
Abstract
Objectives:
Auditory localization, an essential skill for survival and communication, enables individuals to identify the source of sounds in their environment. Hearing loss (HL) in one or both ears often disrupts binaural hearing mechanisms, compromising auditory localization abilities. This study aimed to compare auditory localization abilities among unilateral cochlear implant (UnCI) users, bimodal cochlear implant (BimCI) users, and individuals with normal hearing (NH).
Methods:
This study included a total of 119 participants: 50 with NH, 46 UnCIs, and 23 BimCIs. The Auditory Localization Scale was used to compare the participants’ localization abilities. The scale consists of 24 items across 5 subdimensions: traffic zone, outdoor situations, indoor situations, psychological aspects, and quiet situations. On this scale, higher scores represent greater difficulty with hearing and sound localization, whereas lower scores correspond to better performance in these situations.
Results:
A statistically significant difference was observed among the 3 groups across all subsections of the Auditory Localization Scale (traffic-zone, P < .001; outdoor situations, P < .001; indoor situations, P < .001; psychological aspects, P = .001; quiet situations, P < .001), as well as in the total score (P < .001). Post-hoc analyses revealed no significant difference between the bimodal and unilateral CI users (P > .017). However, the NH group obtained significantly lower scores across all subsections and in the total score compared with both CI groups. (P < .017).
Conclusions:
While bimodal hearing is advantageous for providing binaural signals, it may not be adequate for auditory localization; consequently, further endeavors are required to enhance subjective benefits and hearing outcomes in adult CI users.
Introduction
Depending on the severity of the hearing loss (HL), the most common rehabilitation options are hearing aids (HAs) or cochlear implants (CIs). Cochlear implantation is recommended for individuals with severe-to-profound sensorineural HL (SNHL) who receive minimal benefit from HAs. 1 Traditionally, most of these individuals receive unilateral CIs, and placement of a contralateral HA in the non-implanted ear is frequently recommended, becoming standard clinical practice. 2 Combining electrical stimulation via a CI in 1 ear and acoustic amplification via a HA in the other ear is defined as bimodal hearing. Bimodal stimulation can facilitate bilateral processing and binaural redundancy, leading to improved sound localization and speech perception in noise due to interaural level differences.3,4
Sound localization is vital for both survival and communication, providing awareness of the location of sounds in the environment. This process relies on precise encoding of binaural and monaural auditory cues and the decoding of neural signals.5,6 Binaural cues include interaural time (ITD) and level differences (ILD). These cues are conveyed in the temporal-fine structure (instantaneous changes in pressure or intensity over time) and temporal envelope (slower, more gradual changes in pressure or intensity over time) of a signal. 7 The ITD cues are primarily used for localizing low-frequency sounds (below 1500 Hz), and the ILD cues are primarily used for localizing high frequency sounds (above 1500 Hz). Monaural spectral cues are coded in high-frequencies (over 5000 Hz) and used to locate sounds in the front and back dimensions, as well as vertically. 8 When the binaural hearing mechanisms are disrupted due to HL in 1 or 2 ears, the auditory localization abilities of individuals are often compromised. 9
Auditory localization abilities can be assessed behaviorally or through self-report measurements following cochlear implantation. 10 Behavioral assessments typically measure localization in the horizontal or both horizontal and vertical planes, requiring participants to identify the sound source within a loudspeaker array. 4 Recently, self-report assessments based on patients’ daily-life experiences have gained significance, providing valuable information regarding real-world functionality and quality of life. 10 Common self-report questionnaires include the Spatial and Qualities of Hearing Scale (SSQ) and the Spatial Hearing Questionnaire (SHQ). 11 However, these instruments do not focus exclusively on auditory localization skills. To address this, Neelamegarajan et al 11 developed the Questionnaire for Auditory Localization, designed to assess localization difficulties in individuals with HL and to evaluate outcomes of amplification device use and localization training.
Behavioral localization equipment is not available in every audiology clinic, and the testing rooms used for these assessments provide only a simulated representation of real-life listening environments. Additionally, subjective self-report questionnaires offer clinicians faster and more practical information. In line with this information, the present study aimed to investigate differences in auditory localization abilities among unilateral CI (UnCI) users, bimodal CI (BimCI) users, and individuals with normal hearing (NH) using the Turkish version of the Questionnaire for Auditory Localization.
In line with this information, the current study aimed to investigate differences in auditory localization abilities among UnCI users, BimCI users, and individuals with NH using the Questionnaire for Auditory Localization Turkish version.
Materials and Methods
This study was conducted at Hacettepe University Faculty of Health Sciences, Audiology Department, and received ethical approval from the Hacettepe University Health Science Research Ethics Board (SBA 24/402). The participants provided informed consent on the day of enrollment.
Participants
A total of 119 individuals participated in the current study, divided into 3 groups: 50 individuals with NH as the control group, and the study group – CI users – included 46 UnCI and 23 BimCI users.
The following inclusion criteria were used to determine the CI groups: participants had to be at least 18 years of age, to have received their CIs at Hacettepe University Hospital, to have used conventional HAs bilaterally prior to implantation, and to use either unilateral or bimodal CIs. Participants with UnCI users had bilateral severe-to-profound SNHL, used a CI in only one ear for at least 12 months, and did not use a HA in the contralateral ear after implantation. Participants with BimCI users had bilateral severe-to-profound SNHL, used a CI in one ear for at least 12 months, and wore a conventional HA regularly in the contralateral ear since the diagnosis of hearing loss. All CI participants were required to receive regular implant programing at the Hacettepe University Audiology Department and to have no diagnosed physical or psychological disabilities other than hearing loss.
The NH group included individuals who met the following criteria: being at least 18 years old, having no history of hearing problems or diagnosed hearing loss, and having no diagnosed physical or psychological disabilities.
Test Battery: The Questionnaire for Auditory Localization
The Questionnaire for Auditory Localization, developed by Neelamegarajan et al, evaluates localization of auditory stimuli in both noisy and quiet conditions, considering psychological and social contexts. Its validity and reliability were established in a sample of 120 individuals aged 18 to 50 years. 11
The Questionnaire for Auditory Localization has been adapted in Turkish as the Auditory Localization Scale. 12 Therefore, this study will refer to the Questionnaire for Auditory Localization as the Auditory Localization Scale (ALS).
The validity and reliability of the Turkish version of the ALS were evaluated using data collected from 140 NH individuals and 158 individuals with SNHL. The validity and reliability results of the scale are very high. 12 The scale consists of 5 subsections and 24 items: 5 questions related to traffic-heavy areas (traffic zone), 4 questions related to the outdoor environment (outdoor situations), 2 questions regarding the indoor environment and situations in the immediate environment (indoor situations), 4 questions related to the psychological aspects of hearing (psychological aspects), and 9 questions related to localization in silent situations (quiet situations). It has a five-point Likert-type response format: (1) never, (2) almost never, (3) sometimes, (4) almost always, (5) always. The higher scores suggest that individuals experience difficulty with sound localization and hearing in the specified situations, whereas the lower scores reflect good hearing and sound localization in those situations. After informed consent and detailed history, the scale was administered to the participants.
Statistical Analysis
SPSS version23 was used for statistical analysis. Visual approaches (histogram and probability graphs) and analytic methods (Kolmogrov-Smirnov/Shapiro-Wilk test) were used to determine whether variables were normally distributed. Means, standard deviations, and percentages were used for descriptive analysis. Pairwise comparisons were conducted using the Mann-Whitney U test. Kruskal-Wallis and Mann-Whitney U tests with Bonferroni correction were used to compare 3 groups. Chi-Squared analysis compared categorical variables. P < .05 indicated statistical significance.
Results
The UnCI group included 32 female and 14 male participants, the BimCI group 14 female and 9 male participants, and the NH group 42 female and 8 male participants. Comparative statistical analysis showed that there were no statistically significant differences in gender (P = .73, P > .05), chronological age (0.52, P > .05), and education level (0.97, P > .05) between the groups. Also, there were no significant differences between the UnCI and BimCI groups in terms of the age at diagnosis (P = .86, P > .05), age at implantation (P = .81, P > .05) and age at hearing aid use (P = .92, P > .05; Table 1).
Demographics of the Groups.
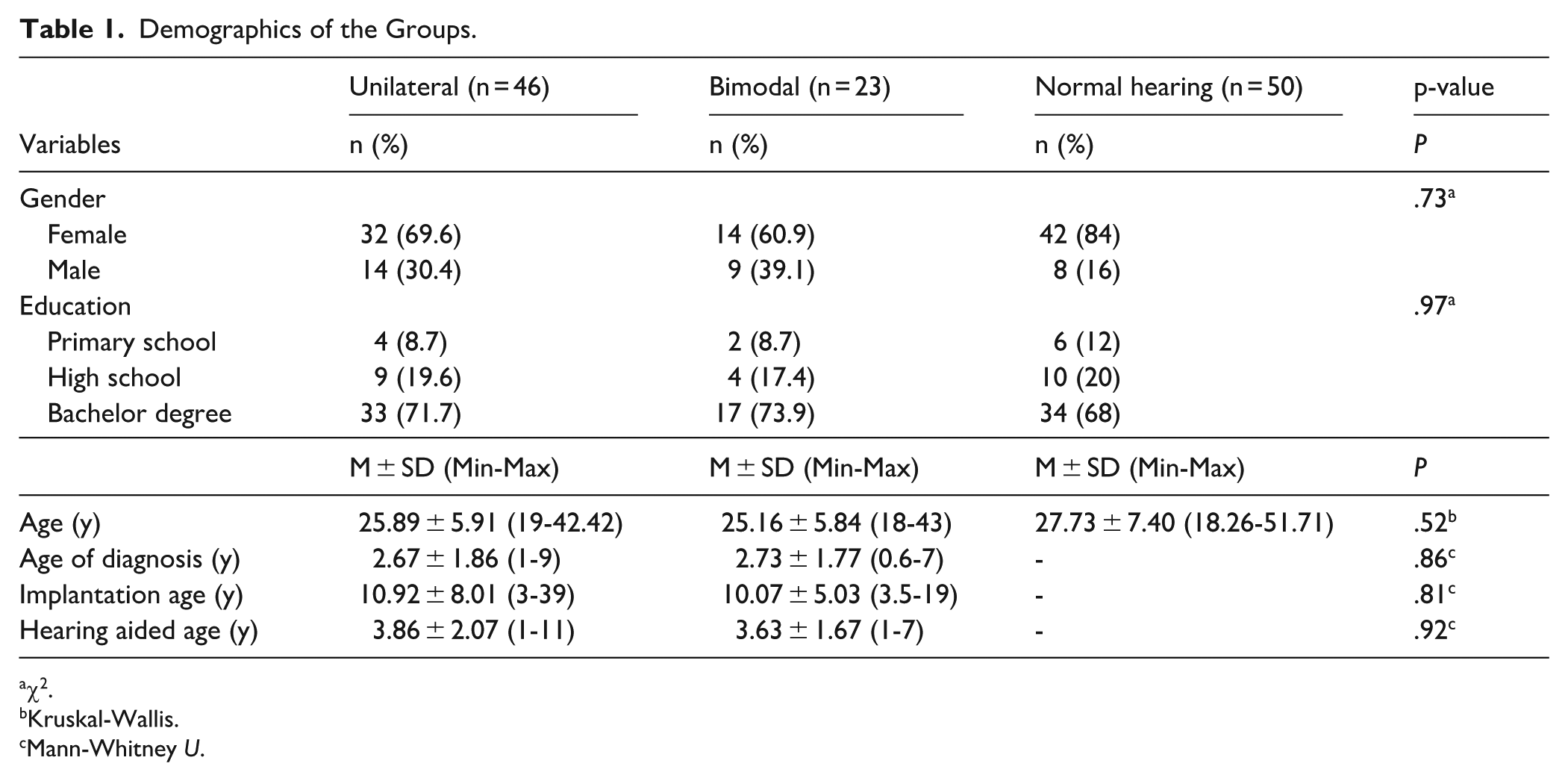
χ2.
Kruskal-Wallis.
Mann-Whitney U.
The descriptive statistics for the ALS subsections and total scores are presented below. For the UnCI group, the mean scores were as follows: Traffic zone, 13.91 ± 4.84; Outdoor situations, 10.13 ± 3.40; Indoor situations, 5.07 ± 1.94; Psychological aspects, 11.37 ± 3.14; Quiet situations, 20.37 ± 5.42; and the total score, 61.20 ± 14.64.
For the BimCI group, the mean scores were: Traffic zone, 12.39 ± 4.21; Outdoor situations, 11.74 ± 4.26; Indoor situations, 4.61 ± 1.97; Psychological aspects, 11.87 ± 3.31; Quiet situations, 21.83 ± 6.84; and the total score, 62.30 ± 14.22.
For the NH group, the mean scores were: Traffic zone, 7.96 ± 3.13; Outdoor situations, 7.48 ± 2.71; Indoor situations, 3.22 ± 1.13; Psychological aspects, 9.44 ± 2.88; Quiet situations, 12.34 ± 3.66; and the total score, 40.44 ± 9.82.
Significant differences were observed among the UnCI, BimCI, and NH groups across all ALS subsections and in total scores (all P < .05). Post-hoc pairwise comparisons showed no significant differences between the UnCIs and BimCIs groups (all P > .017), whereas both CI groups had significantly higher scores than the NH group (all P < .017). Detailed comparison results are presented in Table 2 and Figure 1.
Kruskal–Wallis and Post-hoc Mann–Whitney U Comparison Results.
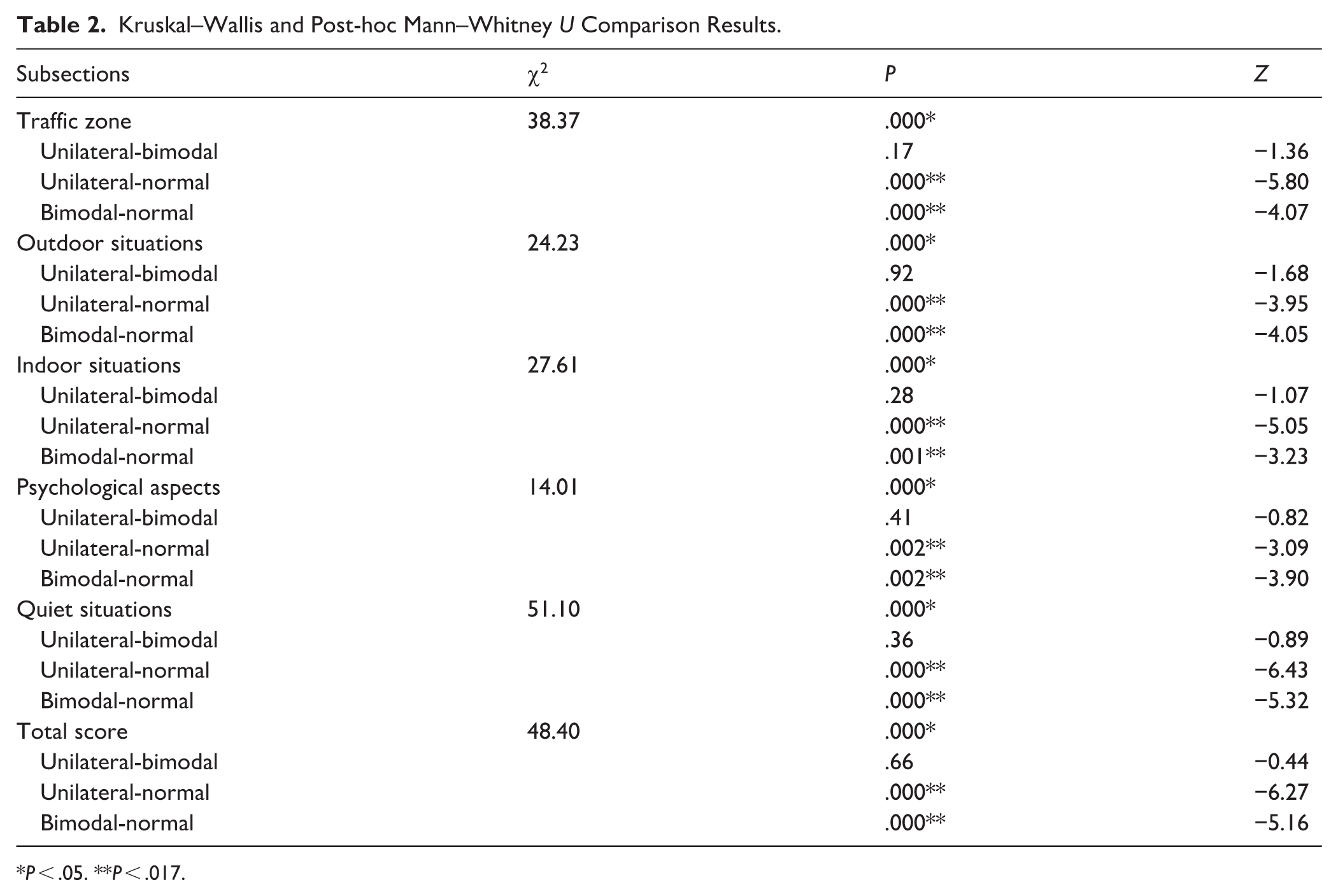
P < .05. **P < .017.
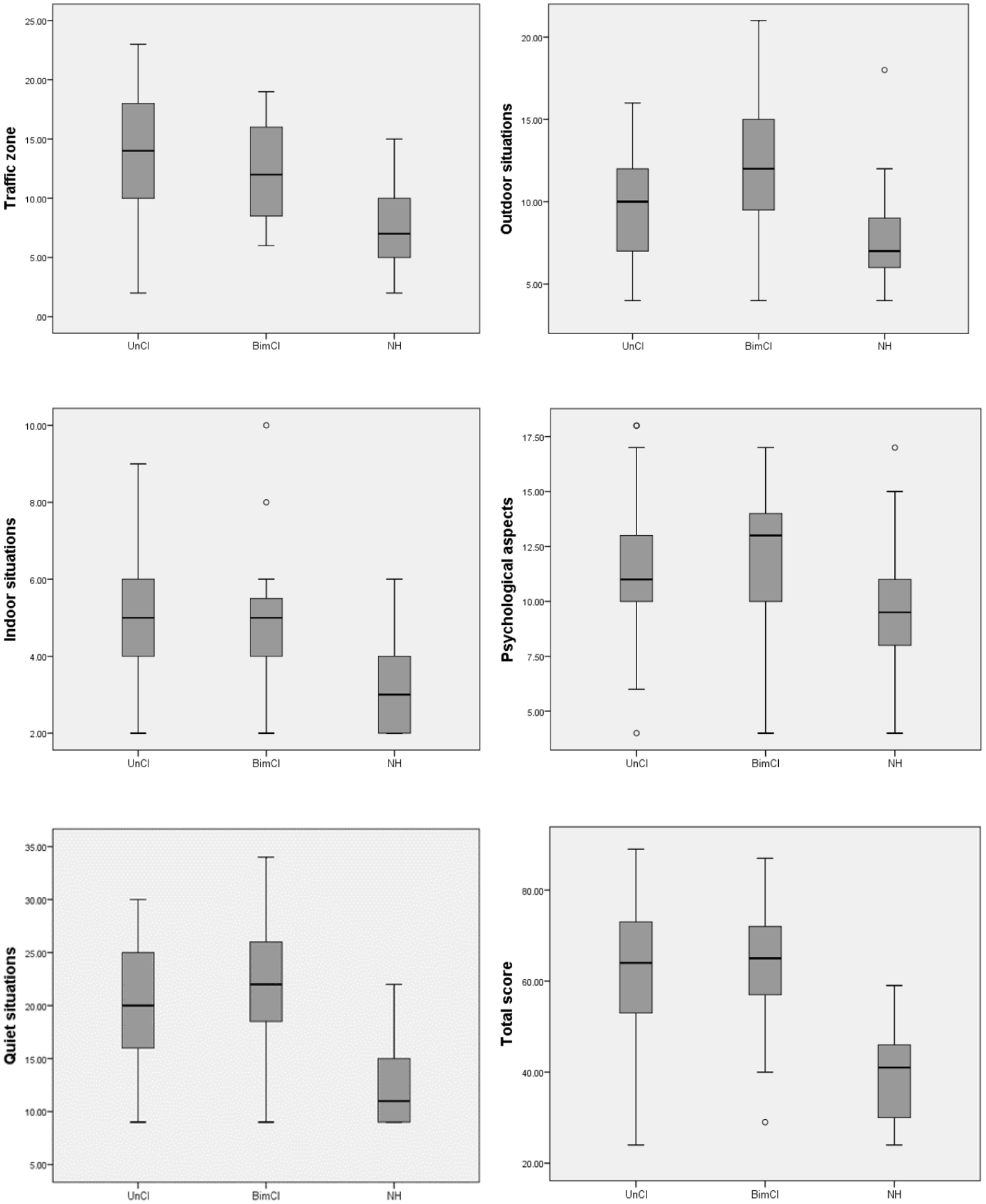
Comparison of auditory localization scores between unilateral CI, bimodal CI, and normal hearing groups.
Discussion
This study assessed participants’ localization abilities using the ALS, a scale that focuses exclusively on auditory localization. The ALS includes items evaluating localization performance in various noisy and quiet environments, as well as the psychological effects of localization and hearing difficulties. The findings showed that the NH group demonstrated significantly better localization abilities than both the UnCI and BimCI groups in noisy and quiet conditions. No significant differences were observed between the UnCI and BimCI groups. Additionally, the NH group reported significantly fewer psychological difficulties related to localization and hearing challenges, while the UnCI and BimCI groups exhibited comparable levels of psychological impact.
CIs successfully provide quality auditory input for individuals with severe to profound SNHL. However, it has been reported that speech recognition in noisy environments and sound localization abilities are limited, particularly in UnCI users, due to poor spectral resolution and the loss of temporal fine structure associated with envelope-based signal processing strategies. 13 Therefore, bilateral cochlear implantation is the most successful option for individuals with bilateral severe to profound SNHL who need access to bilateral auditory input. However, bilateral CIs are not commonly used for adult patients in our country due to their high cost and lack of coverage by social security, except in specific circumstances. 10 As a result, the number of adult bilateral CI users was insufficient for inclusion in the present study.
Devocht et al 2 noted that the current financial systems for adults in many countries around the world only support unilateral cochlear implantation. Additionally, an increasing number of CI users choose to retain their acoustic HA in the non-implanted ear, resulting in bimodal listening. Research has shown that individuals who use a bimodal configuration often experience improved hearing outcomes and enhanced quality of life compared with those who rely solely on a CI.14,15 In the present study, we included BimCI users who consistently used a HA in the contralateral ear following implantation. However, we found no significant differences in localization abilities between unilateral and bimodal users in either quiet or noisy environments. In contrast, Erdem and Çiprut 10 used the SSQ scale to compare the spatial hearing, speech perception, and hearing quality of bilateral, bimodal, and unilateral users. They found that there was a difference between all groups, and, contrary to our findings, bimodal users had better localization abilities compared to unilateral users. On the other hand, a study by Dorman et al 16 assessing sound source localization in a sound-isolated room with 13 speakers arranged in a 180° arc revealed that individuals with NH demonstrated superior localization abilities, while there was no significant difference in performance between bimodal and unilateral CI users. Variations in study design, participant characteristics, and evaluation methods may account for these differing results across studies.
Although the studies in the literature stated that hearing improvements among these patients are heterogenous, it was known that bimodal stimulation supports bilateral processing. According to Holtmann et al, 3 one of the main reasons for variable outcomes is the lack of optimal adjustment between the CI and HA. They emphasized that HA and CI should be fitted concisely to achieve the best possible results, but in the majority of cases, HA and CI are fitted separately. In our study, the HA and CI of bimodal participants were also fitted separately. Furthermore, the study does not include the strategies used in fitting. This aspect is acknowledged as one of the limitations of the present study. Another important variable that affects the outcomes of bimodal users is the functional residual hearing in the non-implanted ear. Although some studies have shown that residual hearing in the contralateral ear has a minimal effect on localization abilities, 16 bimodal stimulation still provides low-frequency temporal fine structure information and some degree of binaural hearing. 17 A limitation of the current study is the lack of detailed audiometric data describing the residual hearing of BimCI users in the hearing-aid ear. As a result, group classification was based solely on documented and clinically confirmed HA use. This limitation should be considered when interpreting the findings. Additionally, the BimCI group was smaller than the NH and UnCI groups. Since the importance of bimodal hearing has only recently been recognized in our country, most adult CI users either do not use HAs in the contralateral ear post-implantation or use them inconsistently. Consequently, the number of BimCI users was limited in our sample. Future research involving larger samples of BimCI and bilateral CI users will enhance the generalizability of the findings.
Even though this study has some limitations, it has also strengths. Few studies in the literature focus exclusively on localization skills in adult CI users. As a result, it was expected that the findings would contribute to the literature. Furthermore, the fact that there was no difference in demographic features between the NH, UnCI, and BimCI groups, and that the BimCI and UnCI groups had similar audiological characteristics, confirms the homogeneity between the groups and strengthens the reliability of the findings. Moreover, the study was enhanced by the inclusion of individuals with NH in order to compare the localization skills of UnCIs and BimCIs users with those of individuals with normal auditory systems.
As a conclusion, the findings of this study indicate that individuals with NH outperformed both BimCI and UnCI users in auditory localization tasks. In our sample, bimodal and unilateral users achieved similar outcomes; however, the lack of detailed audiological data from the non-implanted ear limits the interpretation regarding the effectiveness of bimodal stimulation in supporting binaural hearing. Bimodal hearing may offer some binaural cues, but more efforts are required to enhance hearing outcomes and subjective benefit. In addition, considering the findings of this study, we recommend that scales and questionnaires based on individuals’ experiences should be included in evaluations to acquire more understanding of the needs of CIs users.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.