
Abstract
Objective:
Endotracheal intubation can cause laryngeal injury, with clinical presentation ranging from transient hoarseness to persistent vocal cord immobility. This study examines the incidence, clinical features, and outcomes of post-intubation laryngeal injuries following procedures traditionally considered low risk for such complications.
Methods:
We conducted a retrospective review of adult patients who underwent tracheal intubation for surgical procedures between May 1, 2018, and December 31, 2024, and subsequently presented with postoperative laryngeal injury–related symptoms. Patients who underwent cardiothoracic, thyroid, parathyroid, or anterior cervical spine procedures were excluded. We reviewed patient demographics, airway and intubation characteristics, treatments, and clinical outcomes.
Results:
Among 267 824 patients undergoing 454 924 general anesthetics, 30 developed postoperative laryngeal injury (6.6/100 000; 95% CI 4.5–9.4) which did not resolve spontaneously and required laryngology evaluation. Of these 22 (67%) had well defined movement abnormalities: unilateral (n = 15) and bilateral vocal cord immobility (n = 1), unilateral hypomobility (n = 4), bilateral hypomobility (n = 1), combined unilateral vocal cord immobility with contralateral hypomobility (n = 1), and 11 (33%) had no movement abnormality. Twenty-one (64%) were intubated via video laryngoscopy. Follow-up was available for 21 patients (70%) with a median [IQR] duration of 12 [9-35] months; 15 (72%) showed partial improvement without complete resolution, while 6 showed no improvement.
Conclusion:
Laryngeal injury following general anesthesia with tracheal intubation is a uncommon complication. In our series, approximately two-thirds of patients had identifiable injuries, while one-third exhibited no structural abnormality. While 75% of patients demonstrated partial symptomatic improvement, however, complete resolution was not observed in any of the patients who received follow-up in our institution, underscoring the severity of this complication.
Keywords
Introduction
Laryngeal injury (LI) is a rare complication after anesthesia with tracheal intubation, and may range from transient hoarseness to complete vocal cord immobility (VCIM).1,2 LI often results from surgical trauma to the branches of vagus nerve, 3 particularly during thyroid, parathyroid, 4 cardiothoracic,5,6 and anterior cervical spine procedures. 7 However, it can also occur after procedures considered to be low-risk for this surgical complication. 8
The mechanism of LI in these cases differs from that of direct laryngeal nerve injury, and therefore long-term outcomes may be expected to be differ. Specifically, LI occurring during laryngoscopy for tracheal intubation, or procedures with potential for mechanical trauma to laryngeal structures (such as rigid bronchoscopy, esophagogastroduodenoscopy, or mediastinoscopy), may result in compression-related trauma to laryngeal nerves. This can lead to neuropraxia, a milder form of peripheral nerve injury characterized by transient disruption of nerve conduction without substantial structural damage.
Transient hoarseness following endotracheal intubation is relatively common and is usually resulting from minor laryngeal irritation, with self-limited symptoms and typical recovery within 3 to 4 days.9,10 In contrast, the present report highlights the Mayo Clinic’s, Rochester, Minnesota, experience with patients who developed non-resolving LI following procedures considered to be low-risk for direct surgical injury to laryngeal nerves and who subsequently required referral to a specialized laryngological clinic. We describe the incidence and types of these injuries, outline the management strategies employed, and report patient outcomes, thereby providing further insights into prognosis and recovery.
Methods and Materials
The Mayo Clinic Institutional Review Board approved this study. In accordance with Minnesota State Statute 25-002285, we included only patients who provided written authorization for research use of their medical records.
We electronically interrogated the Mayo Clinic, Rochester, Minnesota, electronic medical records to identify adult patients who underwent tracheal intubation for procedures requiring general anesthesia and subsequently presented to the laryngology clinic between May 5, 2018, and December 31, 2024, for evaluation of hoarseness, breathiness, voice fatigue, dysphonia, raspy voice or pain or discomfort when speaking. Patients who had thyroid, parathyroid, cardiothoracic, anterior-approach cervical spine surgeries, or similar procedures which carry high risk for surgical injury to laryngeal nerves, were excluded.
Electronic medical records were reviewed for demographics, perioperative variables, and airway management details. Anesthesia records were examined for intubation method (direct laryngoscopy [DL], video laryngoscopy [VL], fiberoptic intubaiton), difficulty encountered during intubation, and best glottic view during laryngoscopy. Laryngology records were reviewed for type of LI and timing of symptom onset, with symptoms categorized primarily as dysphonia, dysphagia, or pain. Vocal cord anatomy, mobility, and type of structural injury (eg, immobility, hypomobility) were assessed using flexible laryngoscopy and videostroboscopy. Treatments were recorded as conservative therapy (eg, voice therapy, antimicrobials), injection laryngoplasty, or advanced procedures (eg, thyroplasty, microflap surgery). Outcomes included resolution of LI, need for repeat therapeutic procedures, and clinical status at last follow-up (full vs partial recovery). Data were summarized using descriptive statistics.
Results
We reviewed medical records for 267 824 patients who underwent 454 924 procedures performed under general anesthetics with tracheal intubation. Of these 498 were referred to the laryngology clinic and these patients’ records were reviewed to identify cases of postoperative LI. We identified 30 patients who were diagnosed with postoperative LI, corresponding to an incidence of 6.6 LI cases per 100 000 anesthetics (95% CI, 4.5-9.4). Table 1 summarizes patient and surgical characteristics. Airway records noted ‘some difficulty with intubation’ in 2 patients while using DL. Among DL cases, the Mallampati score was III in 3 of 9 patients, whereas patients intubated with VL 9 of 20 patients were assessed as Mallampati scores of III or IV. Endotracheal size was reported in 15 male patients (3 [20%] had a 7.0 mm, 8 [53%] a 7.5 mm, 3 [20%] 8.0 mm, and 1 [7%] a double lumen 37 French endotracheal tube) and 14 female patients (1 [7%] 6.0 mm, 10 [71%] 7.0 mm, 2 [14%] 7.5 mm, and 1 [7%] 8.0 mm endotracheal tube). Duration of endotracheal intubation was documented for 29 patients (97%), with a median time of 415 minutes [IQR 136-696]. There were 9, 4, and 16 cases of LI for tracheal intubations lasting <3, 3-6, and >6 hours, respectively (Figure 1).
Characteristics of Patients with Postprocedural Laryngeal Injury.*
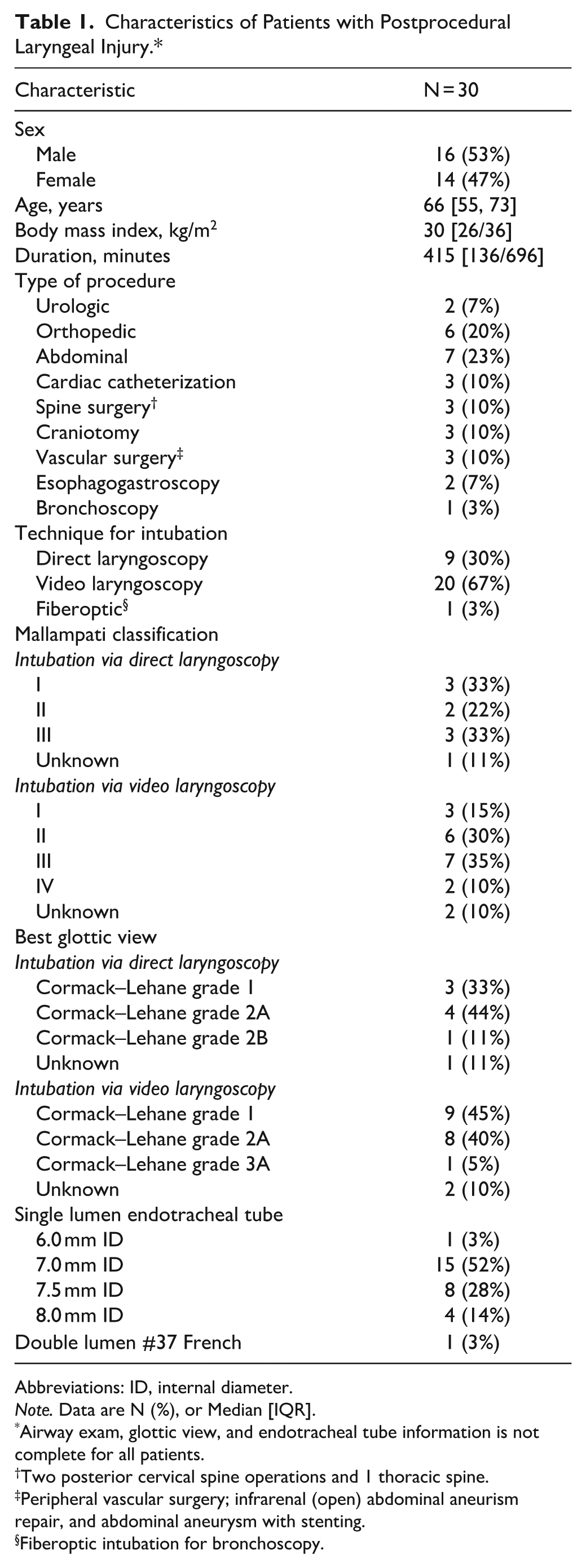
Abbreviations: ID, internal diameter.
Note. Data are N (%), or Median [IQR].
Airway exam, glottic view, and endotracheal tube information is not complete for all patients.
Two posterior cervical spine operations and 1 thoracic spine.
Peripheral vascular surgery; infrarenal (open) abdominal aneurism repair, and abdominal aneurysm with stenting.
Fiberoptic intubation for bronchoscopy.
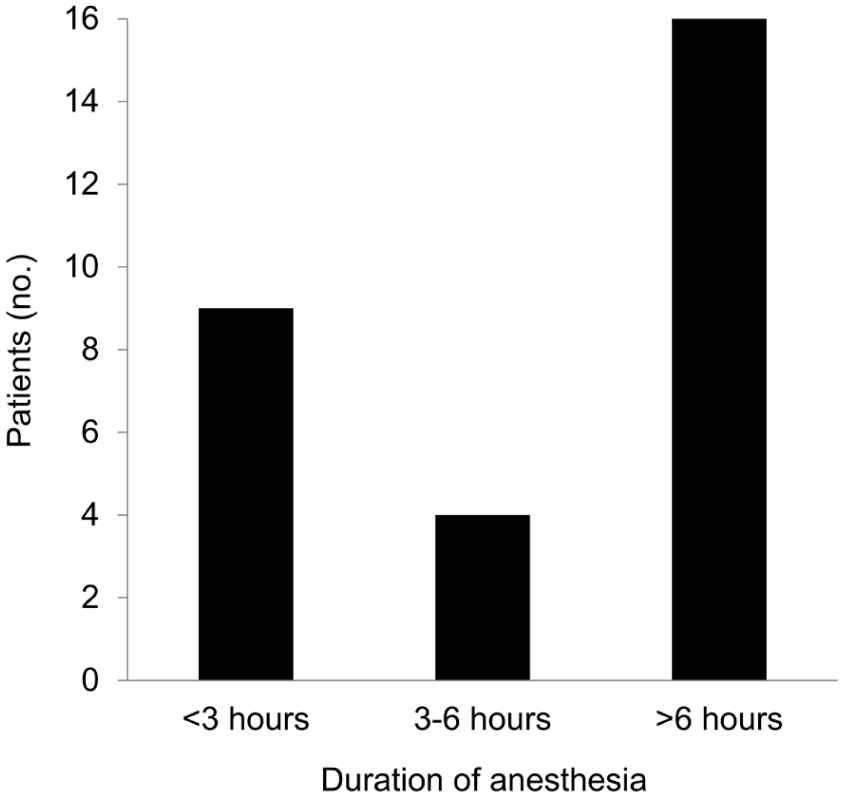
Frequency of laryngeal injury among patients stratified by tracheal intubation duration.
Supplemental Table details findings for all patients including relevant co-morbidities. Dysphonia was reported soon after tracheal extubation in all but 1 patient, who noted onset 1 week later. In addition to dysphonia, 4 patients (13%) reported dysphagia and 7 (23%) oropharyngeal pain. The laryngoscopic examination showed unilateral VCIM in 12 patients (40%), bilateral VCIM in 1 (3%), unilateral hypomobility in 4 (13%), bilateral hypomobility in 1 (3%), combined unilateral VCIM with contralateral hypomobility in 1 (3%), and no structural abnormality in 11 (37%). Supplemental Video shows unilateral vocal cord immobility in a 52-year-old man following intubation for an abdominal procedure.
The most common therapeutic intervention was hyaluronic acid injection laryngoplasty, performed in 12 patients (40%), including 1 who also received a triamcinolone injection: 8 (27%) required repeat injections. One patient with polypoid fullness of the unaffected vocal cord underwent laser ablation of the lesion during injection laryngoplasty of the injured cord. Fourteen patients (47%) received conservative treatments: 12 voice (40%), 1 swallowing (3%), and 1 physical therapy (3%). Two patients undergoing voice therapy were also treated with antimicrobials. One patient (3%) underwent both microflap excision of a polyp on 1 cord and triamcinolone injection of a scar on the other.
Follow-up was available for 21 patients (70%). Median [IQR] follow up for these patients was 12 [9-35] months, with range 1 to 57 months. Of those with available follow-up consultation, some improvement but no complete resolution was noted in 15 while 6 patients did not improve. Ten of 13 unilateral VCIM cases improved: 5 after multiple hyaluronic acid injections, 2 after a single injection, and 3 without injections. The single bilateral VCIM patient improved after repeated injections. Three of 5 with hypomobility improved, 2 with voice therapy and 1 without treatment. Only 2 of 11 patients without a structural diagnosis had follow-up; 1 improved with voice therapy, the other received antimicrobial therapy, but hoarseness did not improve. Nine patients (27%), all without structural abnormalities, were lost to follow-up after their initial visit.
Discussion
Severe non-resolving laryngeal injury following anesthesia with tracheal intubation remains an uncommon but clinically significant complication. In our series, 15 patients were diagnosed with either unilateral or bilateral VCIM, while 11 patients, despite persistent hoarseness or dysphonia, demonstrated no structural abnormalities on examination. Although some patients experienced partial improvement over time, of those with available follow up at the Mayo Clinic none achieved complete resolution of symptoms. These findings highlight the importance of individualized management, as permanent vocal dysfunction has a profound impact on patient quality of life.
Incidence of LI
In our case series, the incidence of severe LI was 6.6 per 100 000 cases. The rates of LI vary mostly due to differences in study designs and patient populations, which complicates their direct comparison. For example, Lim et al 11 reported a postoperative VCIM incidence of 43 per 100 000 cases, from a cohort that included surgeries that are high-risk for laryngeal nerve(s) injury such as thyroid, parathyroid, and thoracic procedures. Similarly, Kikura et al, 12 reported a rate of 77 per 100 000 cases following anesthesia with direct laryngoscopy, while Yamanaka et al, 13 in a prospective study of 3093 patients undergoing general endotracheal anesthesia, identified 25 patients with LI symptoms, of whom only 4 were confirmed to have VCIM (1.3 per 100 intubations). Several factors may explain why the incidence in our study was substantially lower. First, referral bias: our cohort was limited to patients presenting to a quaternary laryngology clinic, potentially underrepresenting milder or self-limited cases managed in primary care settings. Second, case selection: we excluded procedures with inherently higher risk of vagal nerve injury, such as thyroid, parathyroid, anterior cervical spine, and cardiothoracic surgery, which likely lowered the observed incidence.
Risk Factors for LI
Difficulty in airway management, with multiple laryngoscopy attempts, can contribute to oropharyngeal trauma.14,15 In our series, difficulty with airway management was documented in only 2 patients, both by using DL but the medical records did not provide details regarding the nature of these challenges. The majority of patients in our cohort were intubated using VL, which is considered a less traumatic technique than DL, as it provides improved glottic visualization and facilitates intubation in difficult airway scenarios.16-19 A Cochrane systematic review 20 analyzing 22 studies comparing VL and DL reported a reduction in airway injuries with VL (0.68 [95% CI 0.48, 0.96]). In recent years, our practice has increasingly favored VL for tracheal intubation, with approximately 70% of intubations managed with VL. Notably, despite being a superior technique for laryngoscopy VL is not devoid of potential for LI, as 67% of LI in our series occurred following VL. While VL drastically improves glottic visualization, the direction of the endotracheal tube across the glottic opening can pose challenges. VL intubation typically requires a stiff, L-shaped metal stylet, which, if improperly used, can cause laryngeal trauma due to the tube’s curvature and rigidity needed for a sharp anterior trajectory during endotracheal tube insertion. To minimize potential for LI, the stylet should be withdrawn before or simultaneously with advancement of the tube through glottic opening. Even after stylet removal, additional maneuvers—such as rotational (‘screw-in’) movements or application of cricoid pressure—may be necessary to align the tube with the tracheal axis, potentially contributing to injury.
Prolonged tracheal intubation has been associated by some reports with an increased risk of LI. Kikura et al, 12 demonstrated that the risk of VCIM was twofold higher in patients intubated for 3 to 6 hours and 15-fold in those intubated for more than 6 hours. Similarly, Santos et al, 21 reported higher rates of LI with longer intubation duration. In our study, the median intubation time was 415 minutes; however, despite the relatively long duration of intubation, no association was observed between intubation time and LI (Figure 1). This finding aligns with Shokri et al, 22 who reported that procedures exceeding 120 minutes were not associated with an increased risk of LI. Likewise, Mendels et al, 23 in a systematic review of laryngeal injuries after procedures lasting less than 5 hours concluded that, given the heterogeneity of LI, no clear association exists between intubation duration and risk of injury. Absence of association between duration of anesthesia and LI is suggestive of early mechanical injury (eg, rough intubation from laryngoscopy, improper use of rigid stylet) rather than injury caused by ischemia due to long-standing pressure (eg, high ‘riding’ cuff at glottic opening, too big endotracheal tube). In addition, procedures requiring large medical instruments competing in space with endotracheal tube (eg, gastroscope) or extrinsic pressure on nerves (eg, mediastinoscopy) may also contribute to laryngeal injury. In this series, 2 patients had undergone EGD procedures, in which mechanical trauma or pressure to the glottic region may have contributed to the development of LI. Thus, protracted presence of endotracheal tube though glottic opening is unlikely to be an isolated contributor to vocal cord irritation leading to laryngeal injury.
It has been demonstrated that the rate of postoperative sore throat and/or hoarseness decreases with the use of smaller endotracheal tubes.24-26 These complications are common after general endotracheal anesthesia, readily allowing for evaluation of risk and endotracheal tube size. In contrast, given the rarity of postoperative LI, existing literature is insufficient to assess for an association between ETT size and LI. 27 However, Shinn et al 28 was able to demonstrate that among critically ill intubated patients the risk for post-extubation LI increased with endotracheal tubes greater than 7.0 mm internal diameter. Amongst patients in this cohort where the size of the endotracheal tube was reported, 3 of 15 male patients and 11 of 14 female patients had an endotracheal tube ≤ 7.0 mm internal diameter. Although current data does not allow for a definitive conclusion regarding postoperative LI and endotracheal size, logical rationale would support the routine use of smaller endotracheal tubes for general anesthetics.
Outcomes
In this study, laryngeal injury after general anesthesia with tracheal intubation was found to be uncommon albeit clinically significant complication. Although 71% of patients reported some improvement in dysphonia, none achieved complete resolution, highlighting the potential for long standing morbidity. Of note, given that our institution receives referral patients from other regions of the country, several patients had relatively short postoperative follow-up, and thus long-term outcomes could not be assessed. Hyaluronic acid injection was the most common intervention, and while it provided temporary relief in some cases, repeat procedures were required, consistent with prior studies demonstrating limited durability of this therapy.29,30 Notably, a subset of patients improved spontaneously without intervention, aligning with previous report of gradual recovery over time. 31 These findings underscore the importance of early recognition of LI and timely referral for laryngology evaluation. Prompt diagnosis and tailored management strategies may help optimize functional outcome. 32
Limitations
This study is subject to the inherent limitations of its retrospective design. The reported incidence likely underestimates the true occurrence of postoperative LI. For example, patients with mild dysphonia may have experienced spontaneous recovery, chosen not to seek evaluation, or obtained care outside our institution, resulting in a cohort that primarily reflects more severe cases referred to the otolaryngology clinic for assessment. Furthermore, loss to follow-up in 9 patients, together with incomplete recovery observed in 6 patients during early postoperative evaluations, precludes definitive conclusions regarding long-term recovery following postoperative LI. Finally, this study could not elucidate the mechanism of LI; however, we did not include cases from surgical procedures associated with high risk for surgical injury to laryngeal nerves. Also, there is a possibility that some patients had predisposition for LI and that intubation and presence of endotracheal tube contributed to injury, as in few patients the exam revealed presence of ‘polypoid structures’, and in 1 ‘fungal laryngitis’. Therefore, we cannot make a definitive attribution regarding causation of injury. While the laryngeal symptoms manifested after tracheal intubation, this does not definitively prove that the tracheal intubation was causative. Furthermore, the relatively small sample size and loss to follow-up represent additional methodological constraints that may limit the generalizability and strength of the conclusions drawn.
Conclusion
In conclusion, laryngeal injury following tracheal intubation can occur even after seemingly atraumatic instrumentation. Its clinical presentation varies widely, ranging from vocal cord immobility to isolated hoarseness without detectable structural laryngeal damage. The exact pathogenesis remains unclear, as it is often difficult to distinguish whether the injury arises from laryngoscopy during intubation or preexisting laryngeal pathology. Postoperative dysphonia persisting over several days should prompt referral to otorhinolaryngology for early evaluation and management, potentially improving outcomes with treatments and therefore reducing long-term voice impairment.
Supplemental Material
sj-docx-1-aor-10.1177_00034894261457485 – Supplemental material for Laryngeal Injuries Following General Endotracheal Anesthesia: A Case Series
Supplemental material, sj-docx-1-aor-10.1177_00034894261457485 for Laryngeal Injuries Following General Endotracheal Anesthesia: A Case Series by Aurelia Zodl, Toby N. Weingarten, Martin J. Ryll, Semirra L. Bayan, Dale C. Ekbom, Juraj Sprung and Tracy E. Harrison in Annals of Otology, Rhinology & Laryngology
Footnotes
Acknowledgements
We would like to acknowledge Anesthesia Clinical Research Unit (ACRU) Data Specialists, Ms. Kellie A Robbins, M.S.N., R.N., for her help with data extraction.
Ethical Considerations
The Mayo Clinic Institutional Review Board approved this study (IRB number 25-002285, May 1, 2025). In accordance with Minnesota State Statute 25-002285, we included only patients who provided written authorization for research use of their medical records.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Department of Anesthesiology and Perioperative Medicine, Mayo Clinic. No external funding was provided.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.N.W. has received consulting fees from Merck & Co, Takeda Pharmaceuticals International Co, and Trevena, Inc.
Data Availability Statement
Authors elect to not share data due to patient privacy concerns.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.