
Abstract
Background:
This study aims to assess the effectiveness of high-fidelity simulation training in enhancing skills for frontal sinus surgery (FSS) within the framework of continuing medical education.
Methods:
A cross-sectional, within-subject study was conducted during a CME-accredited national frontal sinus surgery simulation course. Participants completed pre- and post-course surveys rating potential deterrents to FSS. Paired statistical analyses assessed changes in deterrent ratings, and correlational analyses evaluated relationships with surgical experience and case volume.
Results:
Twenty-eight participants completed both pre- and post-course surveys. Mean time in practice was 14 years, with an average FSS volume of 2 cases per month. Baseline deterrence was moderate (mean 5.10/10), driven primarily by concern for skull base violation and technical difficulty. Following simulation, overall deterrence decreased significantly by 1.27 points (to 3.83; P < .05), with 7 of 9 deterrents showing significant reduction. The largest improvements were seen in apprehension regarding skull base injury, technical challenge, and adequacy of dissection. Factors related to operative time and prior experience showed minimal change. Case volume correlated with lower baseline and post-simulation hesitancy for select deterrents, while years in practice and interval since last FSS did not. All participants reported improved confidence, and the majority anticipated increased incorporation of FSS into their practice.
Conclusions:
Simulation-based CME significantly reduced modifiable deterrents and improved confidence among practicing otolaryngologists performing FSS, regardless of years in practice. These findings support simulation as a valuable adjunct for ongoing professional development, enabling experienced surgeons to recalibrate risk perception, refine technical judgment, and support lifelong surgical learning.
Keywords
Introduction
Endoscopic frontal sinus surgery (FSS) is a widely accepted surgery commonly performed by otolaryngologists.1,2 Though regularly performed, cases require navigating a corridor flanked by the orbit, skull base, and critical neurovasculature where surgical confidence is vital. While otolaryngologists are trained for proficiency here, surgical exposure and comfort levels vary widely. 3
Despite its growing role in residency training,4-6 simulation remains underused in continuing medical education (CME), where learning needs differ from trainees. For experienced otolaryngologists, surgical simulation may provide a platform to refine skills, reevaluate familiarity, and delineate hesitancies surrounding evolving techniques.
Objective
This study aimed to characterize perceived deterrents for FSS among practicing otolaryngologists and assess how a simulation-based CME course may influence surgical self-assessment and confidence.
Methods
A cross-sectional study was conducted during a CME-accredited national otolaryngology meeting. Sixty-two otolaryngologists from diverse institutions enrolled in the course which included expert technical teaching7,8 and live surgical demonstration on a high-fidelity 3D model as previously described. 6 Participants who completed both pre- and post-course surveys were included in analysis.
Before simulation, participants reported residency graduation year, monthly FSS case volume, and the date of last case. Participants completed a pre-course survey, rating potential deterrents to FSS in practice on a 0 to 10 scale (0 = no deterrent, 10 = significant deterrent). Deterrents included apprehension about: violating skull base and/or orbit, thorough dissection, operative time, anatomic knowledge, technical difficulty, low case volume, prolonged case interval, and inadequate training.
A fellowship-trained rhinologist instructed and demonstrated FSS dissection with live endoscopic video and CT guidance. Established surgical landmarks and techniques were reviewed throughout. Participants then performed a simulated FSS using the same 3D models and image guidance. Post-simulation, participants completed the survey with additional questions regarding confidence, understanding, and perceived educational impact. This within-subject design allowed each participant to serve as their own control.
Primary outcomes included deterrent ratings before and after simulation. Paired t-tests and Spearman correlations assessed changes in confidence, technical apprehension, and perceived risk, and influence of surgical simulation training on participant hesitancy toward performing FSS. Alpha was set at .05. IRB approval was obtained (IRB#00002893); participation was voluntary and anonymous.
Results
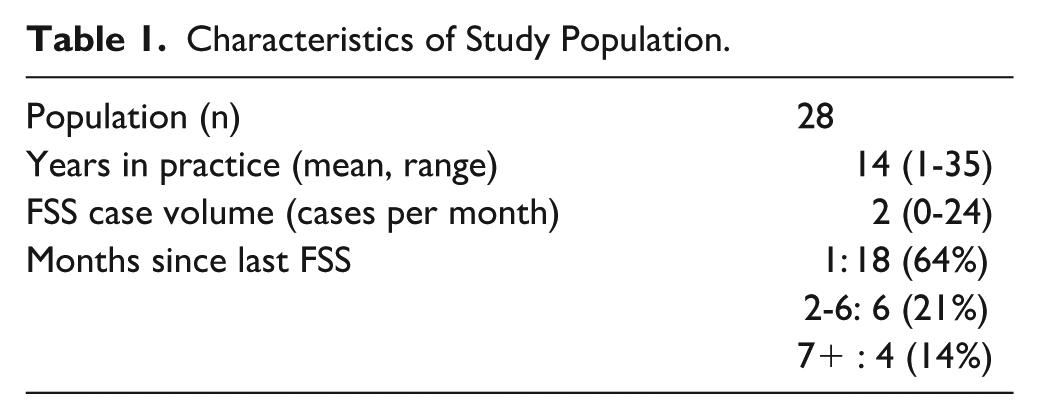
The study population included 28 practicing otolaryngologists (Table 1). Participants had been in practice for 1 to 35 years (mean = 14). FSS volume ranged from 0 to 10 per month (mean = 2). At time of survey, 64% performed FSS within the past month, 21% within 2 to 6 months, and 14% over 6 months ago.
Characteristics of Study Population.
Before simulation, the mean deterrent score was 5.10 out of 10, with “potential to violate skull base” rated highest (6.25) and procedure duration lowest (3.75). After simulation, “inadequate residency training” emerged as the top concern (5.25), while “knowledge of frontal sinus anatomy” was lowest (2.89). On average, overall deterrence scores decreased by 1.27 points (5.10 to 3.83), with 7 of the 9 deterrents significantly reduced (P < .05; Figure 1). Largest reductions were seen for skull base violation (−2.18, P < .001), technical challenge (−2.04, P < .001) and apprehension about thorough dissection (−1.64, P = .003). In contrast, deterrents related to time and prior experience showed minimal change.
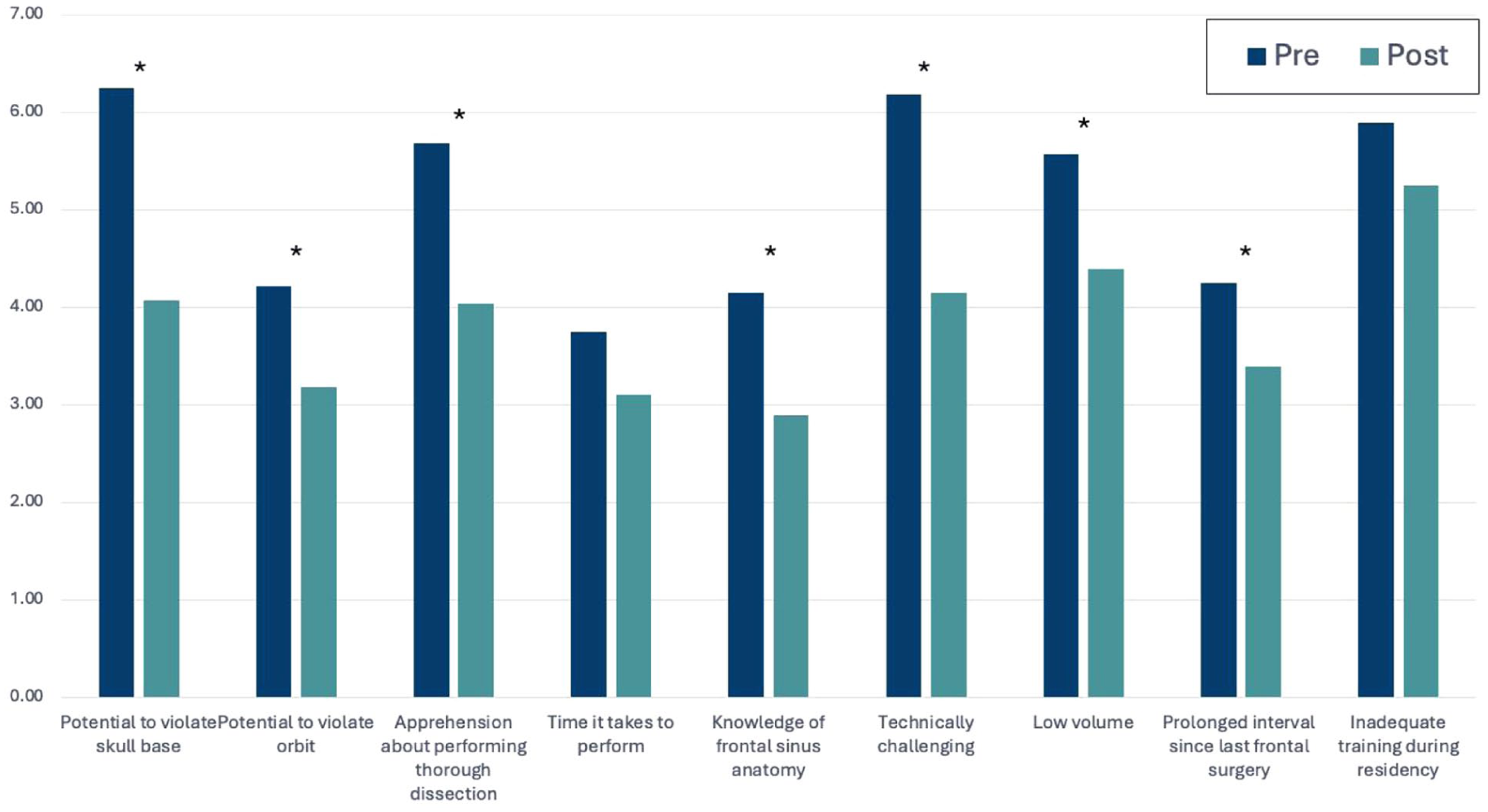
Hesitancy ratings of various deterrents in frontal sinus surgery.
Experience-based correlational analysis (Spearman’s rank) revealed higher volume was associated with lower pre-simulation hesitancy for thorough dissection (ρ = −0.41, P = .029) and trended toward lower orbit-violation concern (ρ = −0.37, P = .05). After simulation, greater volume remained linked to reduced post-training hesitancy about frontal sinus anatomy (ρ = −0.55, P = .003) and orbital risk (ρ = −0.45, P = .015). In contrast, years in practice and interval from last FSS showed no significant correlations with either pre- or post-simulation hesitancy. No significant association was found between volume, experience, or time since last case and hesitancy reduction.
Following simulation, all participants (100%) reported improved confidence in FSS. Most endorsed improved understanding (96.4%) and anticipated incorporating more FSS into practice (92.8%).
Discussion
Our findings show that even experienced otolaryngologists with regular case exposure retain hesitancy when operating within the frontal sinus, influenced by anatomic complexity and individual risk perception. Surgical simulation helped surgeons calibrate their confidence and refine distinctions between appropriate caution and hesitation in practice.
Intuitively, baseline apprehension was driven primarily by high-stakes surgical concerns including risk to skull base, technical difficulty, and training adequacy. Post-simulation, the greatest reductions occurred in these same areas, while systemic factors like procedure length and case volume remained largely unchanged. Correlation analysis reinforced the simulation’s value in addressing modifiable deterrents across varied practice profiles with no single baseline feature sufficiently predicting confidence shifts in hesitancy metrics. Importantly, inadequate residency training became the leading deterrent, despite enhanced anatomic and technical confidence overall, reaffirming that simulation cannot replace foundational training but instead supports its utility in targeted self-assessment and growth.
Limitations included a small sample size, subjectivity of survey data, and potential response bias, preventing conclusions of causality. It should be noted that proficient FSS requires comprehensive training in surgical decision-making, preoperative planning, surgical adaptability, and technical skill. Assessing simulation’s effect on FSS proficiency would require a rigorous curriculum with serial cases, various models, surgical planning exercises, and objective assessments of skill.
This study addresses a notable gap in the literature by examining simulation’s role in CME for practicing surgeons. Beyond its traditional use in early training, simulation is a valuable tool for refining judgment and supporting ongoing self-assessment across a surgeon’s career.
Footnotes
Author Note
Simulation course conducted at AAO-HNSF Annual Meeting (2023, 2024).
Ethical Considerations
IRB approval was obtained (IRB#00002893).
Consent to Participate
Participation was voluntary and anonymous.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter John Wormald: Acclarent, Medtronic, Neilmed, Stryker, Chitogel, Fusetec. Masayoshi Takashima: Medtronic, Aerin Medical, Neurent, Sanofi, Spirair, Lyra Therapeutics, Cyrano Therapeutics, LivaNova, and Apnimed. Philip G. Chen: Optinose, GSK, Amgen, Sanofi. Omar G. Ahmed: Sanofi, Aerin Medical, Neuromark, Spirair, Livanova, and Medtronic. Michael Yim: Aerin, Chitogel, Sanofi, Spirair. Mackenzie Latour, Elizabeth Bryan: No conflicts of interest to disclose.
Data Availability Statement
Due to the sensitive nature of the dataset and participant privacy protections, data repository is not publicly available but can be accessed upon reasonable request by reviewers.