
Abstract
Objective:
Evaluation of the clinical efficacy and safety of finafloxacin otic suspension in 2 Phase III clinical trials, in patients 6 months or older, reflective of the populations at risk for acute otitis externa (AOE).
Methods:
Two identical multicenter, randomized, double-masked, vehicle-controlled prospective Phase III studies in which 1234 patients (≥6 months) with AOE of presumed bacterial origin were randomized at 128 sites in the United States and Canada. Patients received finafloxacin otic suspension or vehicle twice daily for 7 days. The primary efficacy endpoint was the proportion of patients with clinical cure (resolution of tenderness, erythema and edema) on day 11 in the pathogen positive subset of the intention to treat (ITT) population.
Results:
Patients of the pathogen positive subset of the ITT population treated with finafloxacin had a clinical cure rate of 70.2% on day 11 (test of cure visit, ToC) compared to 36.6% in the vehicle group (P < .0001). A comparable effect was observed in the ITT population (finafloxacin 71% cure vs vehicle 49.8%). Finafloxacin eradicated the most common AOE pathogens with high efficiency: 89% for Staphylococcus aureus and 85.3% for Pseudomonas aeruginosa (39.2% and 26.8% in the vehicle group, respectively). Median time to cessation of ear pain was 3.5 days in the finafloxacin group versus 7.0 days in the vehicle group (P < .0001), and thus markedly shorter than durations reported for other otic therapies. Finafloxacin had a safety profile comparable to that of vehicle. Adverse events–primarily ear pruritus, ear discomfort, and dizziness–occurred at similar rates in both groups.
Conclusions:
Finafloxacin otic suspension was statistically superior to vehicle in clinical cures, pathogen eradication, and median time to ear pain resolution. It also demonstrated high efficacy against the primary AOE pathogens, S. aureus and P. aeruginosa, including fluoroquinolone-resistant pathogens. Finafloxacin was well-tolerated with a safety profile equivalent to vehicle.
Clinical trial registry name:
ClinicalTrials.gov;
Identifier:
NCT01535599 and NCT01535560
Keywords
Introduction
Acute otitis externa, usually caused by a bacterial infection of the external auditory canal, occurs in a low pH environment (pH 4.2 to 5.6). 1 It may result in diffuse cellulitis and can involve underlying structures along with the skin of the pinna and regional lymph nodes. 2 AOE, also known as “swimmer’s ear,” is common and associated with significant healthcare costs and clinician time. 3
Current guidelines for treatment of AOE in North America 4 emphasize eradication of P. aeruginosa and S. aureus as the predominant pathogens and identify topical fluoroquinolones, aminoglycosides, and/or polymyxin B for empiric treatment. Two meta-analyses suggest that quinolone-containing ear drops resulted in (i) higher microbiological eradication rates,5,6 defined as absence of the pathogen on culture, and (ii) higher clinical cures rates, defined as resolution of clinical symptoms on follow-up 6 , compared with combination drugs not containing quinolone.
The diagnosis of AOE is usually based primarily on physical examination. The predominant symptoms are tenderness 3 and pronounced pain7,8 which are associated with moderate to severe AOE.
One additional objective of these studies was to determine whether finafloxacin accelerates the resolution of otalgia compared with other available ear drops. In previous trials, median time to cessation of ear pain was 5 days for Ciprodex (ciprofloxacin 0.3%/dexamethasone 0.1% otic suspension) and Ciloxan (ciprofloxacin 0.3% otic solution), 9 6 days for Cipro HC (ciprofloxacin 0.2%/hydrocortisone 1% otic suspension), 10 and 8 days for Otiprio (ciprofloxacin 6% otic suspension), 11 whereas finafloxacin provided pain relief after only 3.5 days.
Finafloxacin, an advanced-generation fluoroquinolone, has demonstrated a potent effect on otalgia and proven broad-spectrum activity against key AOE pathogens, including fluoroquinolone-resistant strains.
Methods
Study Design
Between March 2012 and May 2013, 2 identical, prospective, multicenter, randomized, double-masked, vehicle-controlled trials were conducted to demonstrate superiority of finafloxacin versus vehicle for the cure of AOE. The diagnosis of AOE was based on clinical observation and presumed bacterial origin in at least 1 ear. The patients were evaluated at each of the 4 visits on Day 1 (Baseline), Day 3 (on-therapy visit), Day 8 (end of therapy visit) and Day 11 (ToC). Treatments were administered as 4 drops in the affected ear(s) twice daily for 7 days. For patients requiring an otowick, the initial dose was doubled to 8 drops, followed by the standard dosing regimen.
Up to day 11, patients reported their pain medication and ear pain twice daily. On day 8, patients ≥8 years completed a treatment satisfaction questionnaire.
Numerical scores for AOE symptoms (0 = none, 1 = mild, 2 = moderate, 3 = severe) of tenderness, erythema, and edema were assigned and summarized at each visit.
Patients deemed treatment failures received Ciprodex as a rescue treatment option or an appropriate alternative therapy at the investigator’s discretion.
Culture-positive patients had at least 1 bacterial organism at baseline from their affected ear(s). If this organism was P. aeruginosa and/or S. aureus, patients were assigned to the pathogen-positive ITT subset.
Detailed inclusion/exclusion criteria are available at https://clinicaltrials.gov/study/NCT01535560?term=NCT01535560&rank=1
Institutional Review Board (Schulmann Associates, Cincinnati, Ohio; IRB00000971) approval was obtained, all participants or guardians provided written informed consent prior to enrollment.
Study Outcomes
The primary efficacy endpoint was the proportion of patients with clinical cure on day 11 in the pathogen-positive ITT subset as defined by a sum of the numerical score of 0 for the 3 signs and symptoms of AOE on day 11.
The secondary efficacy endpoints were: (i) proportion of patients with microbiological success on day 11, defined by the absence of all pretherapy bacteria and (ii) the median time to cessation of ear pain as reported by the patient, defined as the first time point at which ear pain was absent and did not reoccur.
Study Drug
Finafloxacin otic suspension 0.3% (tradename Xtoro) is a sterile, stable, preserved suspension adjusted to pH 6.0. The composition of the vehicle was identical to finafloxacin otic suspension but without a solubilizing agent and finafloxacin (0.3%) as the active substance, both were delivered in identical opaque bottles.
Statistical Methods
All statistical analyses were performed using SAS® software (SAS Institute; Cary, NC). Data of the 2 independent clinical trials were pooled. The primary analysis set for all primary, secondary, and supportive endpoints was the pathogen-positive ITT subset. The primary objective of this analysis was to compare finafloxacin with vehicle for clinical cure at TOC (day 11). The null hypothesis stated that there is no difference in the proportion of patients with a clinical cure on day 11 (TOC) between both treatment groups, versus the alternative that there is a difference. Hypotheses testing was 2-sided with alpha of .05. The 2-sided Fisher’s Exact Test method was used for the calculation of the corresponding P-values.
Sample Size
Based on previous AOE studies a 56% pathogen-positive rate was assumed at baseline. Therefore, the randomization of at least 500 patients per study was planned to obtain at least 280 patients in the pathogen-positive ITT subset at baseline. The safety and tolerability of the study medication was evaluated in all patients who received a study drug dose (safety analysis set). With an expected clinical cure rate of 74% for finafloxacin at Day 11 and ≥280 pathogen-positive ITT patients, each of the study had approximately 90% power to detect a treatment difference of 20% points between finafloxacin and vehicle in the clinical cure rate at Day 11. The combined studies (a total of ≥560patients) had approximately 90% power to detect a treatment difference of 13% between finafloxacin and vehicle in the clinical cure rate at Day 11.
Randomization
At each study center, patients were enrolled and randomized at the Day 1 visit according to a sponsor-provided schedule. Numbers for consecutive randomization were generated to assign patients randomly to treatment groups in the planned ratio. Treatment was double-blind: neither patients nor investigators were aware of the assigned treatment.
Results
Study Population and Baseline Data
Across investigational centers in the US, Puerto Rico and Canada, a total of 1242 patients were randomized. Figure 1 describes the characteristics of the patient disposition. 560 patients–292 treated with finafloxacin and 268 treated with vehicle–who received study medication and were pathogen-positive at baseline (S. aureus and/or P. aeruginosa) formed the primary analysis subset.
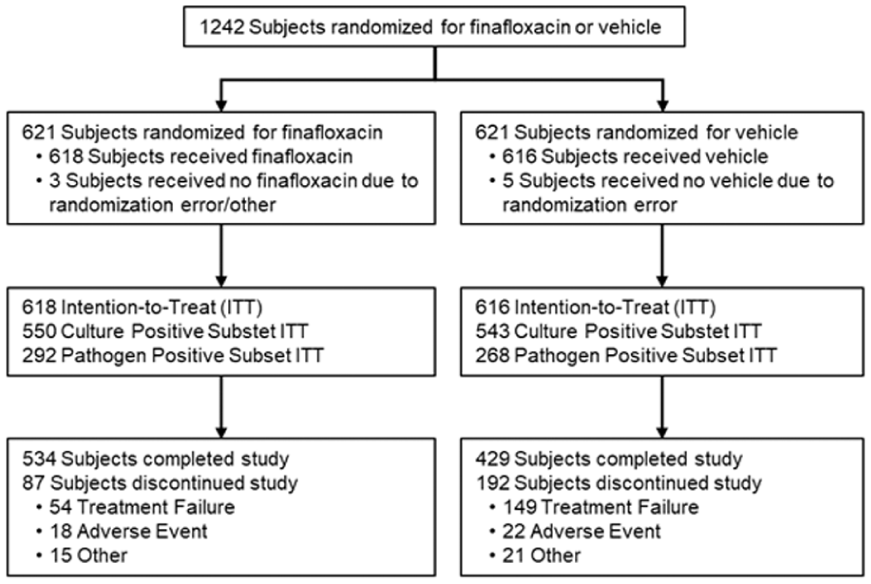
Study design and patient disposition.
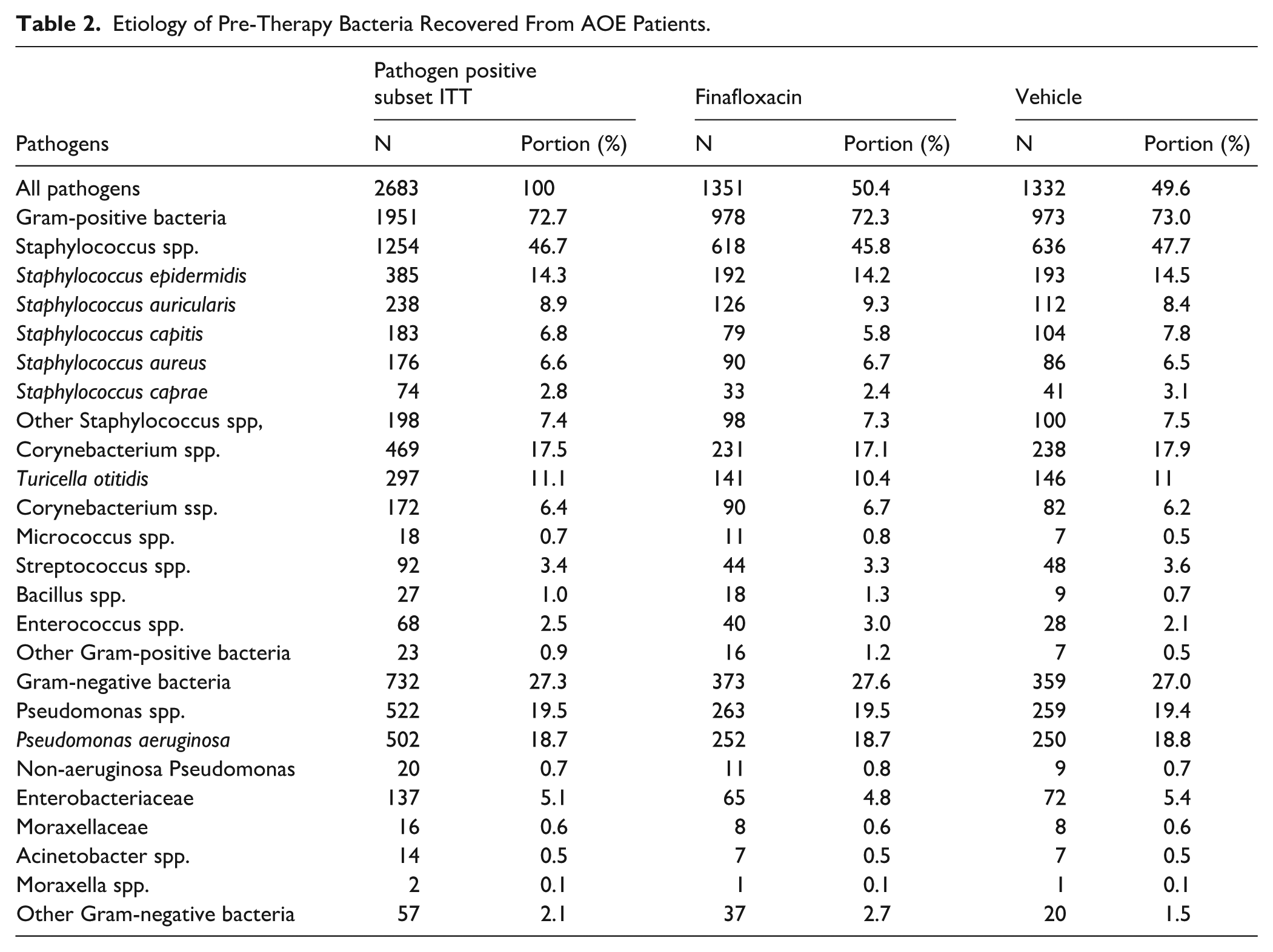
No relevant differences in demographic and baseline characteristics (Table 1) nor in pre-therapy bacteria isolated from the patient’s ears (Table 2) were observed between treatment groups.
Demographic Characteristics* By Treatment–Pathogen Positive Subset of the ITT.
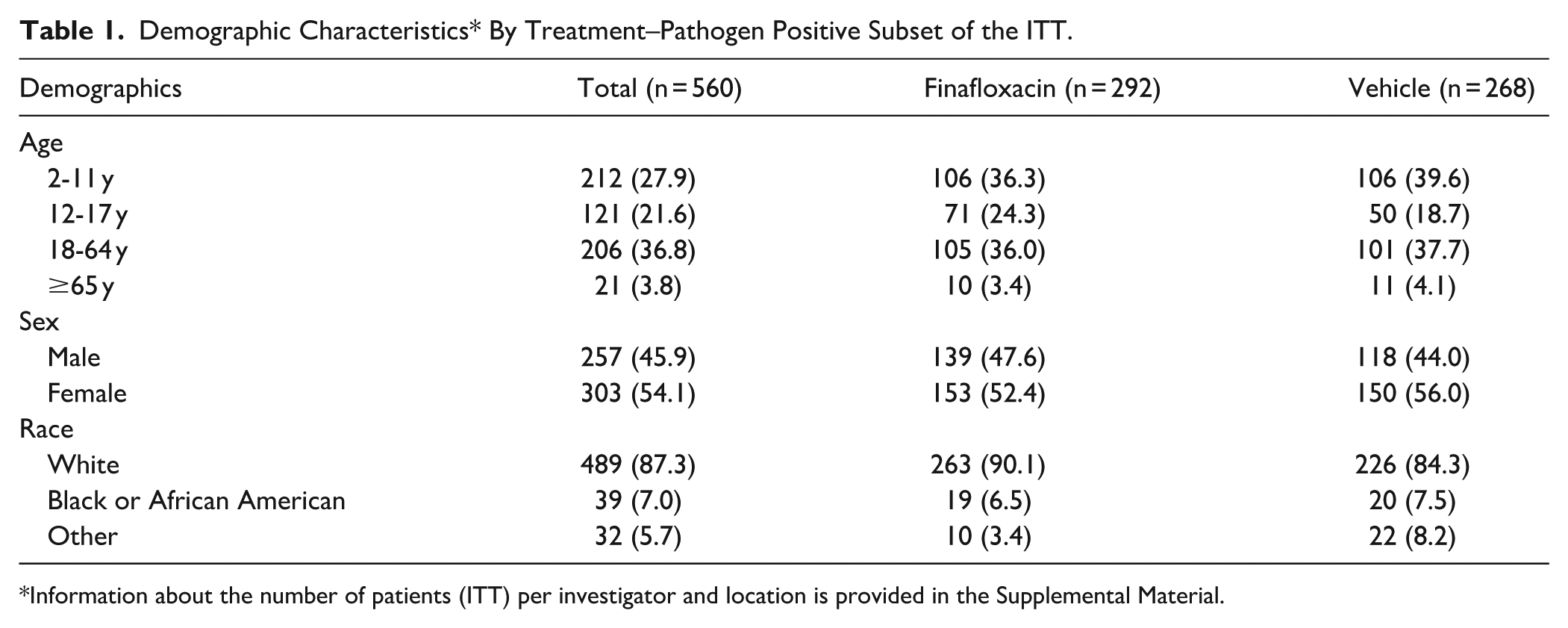
Information about the number of patients (ITT) per investigator and location is provided in the Supplemental Material.
Etiology of Pre-Therapy Bacteria Recovered From AOE Patients.
Unless stated otherwise, all following analyses were conducted on day 11 in the pathogen-positive ITT subset.
Of all patients, 41.8% of the patients had right-ear involvement only, 40% had left-ear and 18.2% had bilateral infections. 72.7% of the 2683 pathogens isolated from the ears of the patients were Gram-positive bacteria and 27.3% Gram-negative. Pseudomonas spp. dominated the Gram-negative isolates with 71.3% (522 of 732), whereas 46.7% (1254 of 1951) of the Gram-positives were Staphylococcus spp.
Clinical Cure and Symptoms
Finafloxacin was statistically superior to vehicle as complete AOE symptom resolution was achieved in 70.2% (205 of 292) of the patients compared to 36.6% (98 of 268) of the patients in the vehicle group (P < .0001; Table 3). A significant difference was observed on day 8 with clinical cures of 57.9% (169 of 292) for finafloxacin and 26.5% (71 of 268) for vehicle (P < .0001). This difference was not significantly affected by age or gender of the patients.
Clinical Cure and Microbiological Success Rate at Day 11 for ITT, Culture Positive Subset and Pathogen Positive Subset.
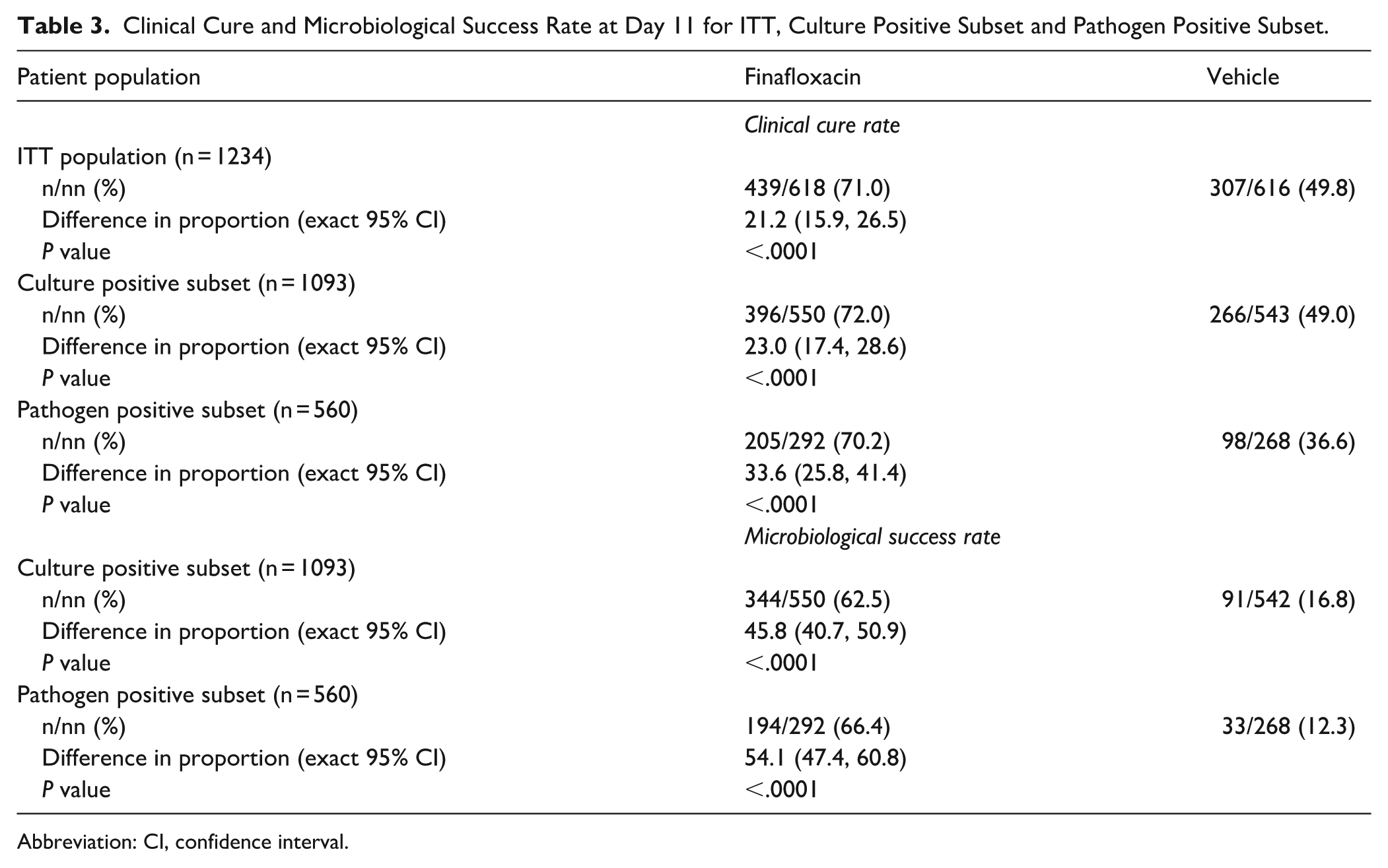
Abbreviation: CI, confidence interval.
The use of an otowick for 27.1% of the patients in the finafloxacin group and 30.6% in the vehicle group had no apparent effect on the clinical cure rates. For patients treated with finafloxacin 156 of 216 patients (72.2%) without an otowick had a successful clinical cure compared to 49 out of 79 patients with an otowick (64.5%; P = .24). Clinical cure rates in the vehicle group were 36.1% (66 of 183) without and 37.6% (32 of 85) with an otowick (P = .89). In the overall ITT population, clinical cure was 71% for finafloxacin versus 49.8% for vehicle (Table 3)
Microbiological Outcomes
Microbiological success at day 11 (TOC) was defined as the absence of all pretherapy bacteria in the culture. From the 560 patients in the pathogen positive subset of the ITT, 66.4% (194 of 292) of the patients in the finafloxacin group compared to 12.3% (33 of 268) of the patients in the vehicle group achieved microbiological success at the TOC visit (Table 3).
Additional analyses were conducted to determine the clinical cure and eradication rates for the primary pathogens S. aureus and P. aeruginosa. The microbiological success on day 11 in the finafloxacin group was 89.0% (73 of 82) for S. aureus and 85.3% (197 of 231) for P. aeruginosa compared to 39.2% (29 of 74) and 26.8% (60 of 224) in the vehicle group, respectively. The eradication of both pathogens by finafloxacin exceeded 89% in clinically cured patients and was markedly higher than vehicle (32.5% for S. aureus and 20.1% for P. aeruginosa).
In total, 110 patients were infected with Gram-positive fluoroquinolone-resistant pathogens (5.6%). Finafloxacin achieved clinical cure and eradicated these pathogens in 86.8% (59 of 68) versus 54.8% in the vehicle group (23 of 42). Twenty-nine patients were infected with Gram-negative fluoroquinolone-resistant pathogens (4.0%). Finafloxacin achieved clinical cure and eradicated the pathogens in 100% (14 of 14) of these patients versus 26.7% in the vehicle group (4 of 15).
Table 4 displays the severity of the 3 symptoms of AOE as assessed by the physicians.
Frequency of AOE Symptom Severity During the Study Visits–Pathogen Positive Subset of the ITT.
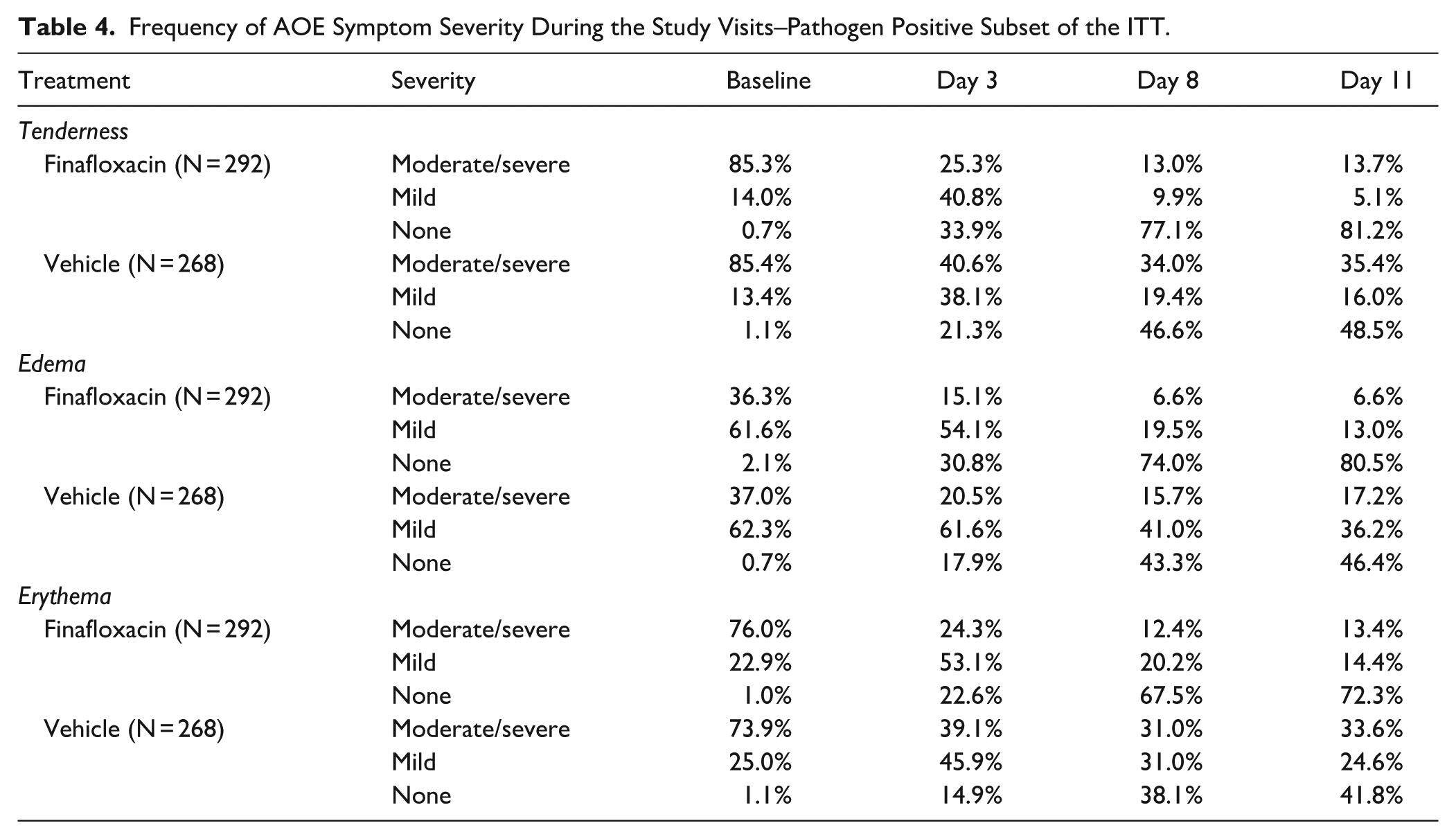
The study was well balanced between treatment groups at baseline with tenderness, followed by erythema and edema, with the highest frequency of moderate to severe rating. Each symptom was absent or reduced to mild in approximately 75% of the finafloxacin-treated patients on day 3, with further improvement by day 8. In the vehicle group, clinical improvements were lower at each assessment during the study.
Symptom Scores
The results of the combined clinical scores for the documented signs of AOE (tenderness, erythema, and edema) in both study groups are shown in Figure 2.
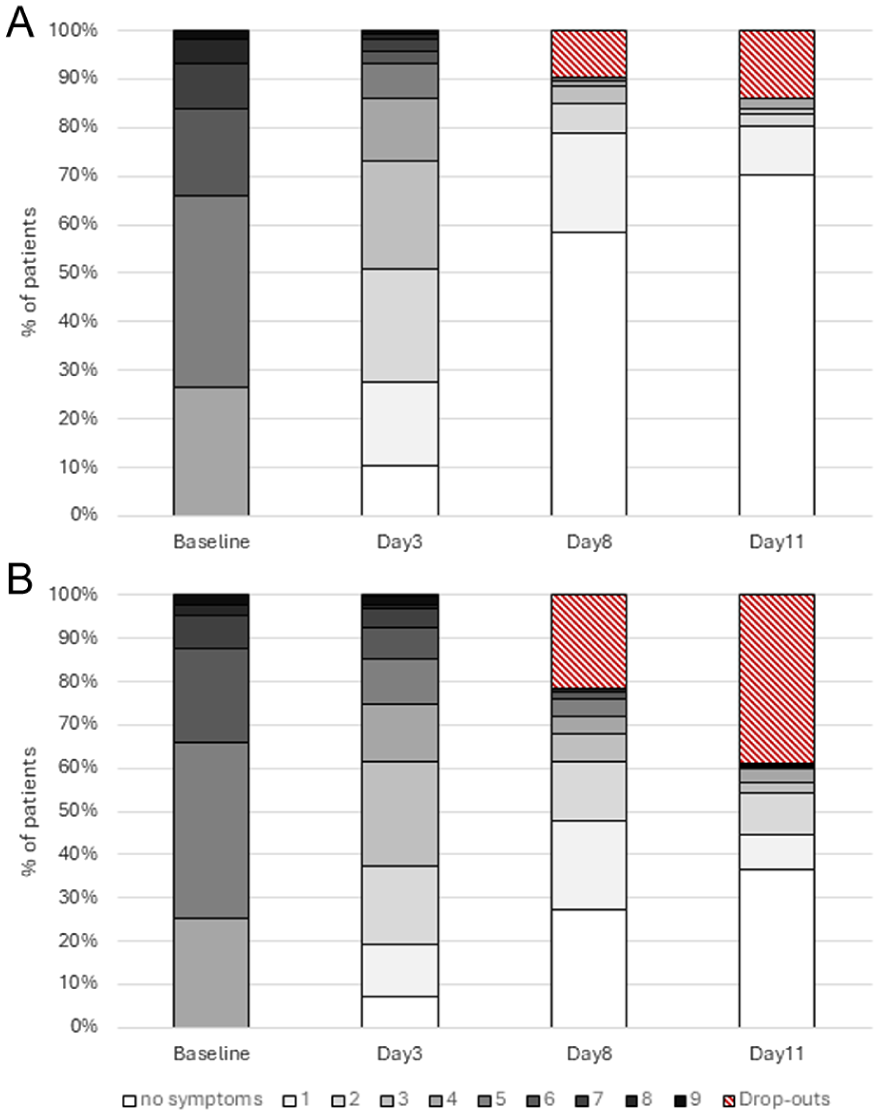
Course of patient symptom score (for all 3 symptoms combined) over time for finafloxacin (A) and vehicle (B)– pathogen positive subset of the ITT.
Total clinical symptom scores for tenderness, erythema, and edema were comparable at baseline, but differences emerged by Day 3, when 51% of finafloxacin patients had a total score ≤2% versus 37% of vehicle patients (Figure 2). On day 8, at the end of the therapy, 59% of the patients treated with finafloxacin had complete symptom resolution and 79% had a total symptom score of 1 or less, compared to 27% and 48% in the vehicle group. At the test of cure visit on day 11 these proportions were 70% versus 37% (symptom free) and 80% versus 45% (score ≤1). Overall, 39.2% of the pathogen-positive patients (105 of 268) from the vehicle group had discontinued the study, 84 of them due to treatment failure. In comparison 14.4% (42 out of 292) of the finafloxacin group discontinued the study, 30 of them due to treatment failure.
Pain Relief
Ear pain was reported by 95.1% (997 of 1048) of the ITT patients prior to treatment initiation or during the study. The median time to cessation of ear pain, the first time point that ear pain was absent and did not return, was 3.5 days in the finafloxacin group (n = 276) compared to 7.0 days in the vehicle group (n = 253; 95% CI: [2.0, 4.5]; P < .0001; Figure 3).
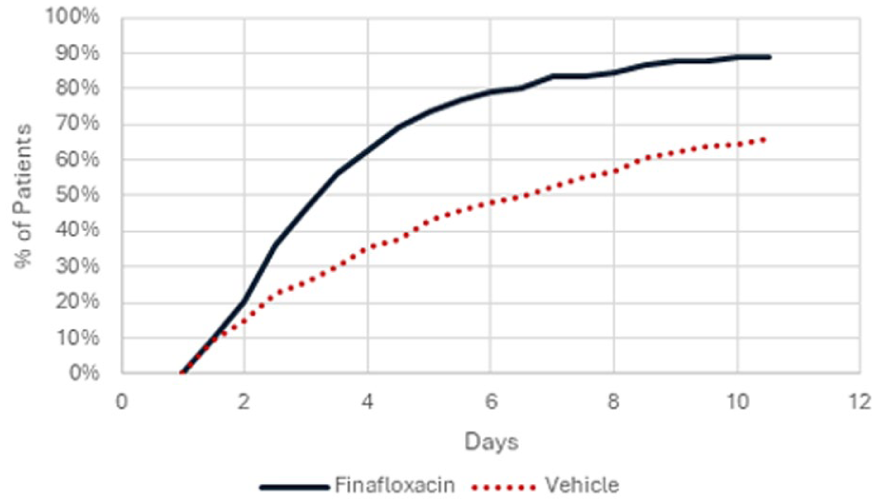
Time to cessation of ear pain – pathogen positive subset of the ITT.
Median time to cessation of pain in patients with clinical cure and/or pathogen eradication was 3 days in the 276 patients treated with finafloxacin (193 with clinical cure; 181 with pathogen eradication) and 4.5 days in 253 patients of the vehicle group (92 with clinical cure; 33 with pathogen eradication). For patients without pathogen eradication the median time to no pain was 4.5 days in the finafloxacin group (95 of 276) compared to 7.5 days in the vehicle group (220 of 253). Likewise, in patients without clinical cure the median time to no pain was 4.5 days in the finafloxacin group (83 of 276) and 10.5 days in the vehicle group (161 of 253).
1.5 days after initiation of treatment, 44% of the finafloxacin-treated patients reported that they were free of pain, and 3.5 days after initiation of treatment 76% of these patients were free of pain. Consequently, the median time to discontinuation of pain medication was 4.9 days in the finafloxacin group versus 7.1 days in the vehicle group, a difference of 2.2 days (P < .0001).
Within the finafloxacin group 88% of all patients were very satisfied or satisfied with the velocity of ear pain resolution versus 69.0% in the vehicle group (P < .0001) and they reported a significantly shorter time to resolution of symptoms like itching or a stopped-up feeling (each P < .0001).
Safety and Tolerability
In total, 190 patients in the safety set reported at least 1 adverse event: 91 (14.7%) in the finafloxacin group and 99 (16.1%) in the vehicle group. Of these, only 11 patients in the finafloxacin group and 7 in the vehicle group experienced adverse events that were assessed as related to the study drug. None of them were classified as serious (Table 5). Overall, 203 patients of the safety set (16.5%) discontinued the study due to a treatment failure, 54 (8.7%) of the finafloxacin group and 149 (24.2%) of the vehicle group.
Overall Frequency and Incidence of Adverse Events (≥1% in Any Treatment Group; Safety Analysis Set).
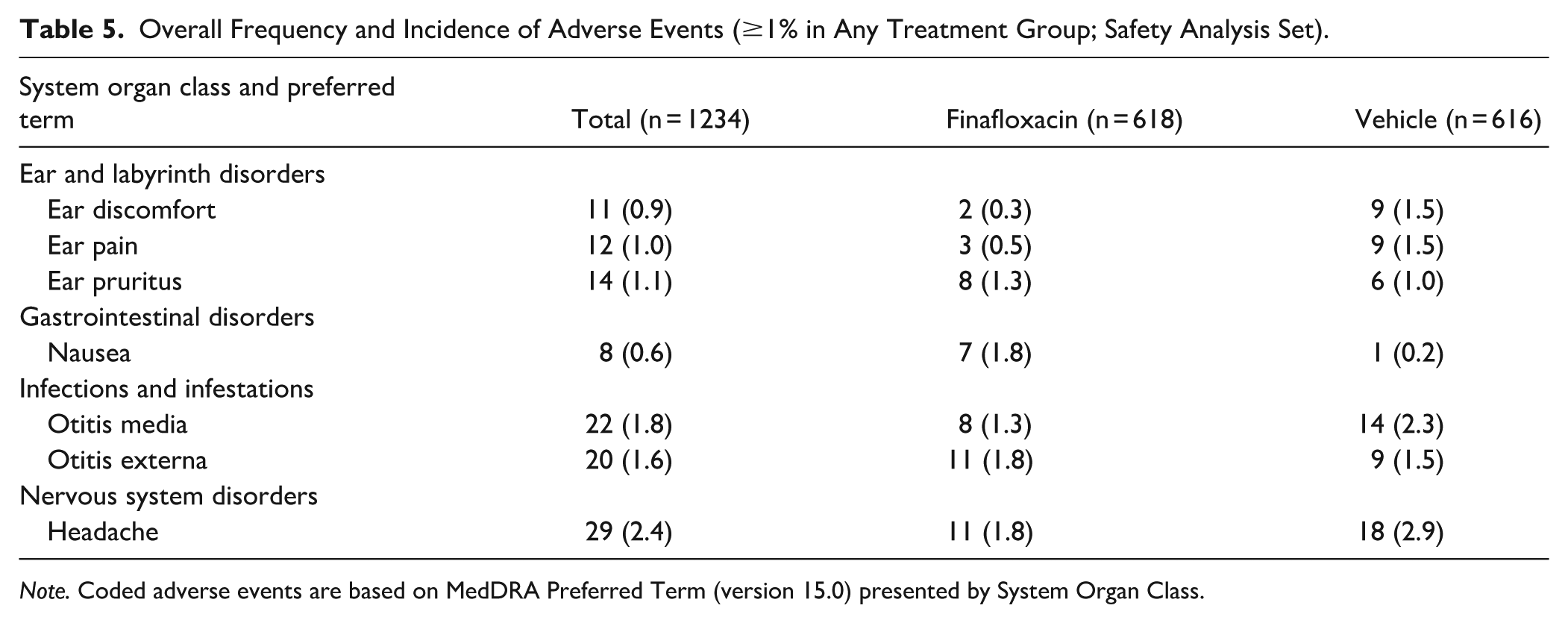
Note. Coded adverse events are based on MedDRA Preferred Term (version 15.0) presented by System Organ Class.
Discussion
This is the first Phase III clinical study showing the efficacy of the novel fluoroquinolone finafloxacin for treating AOE, which is caused primarily by bacterial pathogens. This clinical study demonstrates that finafloxacin is associated with statistically significantly higher rates of therapeutic cure, pathogen eradication, and significantly faster cessation of ear pain and a good safety profile independent of the absence or presence of an otowick when compared with patients treated with the vehicle.
Previous studies identified P. aeruginosa and S. aureus as the most common pathogens in AOE. From 2683 bacteria isolates found in ear cultures in this study 27.3% (n = 732) were Gram-negative and 72.7% (n = 1951) were Gram-positive, consistent with the bacterial etiology of AOE reported in previous studies. Pseudomonas spp. dominated the Gram-negative isolates with 71.3% (522) and 46.7% (n = 1254) of the Gram-positives were Staphylococcus spp. Likewise, Pseudomonas aeruginosa isolates from infected ears show a tendency toward increasing fluoroquinolone resistance. 12
Non-clinical studies of finafloxacin have demonstrated its broad antibacterial spectrum and rapid bactericidal activity against both Gram-positive and Gram-negative species being active against ciprofloxacin resistant isolates as well in acidic environments typical of an infected ear canal.13-16
Patients with bacterial AOE present with rapid onset of ear canal inflammation, which results in severe otalgia, itching, canal edema, canal erythema, and otorrhea. 17 Finafloxacin eradicated the causative AOE pathogens with high efficiency. Patients not treated with the antibiotic had significantly higher rates of persistent pathogens in the ear canal resulting in significantly slower symptom relief, higher rate of patients with persistent symptoms at the end of the study and a high percentage of patients discontinuing the study (38.8% vehicle vs 14.4% finafloxacin). Besides pain, tenderness and erythema were the most severe and frequent clinical symptoms at the start of the study and these symptoms persisted for more than one third of the patients at the end of the study in patients treated with vehicle (vs 14% finafloxacin group).
Ear pain is a dominant clinical finding in AOE patients. Intense pain, usually associated with moderate to severe AOE is often the reason patients seek medical assistance. 8 In this study, 95.1% of the patients reported ear pain prior to treatment initiation or during the study. A 2014 update of the clinical practice guidelines 4 identifies topical fluoroquinolones, aminoglycosides or polymyxin B for empiric treatment. Two meta-analyses suggest that quinolone drops resulted in higher rates of microbiological eradication5,6 and clinical cures 6 than the other drugs defined as the absence of pathogen on follow up, and resolution of clinical symptoms. These findings may result in cost savings because the indirect costs of AOE are likely to be substantial because of severe and persistent clinical symptoms, for example, otalgia which limit activities, especially work. 4 As demonstrated in the current study, finafloxacin has a major impact especially on otalgia; leading to a rapid cessation of ear pain within 3.5 days compared to 7 days in the vehicle group. Interestingly, finafloxacin reduces ear pain irrespective of clinical or microbiological success when compared with the vehicle. In comparison to other otic agents, the ear pain reduction by finafloxacin in AOE patients appears to be especially quick.
In summary, finafloxacin is characterized by superiority to vehicle with regard to clinical cure, microbiological eradication and cessation of ear pain. The significant shortening of ear pain has not been demonstrated for any other otic antibiotic to date. The fact that finafloxacin also reduces ear pain in patients who are not clinically cured, or have persistent pathogens, confers anti-inflammatory properties to the antibiotic. The desirable characteristics of finafloxacin, in combination with low systemic exposure and absence of ototoxicity make finafloxacin an outstanding antibiotic for topical treatment of AOE.
Conclusion
Finafloxacin is an effective new fluoroquinolone for the treatment of AOE, with high efficacy against the causative pathogens, rapid improvement of clinical symptoms and a high safety index. The rapid pathogen eradication and resolution of AOE symptoms by finafloxacin should support patient compliance, reduce the development of chronic infections, and meet the expectations of healthcare providers.
Supplemental Material
sj-docx-1-aor-10.1177_00034894261453726 – Supplemental material for Efficacy and Safety of Finafloxacin Otic Suspension, 0.3% for the Treatment of Acute Otitis Externa: Results from two Phase III Ranomized Clinical Studies
Supplemental material, sj-docx-1-aor-10.1177_00034894261453726 for Efficacy and Safety of Finafloxacin Otic Suspension, 0.3% for the Treatment of Acute Otitis Externa: Results from two Phase III Ranomized Clinical Studies by Ann Edmunds, Christine Bentley, Mark Lückermann, Bernard Voet and Andreas Vente in Annals of Otology, Rhinology & Laryngology
Footnotes
Ethical Considerations
The clinical studies were conducted in accordance with the principles of the Declaration of Helsinki, and in compliance with the International Conference on Harmonization (ICH) E6 Good Clinical Practice (GCP) guidelines. Institutional Review Board (Schulmann Associates, Cincinnati, Ohio; IRB00000971) approval was obtained on 2-24-2012. All participants (or their legal guardians) provided written informed consent prior to enrollment in the study.
Consent to Participate
All participants provided written informed consent prior to enrollment in the study.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christine Bentley, employee: MerLion Pharmaceuticals GmbH; Ann Edmunds, Speakers Bureau for Regeneron and Sanofi; Mark Lückermann, employee: MerLion Pharmaceuticals GmbH; Bernard Voet, statistical consultant for MerLion Pharmaceuticals GmbH; Andreas Vente, employee and shareholder: MerLion Pharmaceuticals GmbH
Data Availability Statement
The datasets generated during and/or analyzed during the current study are publicly not available but on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.