
Abstract
Objective
We aim to establish the sex-related reference intervals (RIs) of PIVKA-II in southwest China by indirect method with the real-world data.
Methods
Between 29 July 2016 and 5 February 2024, PIVKA-II test data were collected from 120,780 healthy adult participants (aged 18 to 97 years) in the Laboratory Information System (LIS) of West China Hospital to establish reference intervals. Additionally, a validation group comprised of 2068 healthy adults was evaluated using the same detection algorithm and platform. Following the CLSI EP28-A3 guideline, Box-Cox transformation was applied for normal transformation, and outliers were identified using the Tukey method. Furthermore, we employed the standard normal deviate test (z-test) recommended by Harris and Boyd to determine whether to stratify reference intervals by age and sex subclasses.
Results
We successfully established population-specific RI for PIVKA-II in southwest China using an indirect method. By utilizing a robust dataset and conducting rigorous statistical analyses, we delineated sex-specific RIs, with values of 0–35 mAU/mL for males and 0–29 mAU/mL for females according to the normal distribution method, and 0–32 mAU/mL for males and 0–28 mAU/mL for females using the non-parametric method. These intervals are more suitable for the local population than those derived from manual methods.
Conclusion
These RIs provide valuable guidance for the accurate interpretation of PIVKA-II levels in the local population.
Introduction
Protein induced by vitamin K absence or antagonist-II (PIVKA-II), also known as des-γ-carboxyprothrombin or acarboxy prothrombin, is a distinct form of prothrombin primarily observed in individuals with vitamin K deficiency. 1 PIVKA-II has gained considerable attention for its clinical utility in screening for hepatocellular carcinoma (HCC), demonstrating excellent sensitivity and specificity compared to alpha-fetoprotein (AFP). 2 The integration of this marker into diagnostic protocols, often in conjunction with AFP, has facilitated the early detection of small-sized HCC in clinical practice.3–5 Additionally, incorporating PIVKA-II into current liver transplantation (LT) criteria could potentially increase the number of eligible HCC patients without compromising post-LT outcomes. 6 Furthermore, when used in combination with AFP, PIVKA-II enhances risk stratification in patients with HCV-related cirrhosis undergoing treatment with direct-acting antiviral agents (DAA). 7
To standardize and enhance the effectiveness of PIVKA-II, it is essential to establish reference ranges and specific cut-off values tailored to the local context. 3 Many laboratories depend on reference ranges provided in reagent manuals, which are typically derived from data collected from specific subsets of the population. However, it is crucial to recognize that these ranges may not accurately represent the full spectrum of global populations, given the variations in genetic makeup, dietary habits, lifestyle choices, and environmental factors. 8 In light of China’s ethnically diverse population, establishing local reference ranges for PIVKA-II based on the characteristics of the population is vital for informed clinical decision-making. 9 Although numerous scholars have recently published research on reference ranges for laboratory indicators using indirect methods,10–12 few studies have focused specifically on PIVKA-II, particularly in southwest China. The indirect method, based on observational confirmation, operates under the assumption that the majority of findings, even among hospital and clinic patients, conform to the 'normal' parameters as outlined in the CLSI EP28-A3C guideline. 13 This method employs mathematical-statistical algorithms to analyse data from hospital databases, including laboratory information systems (LIS), to define biological reference intervals (RIs). The indirect approach offers two primary advantages: (1) access to extensive and reliable data sources; and (2) a more straightforward, time-saving, and cost-effective process, facilitating the creation and periodic evaluation of reference ranges. 8 This study aims to establish sex-specific reference intervals for PIVKA-II in the southwest region of China by employing an indirect method that utilizes real-world data from 120,780 healthy adults recorded in the Laboratory Information System (LIS) of West China Hospital between 2016 and 2024. Through this approach, we seek to provide a robust foundation for accurate clinical diagnosis and treatment.
Materials and methods
Subjects
Between 29 July 2016 and 5 February 2024, PIVKA-II test results were collected from 120,780 healthy examination adults (ranged from 18 to 97 years old) in the Laboratory Information System (LIS) of West China Hospital. Duplicate entries were identified and excluded from the dataset based on physical examination number, name, and age, resulting in a total of 50,272 exclusions. For repeated individuals, we retained the test results when they first come. In the end, the research involved 70,508 individuals in good health (40,970 men and 29,538 women). The study grouped participants into different age categories based on the World Health Organization’s criteria for defining ageing. 14 These categories were 18–44 years, 45–59 years, 60–74 years, and over 75 years. There were 32,191 individuals in the 18–44 years category, 29,370 in the 45–59 years category, 7761 in the 60–74 years category, and 1186 in the category of individuals over 75 years old. In addition, to confirm the applicability of our findings to southwest China, we obtained PIVKA-II data from 2068 healthy adults who were assessed at West China Hospital using the identical detection algorithm and platform from February to 3 March 2024, for the purpose of validation (Supplemental Table 1). We examined the proportion of validation subjects that fell outside our established reference intervals. If the ratio is below 5%, we consider the reference interval to be valid. 13 Owing to the retrospective and anonymous nature of this study, informed consent was not required. This study protocol was approved by the Ethics Committee of West China Hospital of Sichuan University (No. 20241706), and was performed in accordance with the Declaration of Helsinki.
Measurement of serum PIVKA-II
Serum PIVKA-II levels were determined using the LUMIPULSE G1200 instrument (Fujirebio-Europe, Gent, Belgium) and the LUMIPULSE G PIVKA-II kit (Fujirebio, Tokyo, Japan), which uses chemiluminescent enzyme immunoassay (CLEIA) technology. All reagents used were within their expiration dates and safe to use, with quality control checks performed prior to sample analysis. We test the patient’s serum samples in strict accordance with the requirements of the instrument and reagent instructions.
Statistical analysis
Reference intervals were determined in accordance with the CLSI EP28-A3 guideline. 13 We assessed the normality of the PIVKA-II data by conducting the Skewness-Kurtosis test. Whenever a non-Gaussian distribution was observed, we applied the Box-Cox transformation and identified outliers using the Tukey method. 13 To determine whether to divide reference intervals by age and sex subclass, we implemented the z-test recommended by Harris and Boyd. 13 The independent t test and ANVOA analysis were conducted if it becomes necessary to group them by age or sex. We then utilized both the normal distribution method and the non-parametric method to calculate the 95% distribution RIs for PIVKA-II. Since only elevated PIVKA-II values are clinically relevant, RIs were presented as the 95th percentile for the non-parametric method and as mean + 1.645 SD for the normal distribution method. Excel 2016 (Microsoft, Redmond, WA) was used to conduct the Tukey method and z-test. SPSS version 26.0 for Windows (SPSS Inc., Chicago, IL, USA) was used to detect the normality of the data, perform the independent t test and ANVOA analysis and calculate the 95% distribution RIs for PIVKA-II. Stata 17.0 software (StataCorp, Texas, TX, USA) were used to carry out Box-Cox transformation (undetermined parameters λ are obtained by maximum likelihood method). Charts were created using GraphPad Prism 7. The significance level was set at 0.05.
Result
Normality testing and outlier detection
Normality Test of PIVKA-II Before and After the BOX-COX Transformation.

Data Before and After the Removal of Outliers Using the Tukey Method After the BOX-COX Transformation.

Effect of age and sex on serum PIVKA-II levels
Age and serum PIVKA-II exhibited no significant correlation, as determined by the standard normal deviate test (Supplemental Table 2 and Supplemental Figure 1). Consequently, RIs for all age groups were combined. Furthermore, the standard normal deviate test was utilized to assess the influence of sex on PIVKA-II levels, revealing a statistically significant difference between males and females (P < .0001, Figure 1). Box plots depicting serum PIVKA-II levels by sex (**** represents P < .0001).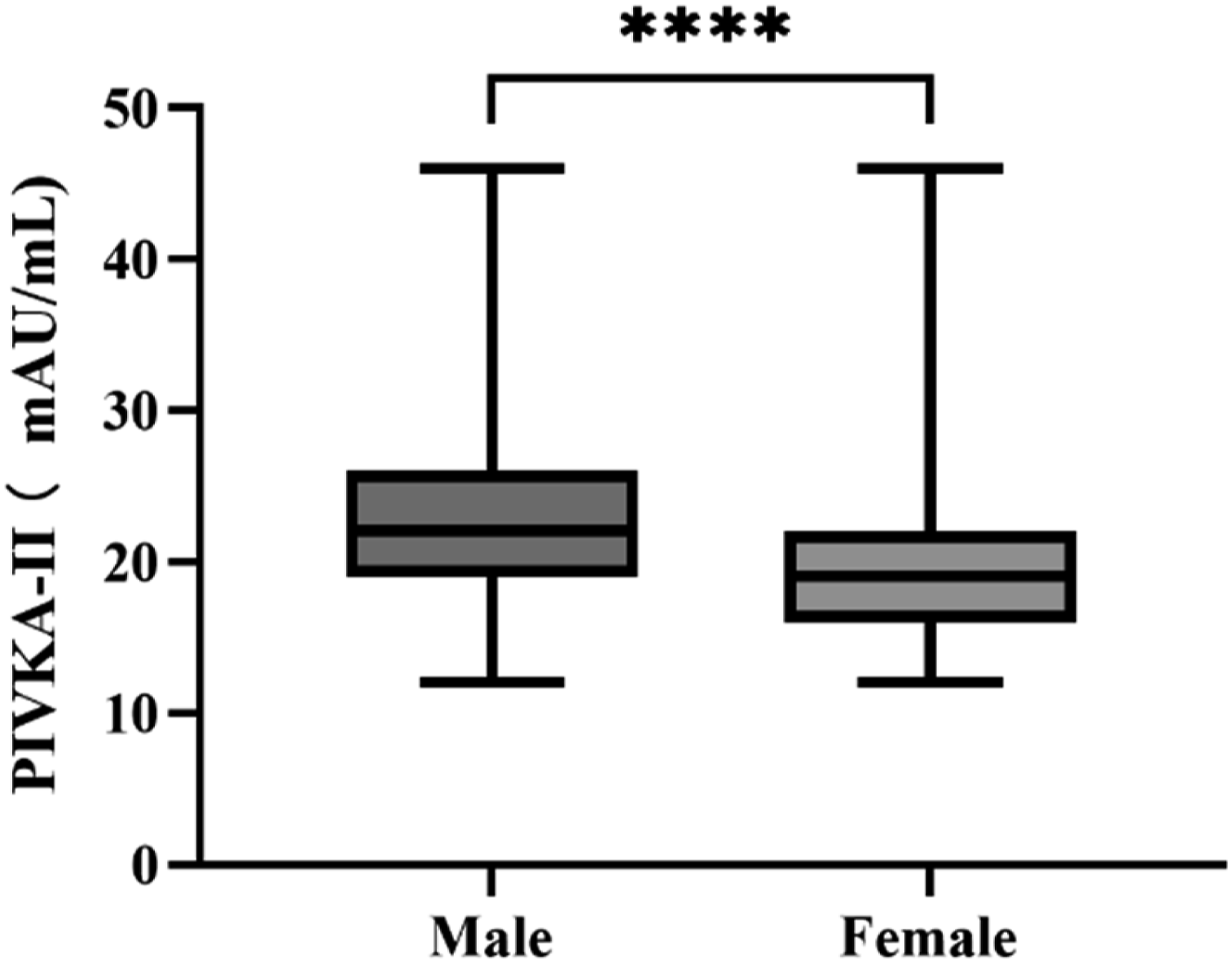
RIs of serum PIVKA-II levels in males and females
PIVKA-Ⅱ RI Calculated by Parametric and Non-parametric Methods.

RI1: normal distribution RI (mean + 1.645 SD) calculated by the BOX-COX transformation data; RI2: non-parametric RI (P95).
CI: confidence intervals.
Verification and comparison of reference intervals
The Verifying of PIVKA-II RIs.
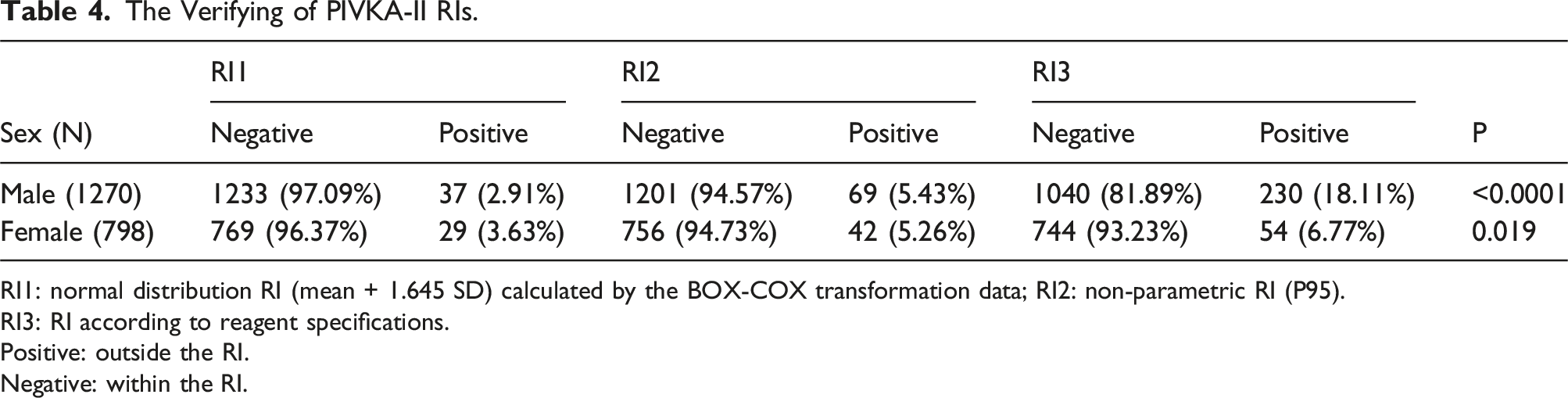
RI1: normal distribution RI (mean + 1.645 SD) calculated by the BOX-COX transformation data; RI2: non-parametric RI (P95).
RI3: RI according to reagent specifications.
Positive: outside the RI.
Negative: within the RI.
The reference values provided in the manual are derived from a cohort over 300 Japanese individuals, determined through parametric methods. Additionally, the manual suggests the establishment of laboratory-specific RIs. Comparison of our female cohort’s results with the referenced values indicates concordance, thereby indirectly validating our findings. Moreover, discrepancies observed between our findings and the reference values underscore the imperative for a tailored distinction of male group.
Discussion
Precision in RIs is critical for clinical laboratories. Solely depending on manufacturer-provided or generalized RIs might fail to capture population-specific variations, which can lead to decreased diagnostic accuracy and impaired treatment efficacy. Measuring Serum PIVKA-II levels is essential for prompt identification, treatment decision-making, and outcome assessment of HCC patients.15,16 Nevertheless, despite its importance in clinical practice, the development of RIs for PIVKA-II outside of European and Japanese groups has been restricted. 17 To address this gap, we investigated PIVKA-II RIs in the southwest region of China. By establishing gender-specific RIs for the individuals residing in this area, our results have the potential to improve the practical use of PIVKA-II among the local community.
In accordance with recommendations outlined in documents like CLSI EP28-A3C, the determination of RIs has a significant effect on the accuracy of diagnoses and effectiveness of treatments. Although the traditional approach of establishing RIs is widely regarded as the most reliable, limitations in resources can present obstacles to its application. The indirect method has become more widely accepted and proven to be effective in various studies, including our own. This approach is not only convenient and cost-effective but also utilizes existing large datasets, eliminating the need for expensive and time-consuming recruitment of healthy individuals. 10 By leveraging these datasets, researchers can expand the applicability of research findings to encompass a more diverse range of age groups, genders, and geographic locations, making the results more representative and practical. 12
We conducted an extensive analysis of a strong dataset collected from individuals undergoing routine health check-ups to determine the PIVKA-II RIs in southwest China using thorough statistical methods. In previous research, it was reported that the 95% reference interval for ARCHITECT PIVKA-II among the Han population was 40.38 mAU/mL, 17 showing slightly higher values compared to our study outcomes. Conversely, a different study indicated that the 95% reference interval for LUMIPULSE PIVKE-II within the Chinese Han population was 28 mAU/mL, 18 aligning closely with our results. These variations in reference intervals underscore the influence of the testing platforms/ assays and the characteristics of the subjects.19,20 Qin et al. gathered a total of 855 individuals who were in good health from five typical regions in China to establish the reference interval of PIVKA-II and recognized variations between regions. 18 Through the use of a standardized testing platform, we found that the reference intervals of PIVKA-II for healthy adults in the southwest region of China were slightly higher compared to those identified by Qin et al. The increased levels of PIVKA-II detected in the southwest Chinese population might be due to an increased risk of exposure to aflatoxin resulting from mycotoxin-contaminated chili peppers,21,22 along with a higher incidence of chronic kidney diseases leading to inadequate levels of vitamin K. 23 At the same time, it was found that the levels of PIVKA were notably elevated in males compared to females, potentially due to variations in sex hormones. Various epidemiological investigations have demonstrated that women after menopause have a higher risk of developing liver conditions such as hepatic steatosis, steatohepatitis, and hepatocellular carcinoma. 24 This suggests that oestrogen could impact the metabolic functions of liver cells, including the processing of fats, sugars, and proteins. As a result, oestrogen might have an effect on the creation and breakdown of specific proteins in the liver, influencing the production or secretion of PIVKA.
Our study has some limitations. Challenges such as the lack of standardized guidelines and potential influence of diseased subpopulations highlight areas for further development and standardizations in the use of indirect method for establishing RIs. 25 The indirect method used for RI establishment may inadvertently include non-healthy individuals, necessitating careful interpretation of the results. Additionally, the cross-sectional nature of our analysis precludes assessment of temporal changes in PIVKA-II levels in healthy subjects, highlighting the need for longitudinal studies to elucidate any such dynamics.
In conclusion, specific RIs for PIVKA-II were effectively determined in southwest China using an indirect approach, filling a significant knowledge gap regarding normal RIs for this biomarker in the area. Through the analysis of a comprehensive dataset and meticulous statistical methods, gender-specific RIs were defined, with established ranges of 0–35 mAU/mL for males and 0–29 mAU/mL for females using the normal distribution method, while 0–32 mAU/mL for males and 0–28 mAU/mL for female using the non-parametric method. These RIs offer essential insights for the precise evaluation of PIVKA-II concentrations within the local population.
By setting up these RIs, our research makes a substantial contribution to improving clinical practice in southwest China, especially in the area of diagnosing and treating HCC. Having RIs that are specific to the region guarantees that medical professionals can utilize precise and dependable reference ranges, ultimately leading to better accuracy in diagnosis and effectiveness in treating patients with HCC in this locale.
Supplemental Material
Supplemental Material - Establishment of sex-specific reference intervals for PIVKA-II in Southwest China: A real-world data analysis
Supplemental Material for Establishment of sex-specific reference intervals for PIVKA-II in Southwest China: A real-world data analysis by Bin Wei, Yalin Zheng, Lixin Li, Limei Luo and Ying Guo in Annals of Clinical Biochemistry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study protocol was approved by the Ethics Committee of West China Hospital of Sichuan University (No. 20241706), and was performed in accordance with the Declaration of Helsinki.
Guarantor
Bin Wei.
Contributorship
Bin Wei performed the data analysis and wrote the manuscript. Yanlin Zheng, Lixin Li and Limei Luo helped perform the analysis with constructive discussions. Ying Guo contributed to the conception of the study and revised the manuscript. All authors read and approved the final manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.