the largest pediatric cohorts with extended follow-up following bipolar-cautery inferior turbinate reduction. Our findings demonstrate that while ITR provides excellent short-term outcomes with >90% improvement rates maintained through 1 year, there is a notable decline in efficacy over time, particularly evident at the 3-year mark where overall improvement drops to 78.7%.
Temporal Patterns of Treatment Response
The temporal pattern of symptom improvement reveals several important findings. First, the initial high success rate (95.4% at 3 months) gradually declines through the first year, stabilizes somewhat between years 1 and 2, then shows a more marked decline by year 3. This pattern suggests that the initial treatment effect is robust but may be subject to multiple factors affecting long-term durability.
When examining specific subgroups at 1 and 2 years, differential patterns emerged. The ITR-only group maintained relatively high improvement rates at 1 year (93.2%) and 2 years (91.2%), similar to the adenotonsillectomy + ITR group (89.2% at 1 year, 87.7% at 2 years). However, the septoplasty + ITR group showed earlier decline (85.6% at both 1 and 2 years), while the sinus surgery + ITR group demonstrated the lowest early rates (73.5% at 1 year, 75.0% at 2 years). The other surgery + ITR group maintained 90.0% improvement at 1 year and 89.3% at 2 years. These early differences foreshadowed the more dramatic divergence seen at 3 years.
The biological basis for this decline may include several mechanisms: (1) mucosal remodeling and regeneration over time, (2) continued growth and anatomical changes in the pediatric nasal cavity, (3) progression of underlying allergic or inflammatory disease, or (4) development of compensatory hypertrophy in other nasal structures.9-12 This study provides the first long-term data extending to 6 years in a pediatric population. The pattern of decline we observed, particularly after 2 years, may be unique to the pediatric population and could be related to ongoing nasal growth and development that does not occur in adults.
Impact of Concurrent Procedures
A counterintuitive finding in our analysis was that patients undergoing ITR alone showed poorer long-term outcomes compared to those with concurrent procedures. The ITR-only group’s improvement rate declined from 98.3% at 3 months to 69.0% at 3 years, representing the most dramatic decline among all subgroups. In contrast, patients undergoing concurrent procedures maintained higher improvement rates at 3 years (range: 74.1%-88.9%).
This finding challenges the conventional assumption that isolated procedures would have better outcomes due to more focused intervention. Several explanations are possible: (1) concurrent procedures may address multiple sites of obstruction, providing more comprehensive relief; (2) patients selected for ITR alone may have had isolated turbinate hypertrophy without other anatomical abnormalities, potentially indicating a more severe inflammatory component prone to recurrence; and (3) the adenoids, when removed concurrently, cannot regrow and contribute to future obstruction.
The GEE analysis supports these observations, showing that concurrent septoplasty and sinus surgery were associated with significantly lower odds of treatment failure compared to ITR alone. This suggests a potential synergistic effect when addressing multiple anatomical sites of obstruction simultaneously.
Clinical Implications
These findings have several important clinical implications for pediatric otolaryngologists. Families should be informed that while ITR provides excellent short-term relief, there is a gradual decline in efficacy over time, with approximately 20% to 30% of patients experiencing symptom recurrence by 3 years. This information is crucial for setting realistic expectations and obtaining truly informed consent. Additionally, children with isolated turbinate hypertrophy may benefit from closer long-term monitoring and should be counseled about the higher likelihood of symptom recurrence compared to those undergoing concurrent procedures. This finding challenges conventional thinking and may influence surgical planning decisions. Our data support the need for extended follow-up protocols beyond the typical 1-year period, with particular attention at the 2 to 3 year mark when symptom recurrence becomes more evident. Finally, the subset of patients with symptom recurrence may benefit from revision surgery or alternative treatments, though this requires further study to determine optimal management strategies for treatment failures.
Study Limitations
Several limitations must be acknowledged. First, the dramatic sample attrition over time is a significant concern, with only 56% retention at 3 years and minimal retention beyond that timepoint. This attrition, while typical for pediatric surgical studies, introduces potential selection bias and limits the generalizability of long-term results.
Second, data completeness varied by subgroup, with the “Other Concurrent Surgery” group having no follow-up data beyond 4 years, and several subgroups having only 1 to 2 patients at later timepoints. This necessitated exclusion of certain subgroup comparisons from the McNemar analyses at later timepoints and limits the interpretability of subgroup-specific long-term outcomes.
Third, we did not systematically record preoperative turbinate size using a standardized grading scale (such as the Camacho classification). The absence of objective preoperative turbinate size data prevents us from analyzing whether the degree of turbinate hypertrophy influenced treatment outcomes or predicted long-term success. This represents a significant limitation, as turbinate size may be an important prognostic factor for treatment durability.
Fourth, outcomes were based on parent-reported binary assessments rather than validated symptom scores or objective measures. The use of a single yes/no question about nasal breathing improvement, while practical for telephone follow-up, lacks the nuance of validated instruments like the Nasal Obstruction Symptom Evaluation (NOSE) scale adapted for children.
Fifth, the retrospective nature of the study precluded standardization of medical therapy before or after surgery, and we cannot assess whether optimized medical management might have prevented some cases of symptom recurrence.
Finally, the small sample sizes at 4 to 6 years make these timepoints unsuitable for definitive conclusions, though they are included for completeness and to demonstrate the follow-up challenges inherent in pediatric surgical research. Future research should focus on prospective studies using validated pediatric nasal obstruction scales and objective measures to confirm these findings. Identifying preoperative predictors of long-term success and comparing different turbinate reduction techniques would improve patient selection. Additionally, trials evaluating postoperative medical therapy to maintain surgical benefits warrant investigation.
Conclusion
Bipolar-cautery inferior turbinate reduction provides safe and effective treatment for pediatric nasal obstruction with excellent short-term results. However, our extended follow-up reveals a gradual decline in efficacy over time, with overall improvement rates of 78.7% at 3 years. Patients undergoing ITR alone show more pronounced symptom recurrence compared to those with concurrent airway procedures. These findings emphasize the importance of appropriate patient selection, comprehensive surgical planning when indicated, and long-term follow-up protocols. While technical refinements and medical adjuncts may improve durability, families should be counseled about the potential for symptom recurrence over time, particularly in patients undergoing isolated turbinate reduction.
Footnotes
Acknowledgements
The authors thank the staff of Pediatric ENT of Oklahoma for their assistance with data collection and patient follow-up.
Ethical Considerations
This study was approved by the Oklahoma State University—Center for Health Sciences Institutional Review Board (IRB #2024160).
Consent to Participate
Verbal informed consent was obtained from parents or guardians during telephone follow-up, and written consent was obtained from those whose nasal endoscopy images were used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.