
Abstract
Background:
Chronic maxillary atelectasis (CMA) describes the loss of maxillary sinus volume and has been well-described in the literature under many different names, creating inconsistency in reporting. A recent proposal has standardized the nomenclature but does not include disease of other paranasal sinuses.
Objective:
We describe a unique case of chronic ethmoid atelectasis, briefly review literature associated with CMA, and propose an expanded classification of chronic sinus atelectasis.
Results:
A 70-year-old man presented to the emergency department with transient vision loss and was incidentally found to have sinus opacification on MRI. At his otolaryngology follow-up, he did not have any signs of sinonasal symptoms, hypoglobus, or enophthalmos. CT confirmed sinus opacification which was correlated with lateralized left middle turbinate and uncinate process. The patient underwent functional endoscopic sinus surgery to correct the anatomical changes.
Conclusions:
The spectrum of atelectasis affecting the ethmoids mirrors what has been described for CMA, potentially indicating a similar disease process affecting different areas. If this falls along the same spectrum of disease, the grading system applied to CMA may be applied to other paranasal sinuses.
Keywords
Introduction
First noted by Montgomery in 1964, 1 chronic maxillary atelectasis (CMA) is a well-described clinical entity and has significant overlap with silent sinus syndrome. Diagnostic criteria include loss of maxillary sinus volume with inward bowing of the maxillary sinus walls and opacification on computed tomography (CT). 2 Several staging and classification schema have been developed, describing the extent of deformity and clinical evidence of volume loss. 2 More recently, in an effort to simplify diagnostic classification between atelectasis and silent sinus syndrome, this has expanded to include involvement or absence of sinus-related symptoms. 3 Currently all means of classifying this disease process are limited to the maxillary sinus, yet various reports4,5 and our clinical experience have identified atelectasis of sinuses beyond the maxillary sinus. Here, we present a case of ethmoidal sinus disease that mimics the findings typically associated with CMA and consider a modified classification system that may be applied to pathology within the ethmoid and frontal sinuses.
Case Presentation
A 70-year-old man presented to the emergency department with concern for possible amaurosis fugax following a transient episode of partial unilateral vision loss affecting the superior third of his left visual field. All symptoms had resolved by the time of the visit. Magnetic resonance imaging of the brain was otherwise unremarkable except for incidental findings of complete chronic left maxillary sinus opacification with T1 heterogeneity, as well as moderate opacification of the left frontal sinus with concern for an associated encephalocele. He was referred to our otolaryngology clinic for further evaluation.
Clinically, the patient denied facial pain, pressure, epistaxis, obstructed nasal breathing, rhinorrhea, concerns with maxillary dentition, headaches, diplopia, or prior sinus surgery. Past medical history was notable for left-sided sensorineural hearing loss, right-sided conductive hearing loss, and allergic rhinitis diagnosed 11 years earlier. On exam, the patient did not demonstrate obvious signs of orbital displacement, although exophthalmometry was not performed. Nasal endoscopy revealed a lateralized left middle turbinate and uncinate process, both adherent to the medial orbital wall, resulting in complete obstruction of the left middle meatus. A computed tomography (CT) scan showed persistent left maxillary and frontal sinus opacification, scattered mucosal thickening within the left ethmoid air cells, and complete opacification of the left frontoethmoidal recess (Figure 1). Due to the persistence of sinus disease on serial imaging and the anatomical changes seen endoscopically, the patient was scheduled for functional endoscopic sinus surgery.
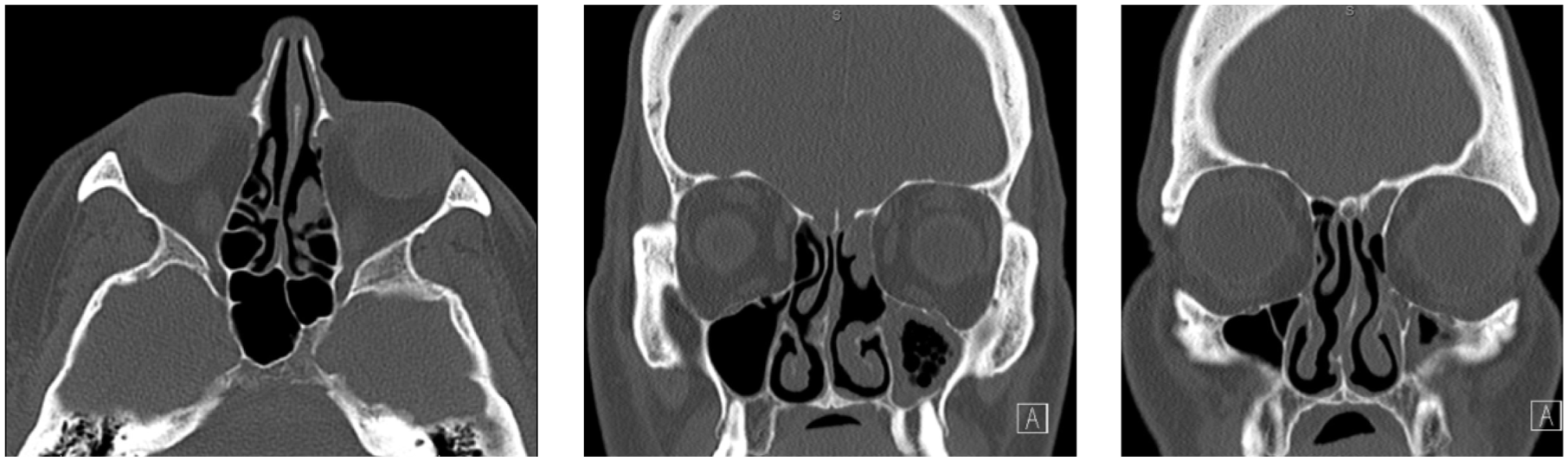
Axial and coronal CT images of patient with chronic ethmoid atelectasis. Imaging was notable for a contracted and shortened middle turbinate, lateralized uncinate process, partially opacified maxillary sinus with no contractile changes, collapse of the ethmoid bulla onto the basal lamella, opacification of the frontal sinus with no contractile changes. The agger nasi was aerated without collapse.
Intraoperatively, improved visualization of the ethmoid cavity revealed that the ethmoid bulla had collapsed in an anterior-posterior direction and was adherent to the basal lamella (Figure 2). An antrostomy, anterior ethmoidectomy, and frontal sinusotomy were performed uneventfully. The maxillary and frontal sinus mucosa demonstrated polypoid changes with thick, inspissated mucoid secretions.
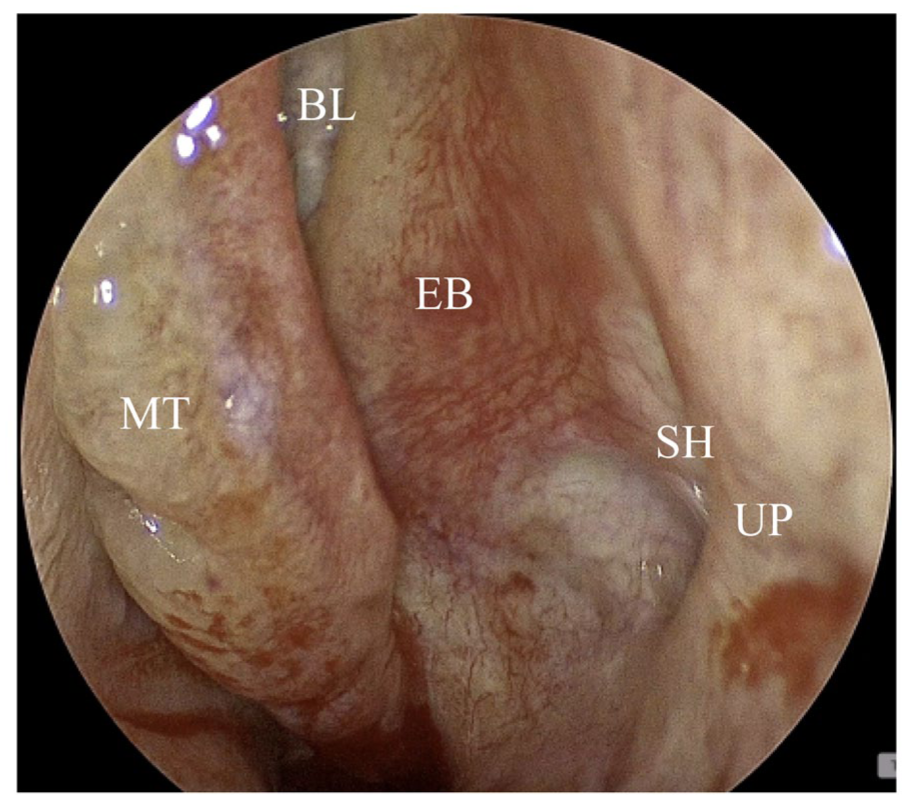
Intraoperative endoscopic view of middle meatus. The middle turbinate had been surgically medialized demonstrating a collapsed ethmoid bulla adherent to the basal lamella. The middle turbinate was contracted posteriorly and superiorly. The uncinate process was lateralized adherent to the lamina papyracea, collapsing the semilunar hiatus.
Discussion
Logically speaking, an obstructed ostium may lead to expansile mucocele formation; however, the opposite occurs in atelectasis. Davidson et al 6 measured negative sinus pressures in this pathology of −23 mmHg, and Rose et al 7 suggested that slow resorption of fluid within post-obstructive mucus leads to sub-atmospheric pressures and eventual remodeling of the surrounding bone and tissue. Based on the volume of literature and our clinical experience, ethmoid and frontal atelectasis are significantly less common than maxillary atelectasis. McArdle and Perry suggest the maxillary sinus’ large size and relatively narrow ostium enable a stronger and more constant negative pressure to be generated and maintained. 4 Despite the difference in frequency, there may be similarities in the pathophysiology of sinus atelectasis among maxillary, ethmoidal, and frontal cases.
As noted previously, nomenclature surrounding sinus atelectasis has been varied. CMA was first reported by Montgomery in 1964, 1 but the term “silent sinus syndrome” (SSS) was characterized by Soparkar et al 8 to describe cases of enophthalmos and hypoglobus without sinonasal symptoms. Kass et al 2 went on to describe a proposed grading system in 1997, albeit referring to the disease process as “chronic maxillary atelectasis.” They described a spectrum of deformities: Stage I with a lateralized maxillary fontanel to Stage III with enophthalmos, hypoglobus and/or midfacial deformity. Alternative names include “imploding antrum syndrome.” 7 Importantly, Amin et al 3 proposed a modified classification system that would allow both CMA and SSS to be diagnosed in a unified fashion by the addition of an “a vs. b” subgroup depending on the presence of sinus symptoms. These characterizations of sinus atelectasis exclude trauma and iatrogenic causes, however a growing number of case reports from these etiologies suggests a need to reassess. Cases of sinus atelectasis have been described following orbital trauma, sinonasal trauma, and surgeries such as rhinoplasty.5,9-11 As far as our search, treatments and outcomes of traumatic and iatrogenic sinus atelectasis do not differ significantly from those of idiopathic disease.
Currently, there is not enough evidence or data on ethmoid atelectasis to support adoption of a novel classification system. Considering the difficulties in nomenclature with chronic maxillary atelectasis, however, we would like to propose an expanded classification that may be used to standardize future research communication. This staging system would be expanded from Amin et al to include atelectasis of the ethmoid and frontal sinuses as well as sinus atelectasis arising from trauma or iatrogenic causes. We hope that future investigations into pathophysiology of sinus atelectasis support the adoption of this system.
Although rare, chronic ethmoid sinus atelectasis (CEA) has been described from both idiopathic and traumatic etiologies. McArdle et al 4 described a case of “Ethmoid Silent Sinus Syndrome” presenting with acute enophthalmos caused by collapse and opacification of left ethmoid air cells. German researcher Heilmeier et al 12 also described a case of enophthalmos due to nontraumatic ethmoid atelectasis. Later, Brown et al 5 described ethmoid atelectasis in a patient who presented with enophthalmos 12 years after orbital trauma. In addition to these, there have been additional cases of traditional CMA with ethmoidal involvement.13-15 This is, to the best of our knowledge, the first report of non-traumatic chronic ethmoid atelectasis that is asymptomatic without enophthalmos. The range of clinical presentations of ethmoidal sinus atelectasis in these case reports appear to mirror the spectrum of CMA in terms of symptomatic and asymptomatic presentations with or without enophthalmos. In conjunction with anatomical plausibility, this may suggest a similar etiology of disease between CMA and its ethmoidal variant. While opacification was noted in both the maxillary and frontal sinuses, the authors feel the disease process described originated within the ethmoid cavity, as the bulla demonstrated evidence of severe collapse while the maxillary and frontal sinuses did not. Thus, it can be considered true CEA and not CMA with ethmoid sinus involvement.
To avoid adding additional nomenclature to the literature, we propose the expansion of the staging system of CMA provided by Amin et al. 3 The group of diseases as a whole may be considered chronic sinus atelectasis and would be sub-divided based on the suspected sinus of origin. If multiple sinuses are involved, we propose naming based on the sinus of origin with additional qualifier such as chronic maxillary atelectasis with combined involvement—CMA-C. Notably the sphenoid sinus is not classified. Per our review of the literature and clinical experience we could not find evidence this syndrome exists or at least has yet to be recognized. Thus, we have decided to forgo its inclusion. It would be a welcome addition to the literature once described.
As part of the expanded nomenclature, we also propose the inclusion of all causes of sinus atelectasis including those from trauma, iatrogenesis, malignancy, or idiopathic causes. A separate modifier to denote the etiology does not seem necessary as etiology does not appear to have therapeutic or prognostic significance, according to the current literature. Cases of enophthalmos or globe malposition due to direct orbital trauma, which generally occurs within 4 weeks, would not be included. 9
This group of diagnoses may be further assessed with the previously mentioned staging system (Table 1). Based on this system, our reported case would be classified as CEA stage IIa due to the presence of a bony deformity and absence of clinical deformity (enophthalmos) or sinonasal symptoms. The cases in McArdle and Perry 4 and Brown et al 5 would be classified as CEA stage IIIa due to the presence of a clinical deformity without sinonasal symptoms. A spectrum of frontal atelectasis has also been described, which can be implemented into this classification system. Khatoon et al 16 and Naik et al 17 both describe a case of isolated frontal atelectasis causing ipsilateral hyperglobus and enophthalmos without significant sinonasal symptoms. These presentations could be categorized as CFA, Stage IIIa. Alternatively, Veryat et al 18 describe multiple cases of isolated membranous deformity (shift in the inter-frontal septum) which were symptomatic with frontal pressure and purulent rhinorrhea. Thus, this could be categorized as CFA, Stage Ib. This staging system relies on differences in phenotypic presentation to provide consistent reporting guidelines. Future subgroup outcome analysis may provide additional information to support this classification scheme or provide better, therapeutically and prognostically significant criteria. We hope that future research will demonstrate that this expanded nomenclature provides diagnostic consistency, improved management, and simplified reporting.
Criteria for Chronic Sinus Atelectasis in the Various Paranasal Sinuses.
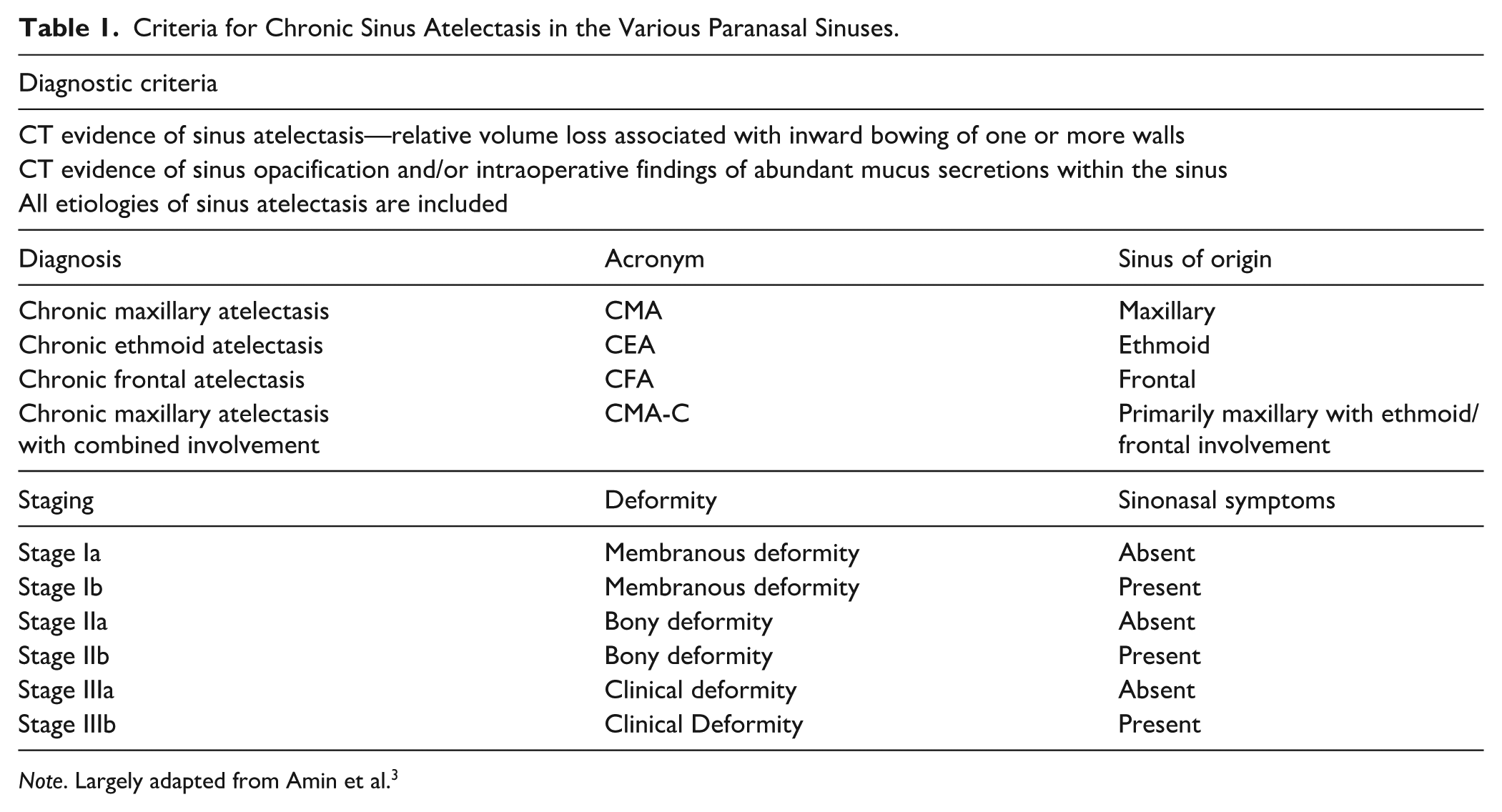
Note. Largely adapted from Amin et al. 3
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent to Participate
Informed consent was obtained verbally before participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.