
Abstract
Introduction
In the United Kingdom (UK), over one million patients present to the emergency department (ED) annually with head injury, often with features of traumatic brain injury (TBI). 1 TBI is defined as a disturbance in brain function and classified using the Glasgow Coma Score (GCS) into severe (3-8), moderate (9-12) and mild (13-15). The vast majority of cases are of mild TBI (mTBI) 2 but often meet national criteria for computed tomography (CT) head imaging 1 with under one in 10 patients demonstrating abnormalities. 3
In a large observational study from the United States (US), patients with mTBI underwent tandem brain biomarker measurement of ubiquitin C-terminal hydrolase-L1 (UCH-L1) and glial fibrillary acidic protein (GFAP) within 12 hours of injury, concluding that it may safely decrease CT imaging by a third. 4
We aimed to evaluate performance of the UCH-L1/GFAP tandem test in the prediction of CT evident brain injury in patients with mTBI in a UK population, and potential impact on ED patient flow.
Methods
A prospective cohort service evaluation was performed in the ED and clinical biochemistry laboratory of a tertiary referral trauma centre in Scotland. This study was reviewed by the institutional research governance team and deemed a service evaluation (Organisational ID 5725), and Caldicott approval (CG/2023/167) was obtained.
Adult patients (≥18 years) presenting within 12 hours of head injury with GCS 13-15 for whom a CT head scan was requested, were eligible for inclusion. Exclusions included: penetrating head injury; poly-trauma; blood sampling >12 hours from injury; insufficient sample volume, and lack of test calibration materials. Samples were transferred to the biochemistry laboratory for preparation of serum or plasma aliquots that were refrigerated (2°C) or frozen (−20°C) for subsequent batch analysis of UCH-L1 and GFAP on the Alinity platform (Abbott Laboratories, IL). Care proceeded normally and UCH-L1/GFAP results were not available to clinical staff. A biomarker result of both UCH-L1 and GFAP beneath manufacturer recommended cut-points (400 pg/mL and 35 pg/mL, respectively) was reported as TBI absent.
Non-contrast CT head scans were performed on a GE Optima CT660 scanner and radiology reports made available to clinicians as per normal practice. These scans were subsequently reported independently by a second radiologist blinded to the first report and to UCH-L1/GFAP results. Reports were compared for the determination of CT-evident TBI, defined as: any traumatic intra- or extra-axial haemorrhage or shear-type injury or traumatic brain oedema +/− associated herniation or ventriculomegaly. Any discordance was resolved by a consultant neuroradiologist.
Using the electronic patient record, patient demographics, mechanism of injury, indication for CT imaging were extracted. Time from CT request to CT result availability was recorded and compared with time from venepuncture to biomarker result availability. Evaluation constraints meant biomarker samples were analysed in batches so ‘time to result’ was estimated as time from venepuncture to sample reception in the biochemistry laboratory plus 60 min (the time taken for sample preparation, testing and issuing of result).
Patients were followed up for any re-attendance, repeat neuroimaging, interventions for brain injury or death, within 30-days. Deaths were adjudicated separately by two physicians as TBI related or not, with discrepancies resolved by a third physician.
Data were expressed as frequencies and percentages, or as mean and standard deviation (SD) or median and interquartile range (IQR), depending on normality of distribution. For CT-evident TBI we calculated the sensitivity and negative predictive value (NPV) for the UCH-L1/GFAP test with 95% confidence intervals (CI), using Wilson’s method.
Results
Of 133 patients who had blood samples taken, 89 (67%) met the inclusion criteria (mean age 63 [SD 22] years, 57% men) (Figure S1). Most patients (53, 60%) were aged ≥65 years, 30 (34%) were intoxicated and 33 (37%) were anticoagulated at time of injury. The commonest mechanism of injury was a fall from standing (68, 76%) and 59 patients (66%) had a GCS of 15 on ED arrival (Table S1).
The Diagnostic Performance of the UCH-L1-GFAP Tandem Test in the Prediction of CT Evident TBI (n = 89).
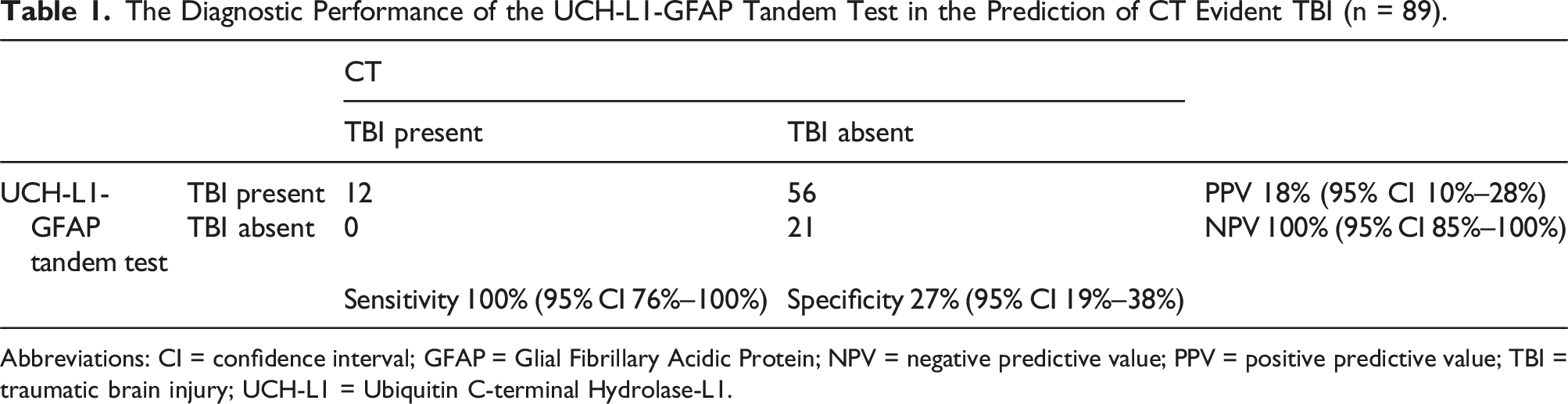
Abbreviations: CI = confidence interval; GFAP = Glial Fibrillary Acidic Protein; NPV = negative predictive value; PPV = positive predictive value; TBI = traumatic brain injury; UCH-L1 = Ubiquitin C-terminal Hydrolase-L1.
The median time from request to CT report availability was 89 (IQR 53-136) minutes and from venesection to biomarker result availability 88 (IQR 75-109) minutes.
Discussion
In our UK population evaluation, the UCH-L1/GFAP test identified one in four patients as low-risk for CT-evident TBI with excellent sensitivity and NPV, comparable with larger international cohorts. 4 Whilst there was no significant difference in time to CT or UCH-L1-GFAP result, we note that three of every four patients undergoing biomarker testing would require subsequent CT imaging, significantly prolonging ED length of stay.
Since 2021, near patient UCH-L1/GFAP testing on the Abbott i-STAT Alinity device has been available with comparable diagnostic performance to measurement on the laboratory platform 5 but, until recently, this required preparation of a plasma sample, limiting usefulness. The advent of whole blood UCH-L1/GFAP testing on a point-of-care device, with results available in 15 minutes, 6 may be a game-changer. If easily adopted into clinical pathways, one in four patients with mTBI may be suitable for early discharge without the need for previously indicated CT imaging; decongesting EDs, reducing pressure on Radiology services and improving patient flow.
We acknowledge that small sample size, single centre design, and the surrogate time to biomarker result as limitations, necessitating caution in interpretation of results. A number of patients were excluded because blood was taken >12 hours after injury, perhaps reflecting difficulty in discerning accurate event timings, or ability to draw blood at time of CT request. Evaluation of test performance in real time, and beyond 12 hours, would be helpful.
Rule-out performance of the UCH-L1/GFAP test in our evaluation in a UK population was excellent. However, for clinicians to change practice evidence from large prospective randomized studies is needed, as well as real-life evaluation of incorporation into pathways that are clinically safe, acceptable to patients, and demonstrate time and cost benefits.
Supplemental Material
Supplemental Material - Ubiquitin C-terminal hydrolase-L1 and glial fibrillary acidic protein tandem brain biomarker test in the prediction of CT evident brain injury: A prospective evaluation in the emergency department
Supplemental Material for Ubiquitin C-terminal hydrolase-L1 and glial fibrillary acidic protein tandem brain biomarker test in the prediction of CT evident brain injury: A prospective evaluation in the emergency department by Jemima M Curran, Katherine Onions, Jessica Watts, Arnab Rana, Emma Hughes, James Allison and Jamie G Cooper in Annals of Clinical Biochemistry
Supplemental Material
Supplemental Material - Ubiquitin C-terminal hydrolase-L1 and glial fibrillary acidic protein tandem brain biomarker test in the prediction of CT evident brain injury: A prospective evaluation in the emergency department
Supplemental Material for Ubiquitin C-terminal hydrolase-L1 and glial fibrillary acidic protein tandem brain biomarker test in the prediction of CT evident brain injury: A prospective evaluation in the emergency department by Jemima M Curran, Katherine Onions, Jessica Watts, Arnab Rana, Emma Hughes, James Allison and Jamie G Cooper in Annals of Clinical Biochemistry
Footnotes
Acknowledgements
We are grateful to the staff in the Emergency Department and the Department of Clinical Biochemistry in Aberdeen Royal Infirmary for facilitating the conduct of this service evaluation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Abbott provided the UCH-L1 and GFAP controls, reagents and calibrators but had no input into the design or administration of the evaluation. JMC received support from the NHS Grampian Endowment Fund and JGC is supported by NHS Research Scotland.
Ethical approval
The need for ethical approval for this project was sought from NHS Grampian’s Research Governance department who suggested this project could be undertaken as a registered service evaluation, institutional ID 5725. Caldicott approval (CG/2023/167) was also obtained.
Guarantor
Jamie G. Cooper.
Contributorship
JMC, KO, JW, AR, EH, JA and JGC conceived the study and its design. JMC, KO, JW, AR, EH and JGC acquired the data, JMC, KO and JGC performed the analysis and, JMC, KO, JW, AR and JGC interpreted the data. JMC and JGC drafted the manuscript and all authors reviewed the manuscript critically for intellectually important content and provided their final approval of the version to be submitted. All authors are accountable for the work.
Presentation
The results from this service evaluation were presented at the Royal College of Emergency Medicine Scottish EM Clinical Conference, 10th May 2023, Glasgow, UK and the UKMedLab23 National Meeting, 11th-14th June 2023, Leeds, UK.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.