
Abstract
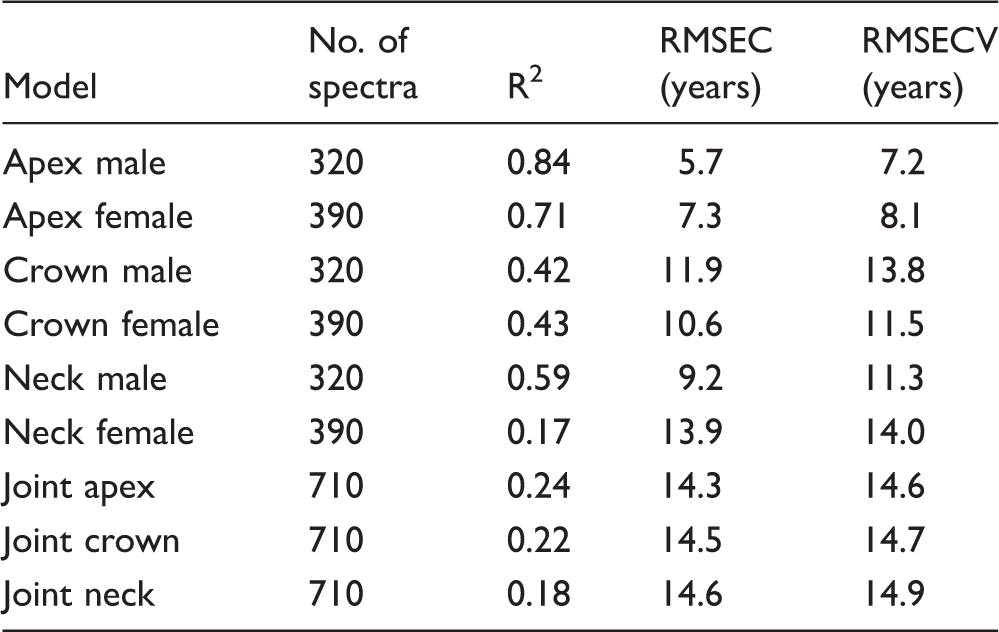
Raman spectra of mineralized tooth tissues were used to build a principal component regression (PCR) age determination model for forensic application. A sample of 71 teeth was obtained from donors aging from 11 to 76 years. No particular selection criteria were applied; teeth affected with various pathological processes were deliberately included to simulate a realistic forensic scenario. In order to comply with the nondestructive specimen handling, Raman spectra were collected from tooth surfaces without any previous preparation. Different tooth tissues were evaluated by collecting the spectra from three distinct sites: tooth crown, tooth neck, and root apex. Whole recorded spectra (3500–200 cm−1) were used for principal component analysis and building of the age determination model using PCR. The predictive capabilities of the obtained age determination models varied according to the spectra collection site. Optimal age determination was attained by using Raman spectra collected from cementum at root apex (R2 values of 0.84 and 0.71 for male and female donors, respectively). For optimal performance of that model, male and female donors had to be analyzed separately, as merging both genders into a single model considerably diminished its predictive capability (R2 = 0.29).
Keywords
Introduction
Age determination is one of the most common forensic procedures which has a wide range of applications, including identifications of accident victims, crime investigations, and social benefit regulations. Among various types of tissues available for forensic analyses, mineralized dental tissues are advantageous due to their high resistance to postmortem decomposition. 1 In forensic dentistry, three distinct approaches can be used for age determination: (i) the assessment of tooth morphological features by visual inspection or radiography, (ii) the evaluation of tooth histological characteristics using microscopy, and (iii) the evaluation of biochemical composition of tooth tissues using various analytical methods, including Raman spectrometry. 2 Whereas morphological and histological methods are routinely practiced in the contemporary forensic dentistry, 1 the biochemical analyses are still more pertinent to the experimental domain. 3 However, the biochemical means of age estimation offer important advantages over the conventional approaches, rendering them useful complementary methods. 4 For example, biochemical analyses require very small amounts of mineralized tissues and are applicable in cases of extensively damaged teeth. 5
Raman spectrometric analyses of dental hard tissues have been performed in various studies, including evaluations of enamel mineralization,6–8 early caries detection,9–11 compositional differences between primary and permanent teeth, 12 and mapping of the spatial distribution of organic and inorganic components in dental tissues. 13 However, only two studies have employed Raman spectrometry to relate the aging-dependent compositional changes in tooth tissues with the donor’s age for forensic purposes.14,15 In these studies, Raman spectra were collected from surfaces of longitudinally sectioned sound teeth and partial least squares regression was performed to correlate predefined compositional variables obtained from Raman spectra with tooth donor’s age. The aforementioned studies were based on ideal case scenarios in which Raman spectra were collected from standardized, flat-cut specimen surfaces obtained from healthy teeth. In order to complement these proof-of-principle studies, the present investigation simulated a more realistic scenario by including the teeth that were affected by common pathological processes, such as periodontal disease and dental caries. In addition, the spectral analysis in the present study was performed considering the whole Raman spectra, in contrast to the aforementioned studies which analyzed various combinations of parameters characterizing individual vibrational bands.14,15 Instead of cutting the teeth to analyze their internal structure, Raman spectrometry in the present study was performed on more accessible external surfaces of teeth. The described approach was adopted in order to evaluate the feasibility of Raman spectrometric age determination by using nondestructive handling of teeth that were affected by various pathologies. The research hypotheses were: (i) Raman spectra obtained from teeth would correlate with donor’s age and (ii) different sites of spectra collection (tooth crown, tooth neck, and root apex) would influence the accuracy of age estimation models.
Materials and Methods
The teeth were extracted at the university clinic of the School of dental medicine, Zagreb, Croatia. As an integral part of the regular practice of informed consent at the clinic, all donors agreed that their teeth can be retained and used for research. No personal data and other identifying information about donors have been disclosed to the investigators. The collection and handling of biological material were conducted in full accordance with the World Medical Association Declaration of Helsinki regarding ethical principles for medical research involving human subjects. The soft tissues that remained after tooth extraction were removed using a plastic brush and the teeth were disinfected by soaking in a 1% formaldehyde solution for 24 h. Thereafter, the teeth were stored dry in dark containers at room temperature (23 ± 3℃) in the archive of the Department of Dental Anthropology of the School of Dental Medicine, University of Zagreb, Croatia.
The sample of 71 teeth used for this study was obtained by a random draw from the aforementioned archive. The age of tooth donors ranged between 11 and 76 years (Table I). The teeth had been extracted due to various indications, most common being periodontitis (51%) and failed endodontic treatment (39%). To simulate a forensic analysis of teeth at different postextraction time periods, the time span between extraction and performing Raman spectrometric measurements ranged between 0.1 and 5.5 years. No special selection criteria were applied; teeth affected with various pathological processes were deliberately included to simulate a realistic sample. The visual appearance of teeth affected by the most common pathologies is represented in Fig. 1.
Representative specimens of teeth affected to different extents by various pathological processes: (a) sub-gingival calculus reaching up to the mid-root level which is indicative of advanced periodontitis, (b) severe destruction of the tooth crown accompanied by irreversible pulpal inflammation, (c) extensively restored tooth with the discolored root indicating failed endodontic treatment, (d) caries at the level of the tooth neck, and (e) sound third molar extracted due to impaction. Characteristics of teeth used in this study. Ortho: orthodontic extraction; Endo: failed endodontic treatment or inability to perform endodontic treatment; Perio: extraction due to advanced periodontitis; Imp/ret: impacted or retained tooth.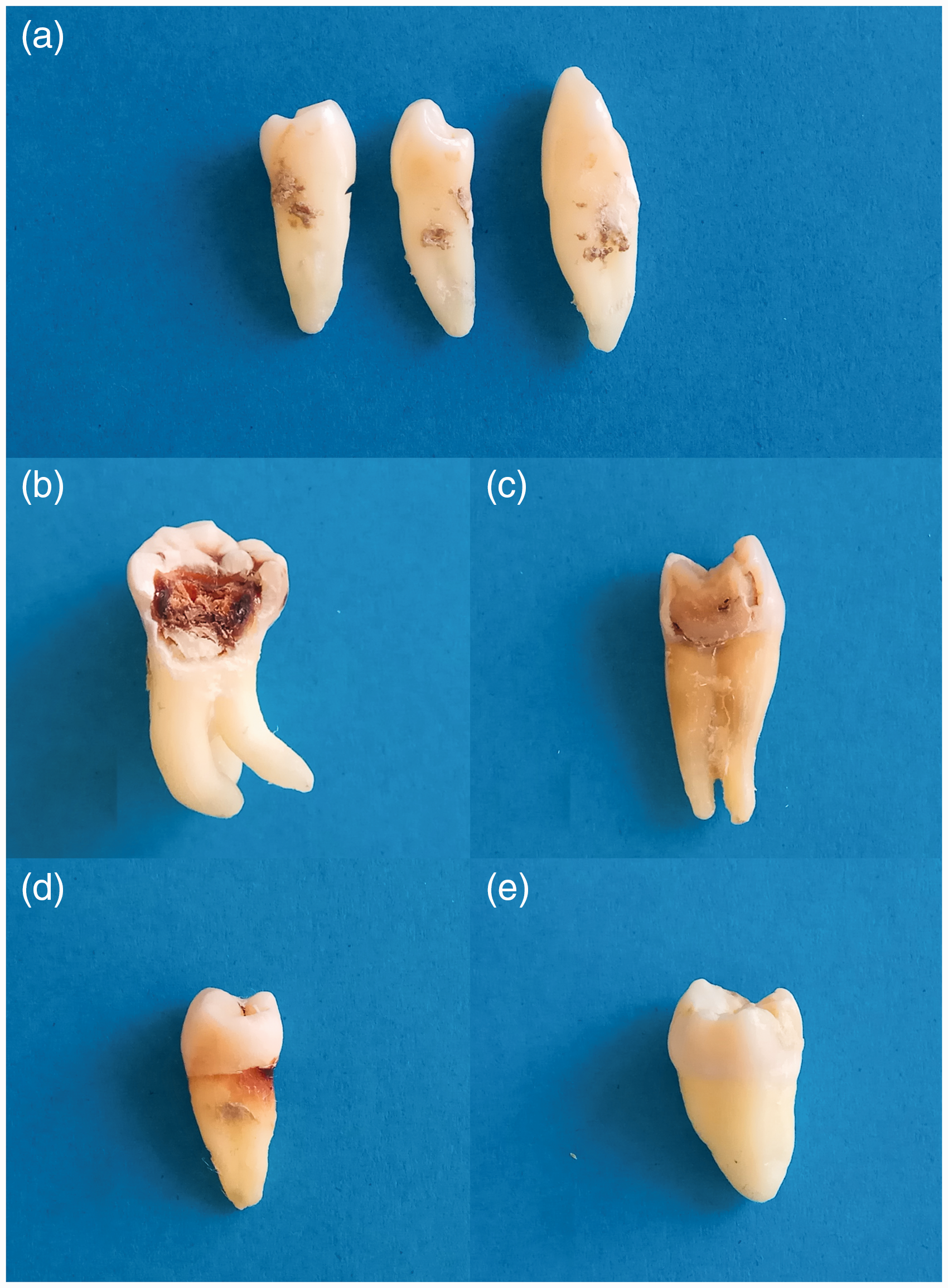

Raman spectra were recorded using an FT-Raman accessory of the Spectrum GX spectrometer (Perkin Elmer, USA) equipped with a neodymium-doped yttrium aluminum garnet (Nd : YAG) laser of 1064 nm wavelength. Each spectrum was recorded by averaging 100 scans in the spectral range between 3500 and 200 cm−1 and with a spectral resolution of 4 cm−1. Spectra were collected from three distinct sites on each tooth: crown, neck, and apex (Fig. 2). At each site, an area of 2.5 mm in diameter was chosen, over which the excitation laser spot (0.25 mm in diameter) was moved in a scanning motion to collect Raman spectra from 10 different positions. This was done in order to account for local heterogeneities of mineralized tooth tissues. Therefore, a total of 30 spectra per tooth were collected (three sites, 10 spectra). The spectra were stored in a data set and connected with the donor’s age and collection site.
(a) Schematic representation of three sites on the external tooth surface from which Raman spectra were collected; (b) a tooth attached to the specimen holder with an aperture of d = 2.5 mm which was used for defining the sampling surface.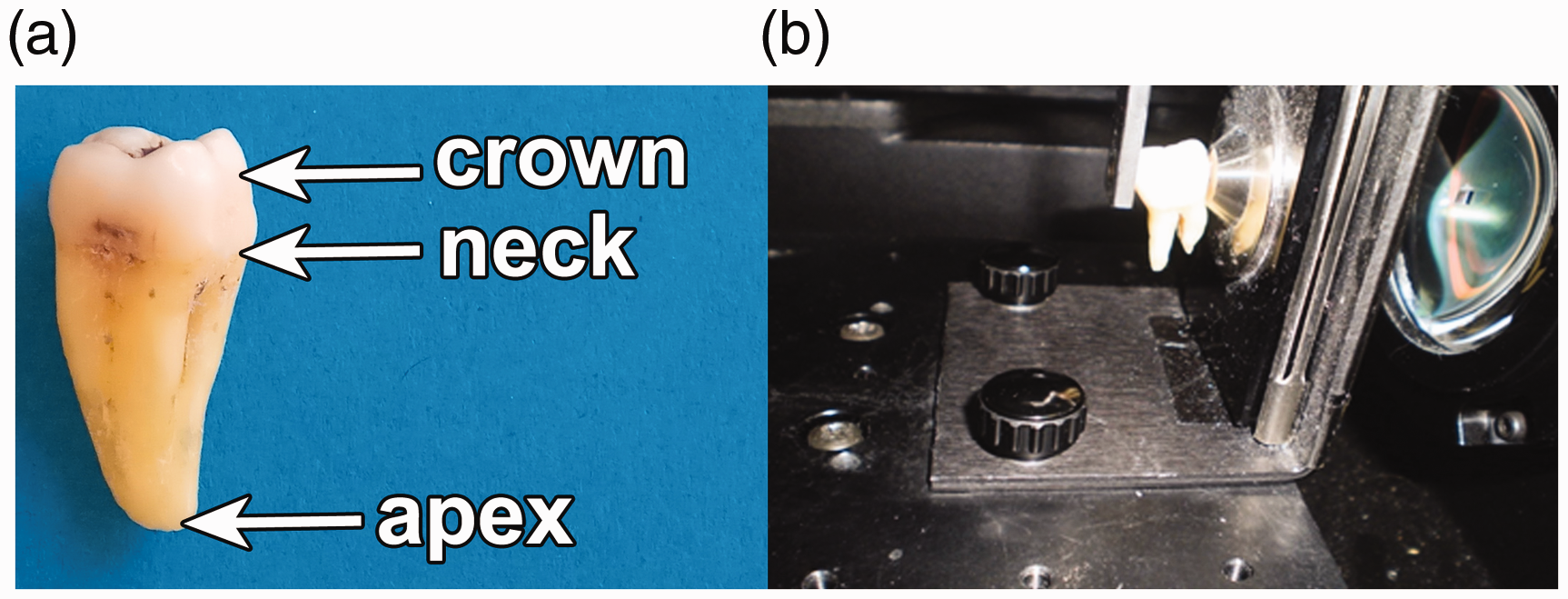
Designation of age groups for principal component analysis.
Results
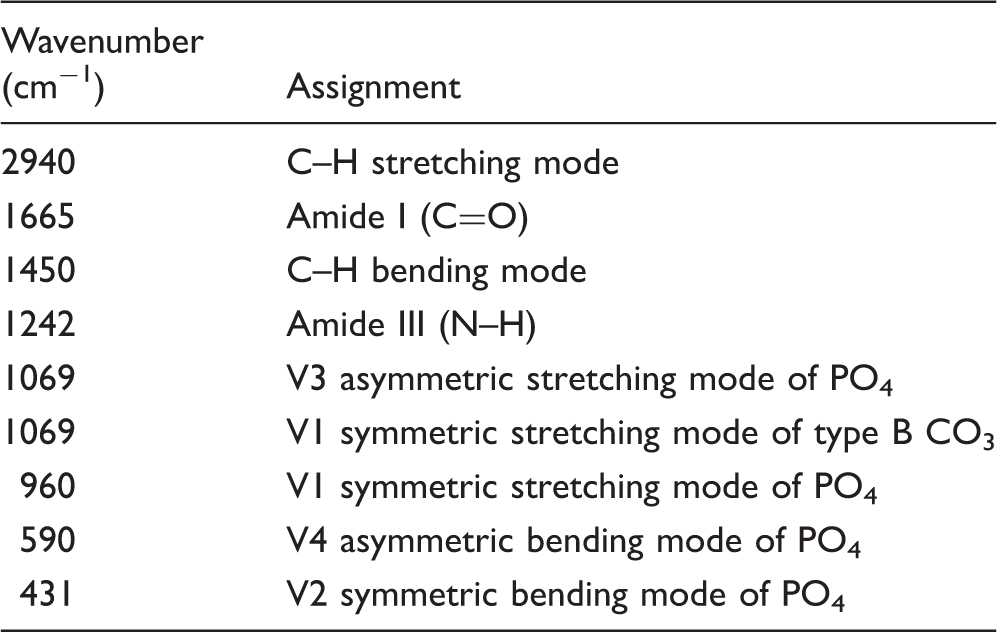
Representative Raman spectra collected from different tooth sites are shown in Fig. 3. The inorganic part is represented by vibrational bands in the wavenumber range of 1100–400 cm−1 (PO4 and CO3 vibrations), while the organic part is represented in the range of 3100–1100 cm−1 (amide bands and C–H vibrations).13,20 While the spectra from all three sites featured the same bands, the inorganic/organic ratio was considerably higher in spectra collected from the crown compared to the other two sites. This reflects the fact that all types of tooth tissue comprise the same basic building blocks, although in various relative amounts. Individual assignments of spectral bands are shown in Table III. From a biochemical perspective, the major component of the inorganic part is carbonated calcium-deficient hydroxyapatite, while most of the organic part consists of collagen.21,22
Representative Raman spectra collected from apex, crown, and neck. The spectra are normalized on the PO4 band at 960 cm−1. Assignments of Raman vibrational bands.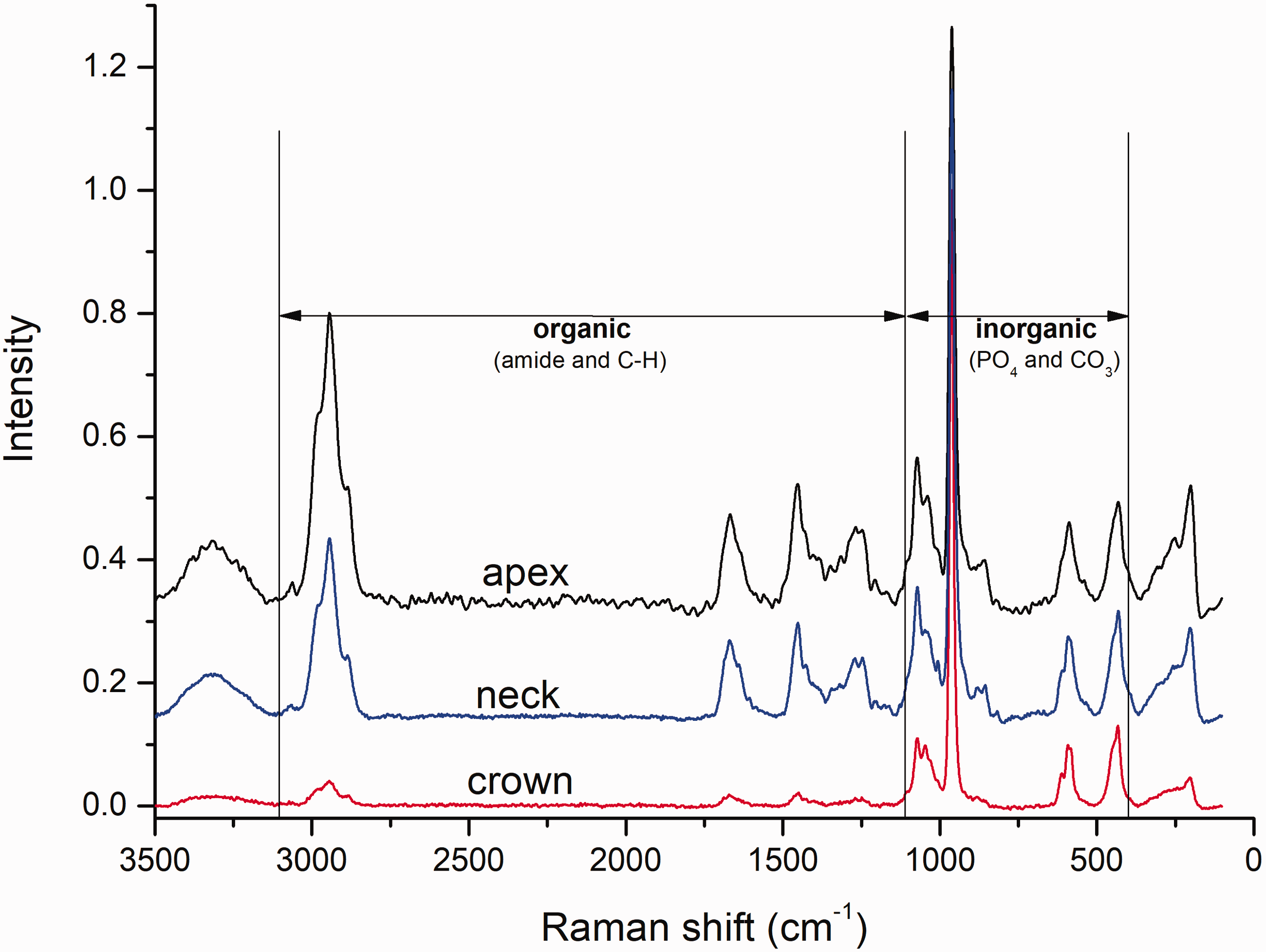
To illustrate aging-related spectral changes, baseline-corrected and normalized spectra collected from the apex of male donors are presented as average spectra for each of the seven age groups (Fig. 4). The changes in the intensity of bands representing both the inorganic and organic components of tooth tissues indicate that it is possible to build a PCA model for distinguishing donor’s age using Raman spectra. Also, the spectral changes occurring as a function of donor’s age indicates that a PCR model for age determination can be built.
Average Raman spectra for seven age groups. The spectra were collected from the root apex of male donors. Note the breaks on the x- and y-axes.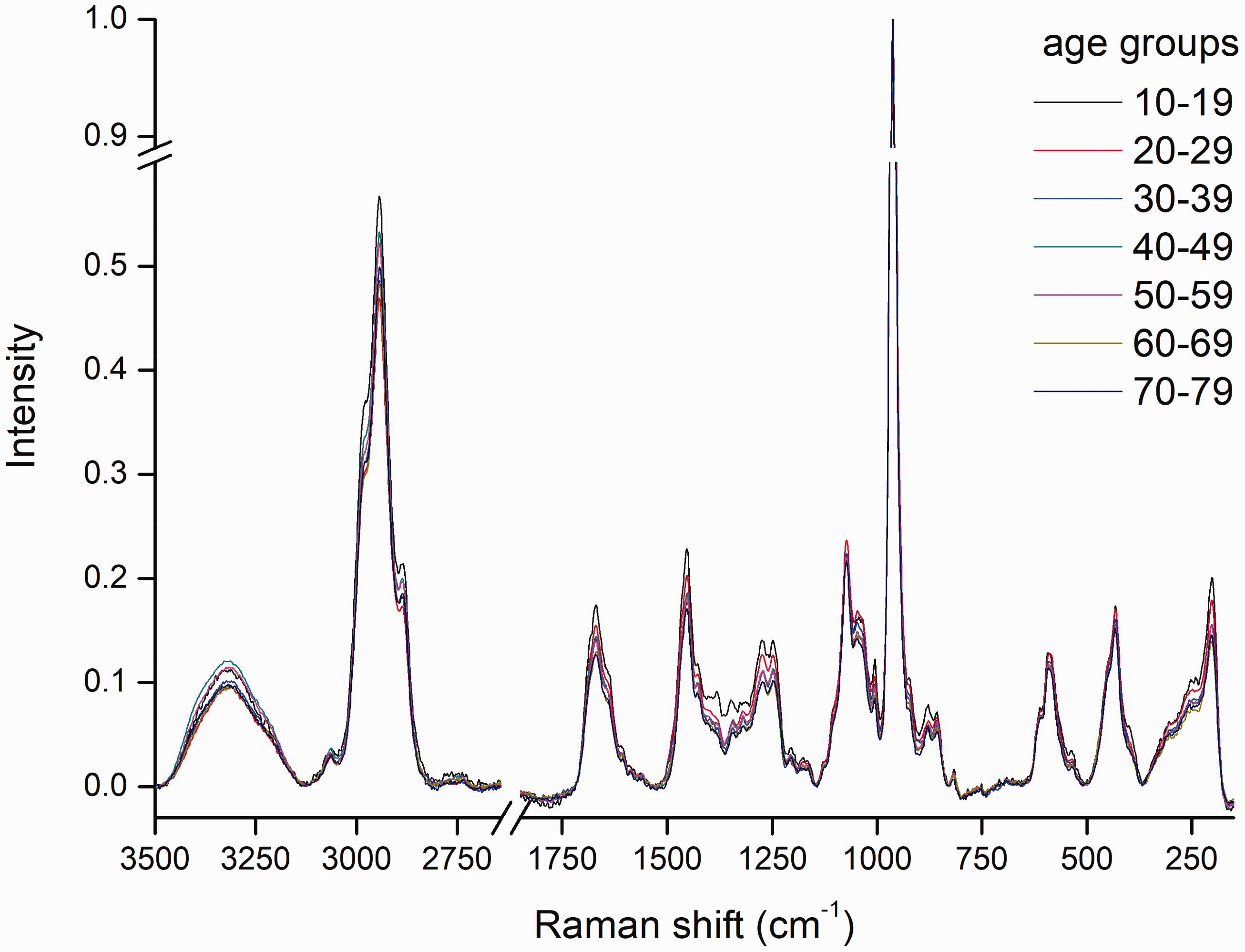
Characteristics and predictive capabilities of different PCR models: number of spectra on which the models were based, coefficient of determination (R2), root mean square error of calibration (RMSEC), and root mean square error of cross-validation (RMSECV).
PCA loadings plots for PC1 and PC2 are plotted with the corresponding representative spectra for each spectra collection site in Fig. 5. In models built from the apex spectra, only PC1 loadings were different from zero (Fig. 5a), while for crown and neck, both PC1 and PC2 loadings differed from zero (Figs. 5b and 5c). For all spectra collection sites, the contributions to first two principal components originated from both the organic and inorganic part of Raman spectra.
PCA loadings plots for the principal components used for age determination models, based on spectra collected from (a) apex, (b) crown, and (c) neck.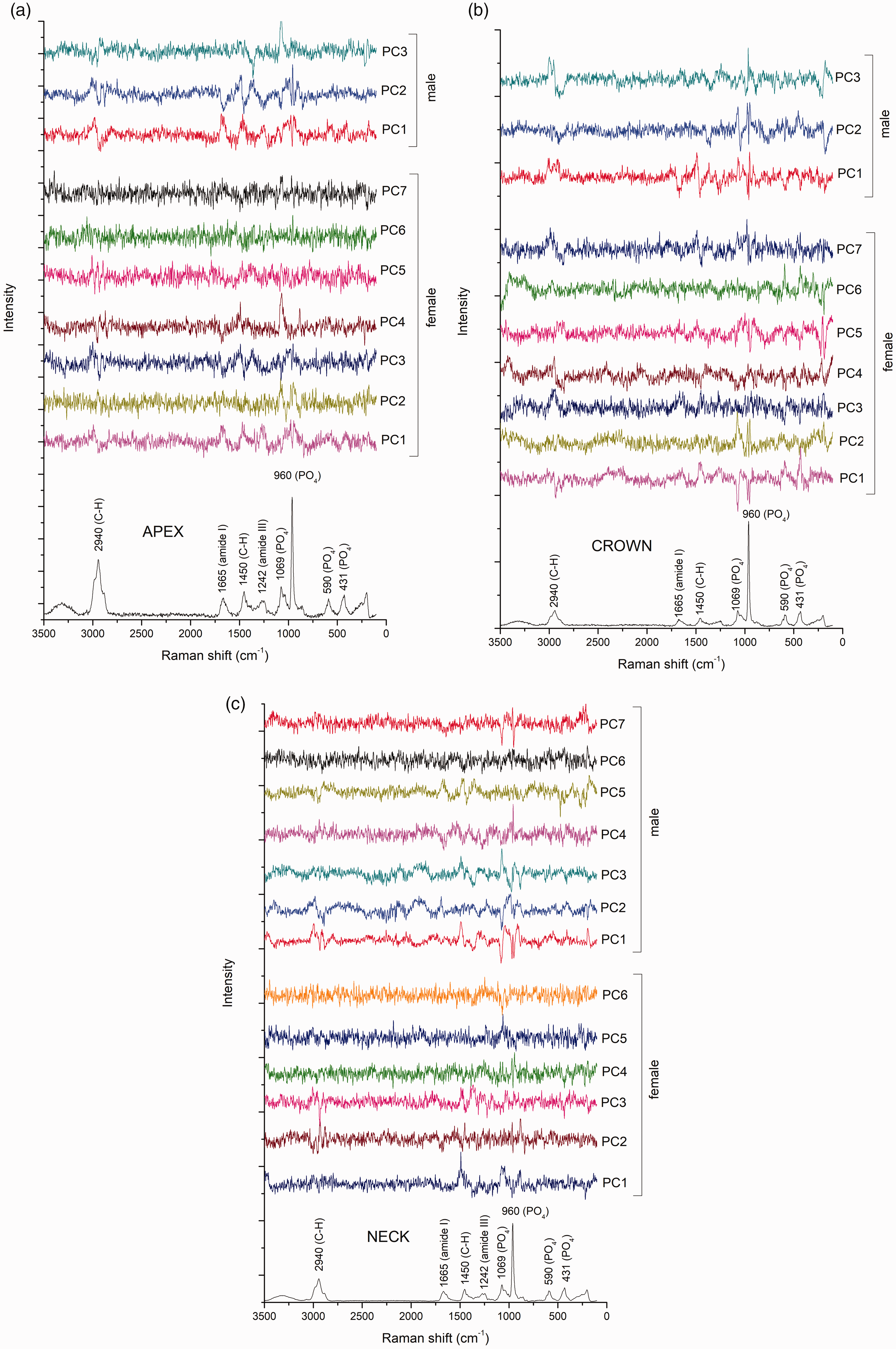
The regression plots for tooth donor’s age and scatterplots for the first two principal components are shown in Fig. 6, for each combination of gender and spectra collection site. The red lines in regression plots represent the actual correlation between measured and predicted values, while the green lines represent an ideal correlation. The PCA models based on apex spectra showed a comparatively better separation of age groups than the models based on neck and crown spectra. Accordingly, the PCR age determination models based on apex spectra showed higher coefficients of determination and lower error values compared to the models based on neck and crown spectra. The PCA scatterplots for apex indicate that age groups were separated only along the PC1 axis (Figs. 6a and 6b). In the PCA model for male apex (Fig. 6a), younger age groups (10–39 years) were especially well separated from older age groups (40–79 years). Comparatively more overlapping between the age groups was found in the PCA model for female apex (Fig. 6b). In contrast to the PCA models for the apex, spectra from neck and crown were distinguishable by both PC1 and PC2 (Fig. 6c to 6f).
Regression plots and scatterplots for the first two principal components. The results are presented for models based on the following combinations of spectra collection site and gender: (a) apex male, (b) apex female, (c) crown male, (d) crown female, (e) neck male, and (f) neck female.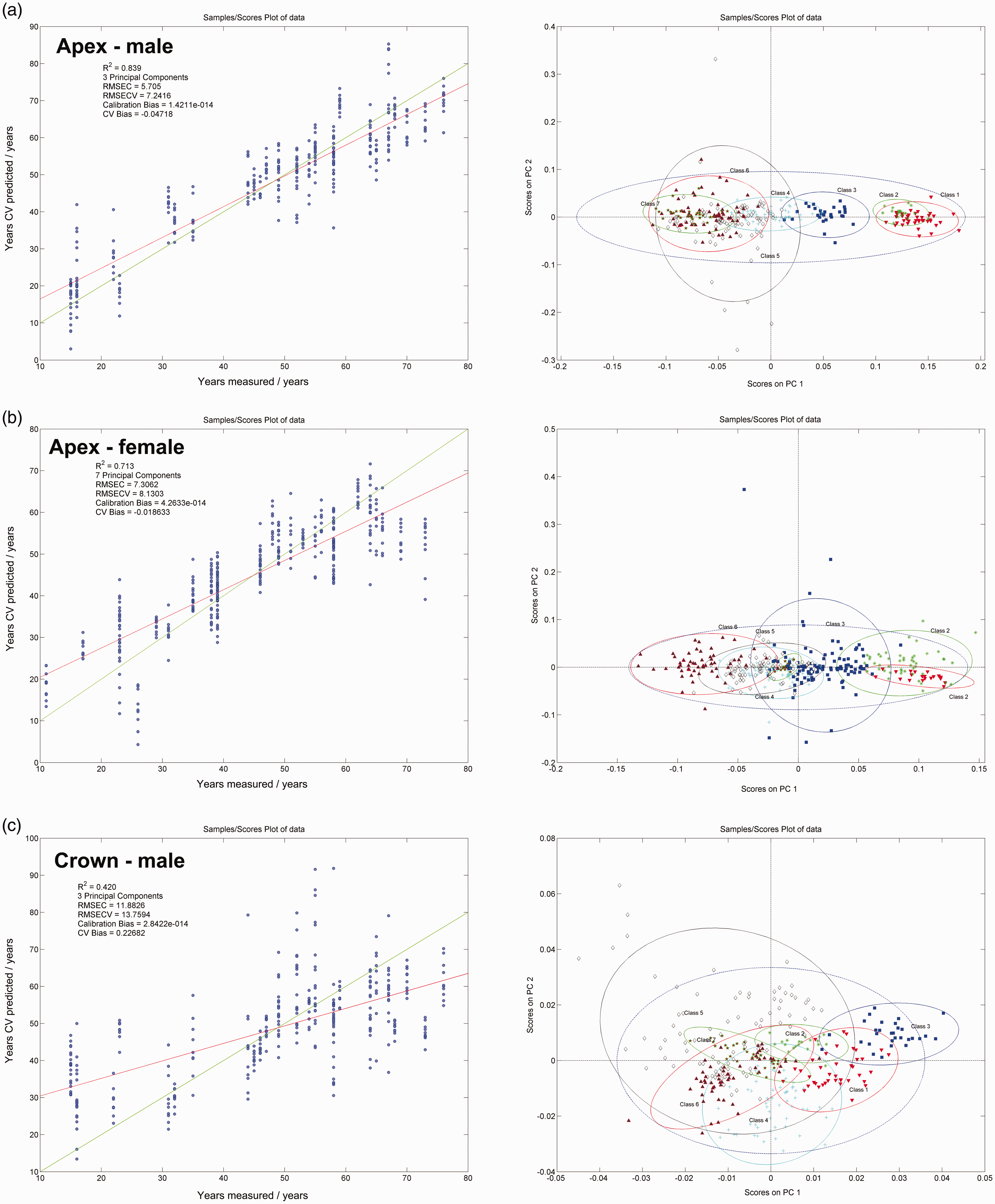
Discussion
In this study, Raman spectra of mineralized tooth tissues were used to build a PCR age determination model for forensic applications. The predictive capabilities of the obtained models varied according to the spectra collection site. Therefore, both research hypotheses were accepted.
The accuracy of regression models for age determination depends on the ratio of the variance attributable to aging-related changes and the uncontrolled variance due to various external factors and interindividual genetic differences. Relative magnitudes of these two sources of variance differed across the investigated sites at the tooth surface, thereby affecting the suitability of a particular site for age determination. High R2 values identified for apex indicate that a proper selection of spectra collection site can minimize uncontrolled variance. Comparatively poorer coefficients of determination were obtained for spectra collected at tooth neck and crown, indicating a higher magnitude of uncontrolled variance at these sites. The differences in the suitability of different tooth sites for age determination can be explained by the distribution of different types of mineralized tissues across these sites. Three main mineralized tooth tissues include enamel, dentin, and cementum. These tissues differ by their fundamental physiological processes and the capability to respond to external stimuli, which affects their aging-related compositional changes. 23
Enamel is the most highly mineralized tissue in the human body, with an inorganic content of 96 wt%. Enamel covers the tooth crown and is distinct from other mineralized tooth tissues because its formative cells are destroyed upon tooth eruption into the oral cavity. 24 As no cellular reparatory response is possible, the aging-related changes of enamel are completely under the influence of environmental factors and masticatory function. With aging, the enamel layer progressively becomes thinner due to chemo-mechanical degradation caused by erosive foods and chewing forces. 25 Additionally, the biofilm on the tooth surface harbors acidogenic bacteria which cause demineralization, i.e., loss of calcium and phosphate ions. The process of demineralization is counteracted by the remineralizing action of calcium and phosphate ions from the saliva. 26 These processes interchange cyclically, making the loss of ions fully reversible. However, if the net balance between remineralization and demineralization is negative for a prolonged period of time, enamel progressively losses its integrity and a carious lesion occurs. Between the sound and the carious state as the extremes, a whole range of intermediate demineralization stages is possible. The surface enamel layer in vivo usually presents various levels of mineralization which are heterogeneously distributed across the tooth surface. 6 This compositional heterogeneity is reflected in the Raman spectra of enamel9,11 and introduces the uncontrolled variance that impairs the accuracy of the PCR model for age determination. Therefore, the low coefficients of determination obtained for the spectra collected from the crown can be attributed to the fact that enamel composition and structure were highly influenced by individual differences related to lifestyle, diet, and oral hygiene practice. 27
Cementum is a mineralized tissue that covers the tooth root and increases in thickness towards the root apex. With approximately 65 wt% of inorganic and 25 wt% of organic content, cementum resembles the chemical composition of bone. 28 However, cementum is structurally different from bone as it is avascular and does not undergo continuous remodeling. Instead of remodeling, cementum is incrementally deposited by its formative cells (cementoblasts) throughout the lifetime. 29 Under physiological conditions, the recruitment of cementoblasts from progenitor cells and the deposition of cementum occurs at a steady pace. 30 The resulting compositional changes identified by Raman spectrometry appear to be consistent with aging, as indicated by high R2 values obtained for spectra collected from the apex. As a potential source of uncontrolled variance at that site, periodontal inflammatory processes should be considered. The periodontal inflammation (periodontitis) with the prevalence of up to 50% in the general population is one of the most common diseases in developed countries. 31 Periodontitis was also the most common reason for the extraction of teeth used in this study; 36 out of 71 teeth (51%) were extracted due to advanced periodontitis. The pathophysiology of periodontitis involves inflammation-mediated destruction of tooth-supporting tissues triggered by specific bacterial species. As the disease is often left untreated, chronic low-level inflammation can persist for years and affect the structure and composition of cementum. On the other hand, the periodontal treatment that involves mechanical scraping of the infected root surface also inflicts damage to cementum and affects the metabolic processes in cementoblasts. Consequently, either treated or untreated periodontal disease can affect the composition of cementum. 32 As periodontitis is initiated at the level of the tooth neck and gradually advances in the apical direction over the course of the disease, the mineralized tissues at the tooth neck are more frequently and severely affected by the joint effect of periodontitis and periodontal treatment. Except in the most severe cases of periodontitis, the apical cementum remains unaffected. The fact that apical cementum is mostly protected from external influences and is characterized by a steady rate of compositional changes renders root apex an appropriate spectra collection site for the age determination PCR model. Another factor that may affect the structure of apical cementum is periodontal inflammation of endodontic origin, which is initiated and most pronounced around root apex. 33 Considering that 39% of the teeth used in this study were extracted due to failed endodontic treatment, this type of pathology was rather common in the analyzed sample. However, it appears not to have significantly impaired the suitability of apical cementum as the tissue of choice for age determination.
Dentin is a mineralized tooth tissue with approximately 65 wt% of inorganic and 20 wt% of organic content. Dentin constitutes the bulk of the tooth and is covered by an enamel layer on the crown and a cementum layer on the root. The structure and composition of dentin are determined by the metabolic activity of its formative cells (odontoblasts) throughout the lifetime. 34 Despite having an acellular structure, dentin is permeated by tubules that contain cytoplasmatic processes of odontoblasts located within the dental pulp. Over the lifetime, these cells continuously secrete minerals into the walls of dentinal tubules, leading to their narrowing, reduced permeability, and increased mineral content. 35 Under physiological conditions, dentin is fully covered by other mineralized tissues and protected from external influences. Therefore, compositional changes of dentin correlate well with donor’s age, which has been exploited in two aforementioned studies employing Raman spectrometry for age determination.14,15 In these studies, access to intact dentin was accomplished by tooth sectioning. Such access to dentin within the bulk of the tooth was not possible in the present study due to the nondestructive specimen preparation. However, areas of dentin were exposed on the tooth neck surface due to defects in overlying enamel and cementum. Dentin exposure on the tooth neck commonly occurs due to repeated damage of overlying enamel and cementum caused by masticatory loading, acid exposure, and aggressive tooth brushing. 36 Within the surface area exposed to the excitation laser (circular spot of d = 0.25 mm), small areas of exposed dentin were sampled together with various fractions of enamel and cementum. Therefore, Raman spectra collected from the tooth neck contained contributions from all three types of mineralized tissues. The relative magnitudes of these contributions varied according to the extent of damage to overlying enamel and cementum, which was not quantified in the present study. The compositional heterogeneity of the mixture of mineralized tissues sampled at the tooth neck can explain the low predictive value of the PCR model based on spectra collected at that site. Also, the exposed dentin on the tooth neck exhibited faster mineral deposition and tubular occlusion as a part of the protective physiological response, 37 which introduced additional variance that was unrelated to aging.
Regarding apical cementum, which was identified as the most suitable tissue for age determination, it is interesting to note that PCR models based on apex spectra were more accurate for male than female donors. This might be related to the potential of female sex hormones to affect cementoblast metabolism, thereby introducing interindividual differences into the structure and composition of cementum. Although the effect of female sex hormones on cementoblast functions has not been well investigated, cementoblasts are known to respond to estrogens. 38 Therefore, fluctuations in the levels of female sex hormones might be involved in the regulation of cementoblast function similarly to that in bone metabolism. 39 The individual variations in the production of female sex hormones and the corresponding cementoblast response can be speculated to have caused a lower accuracy of the age determination model for females.
The aging-related compositional changes in mineralized tissues that made the age determination model possible were identified in both the inorganic and the organic part of Raman spectra. These changes can be attributed to different processes occurring in tooth tissues with aging, including qualitative changes of calcium hydroxyapatite 40 and collagen, 41 as well as quantitative changes in the relative amounts of inorganic and organic components. 42 However, more detailed investigations of these processes through the analysis of principal component loadings were out of the scope of this study, which was focused on the practical application of Raman spectra for forensic age determination.
In teeth affected by various pathological processes, care was taken to collect Raman spectra from apparently intact tooth surfaces. While this approach helped to avoid areas severely affected by caries or covered by calculus, minor irregularities on the surface of mineralized tissues selected for the analysis might have remained unnoticed by visual inspection. A more precise microscopic inspection would allow better control over the quality of the sampled part of mineralized tissues; however, the naked-eye inspection was deliberately adopted as a part of the simplified and nondestructive specimen preparation. An additional rationale for not applying a strict selection of sound mineralized tissues was the study design simulating a realistic forensic scenario in which only a limited amount of material is available for analysis.
A major limitation of the present study is that the age determination model was based on teeth obtained exclusively from Caucasians, thereby not accounting for interethnic variations. It is reasonable to expect that age determination models would become less accurate if these were generalized to account for multiple races. 43 An additional shortcoming of the presented age determination model is that its predictive capability drops considerably if the gender of the donor is unknown. Therefore, for optimal accuracy of the age determination model described in this study, the gender and race of the tooth donor should be determined using other forensic methods. 44
This study showed that whole Raman spectra obtained from the tooth surface using macro-Raman measurements can be used for age estimation. The quality of age-related information varied among tooth sites, and apical cementum showed the highest predictive potential. Although the obtained R2 values were relatively modest even for apical cementum, it was possible to improve these values for more than 0.05 by removing 10% of outliers from the modeling set. This observation indicates that the precise definition of spectra recording conditions coupled with precise criteria for removing outliers can improve model precision. Such a refinement of age determination models will be addressed in our future studies.
Because Raman spectra of hydroxyapatite may be affected by laser light polarization,45,46 it should be mentioned that for spectra collection in our study, both incident and scattered light were unpolarized. Therefore, possible influences of polarization were consistent within all spectra, thereby introducing the same type of error to all of them. Because the algorithms applied in this study are based on detecting relative differences between spectra, that error can be neglected.
In comparison to the previously published approaches based on the extraction of preselected parameters of individual Raman bands,14,15 working with the whole Raman spectra for model building and later forensic application considerably simplifies the procedure. Additionally, macro-Raman measurements simulate spectra collection using a handheld Raman spectrometer, bringing the method closer to an actual forensic application. The age determination models built using spectra of unsound teeth have higher practical relevance than those based exclusively on intact teeth. Also, the spectra collection on the tooth surface is beneficial for forensic analysis, which generally favors nondestructive specimen handling.
To simulate a forensic scenario in which teeth at different postextraction time periods need to be analyzed, Raman spectra were collected 0.1–5.5 years after extraction. During the time period between extraction and spectra collection, the teeth were stored dry at room temperature. Mineralized tooth tissues remained well preserved under such conditions, whereas more extensive decomposition can be expected at higher temperatures or in highly acidic environments.47,48 At this point, it is not possible to determine whether the age determination model presented in this study would be applicable to teeth that were aged under extreme conditions. However, mineralized tooth tissues are known to be resistant to a range of environmental effects of moderate intensity, 1 indicating a potential of hereby presented age determination method for use in contemporary forensic dentistry.
Conclusion
This study showed that the age determination model based on principal component regression can be built using Raman spectra collected from surfaces of unsound teeth without any previous preparation. The optimal age determination capability was attained by using Raman spectra collected from cementum at root apex, whereas spectra collected from mineralized tissues at the tooth neck and crown were less suitable. The age determination model based on apex spectra showed an optimal performance only when tooth donor genders were analyzed separately.
Footnotes
Authors’ note
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.