
Abstract
Venepuncture is traditionally regarded as the gold standard for collecting blood samples. However, self-collected capillary blood sampling has emerged as a practical alternative in various settings, fostering a more patient-centred, personalised, and cost-effective healthcare model. The NHS UK strategic plans published in 2023–2025 emphasise a shift in care from hospitals to community settings and from treating illness to preventing it. Self-collected capillary sampling with back-to-laboratory analysis is a strong option to support the shift of healthcare provision into the community while maintaining high-quality results and direct delivery to the electronic patient record.
Routine clinical laboratories, particularly those within the NHS, should consider this potential delivery model. However, most assay manufacturers do not currently include capillary blood in their instructions for use. Consequently, UK Accreditation Service-accredited laboratories that wish to conduct routine tests using capillary blood must perform additional comparison studies to obtain accreditation. If this is not done, they must be able to distinguish between non-accredited (capillary blood) and accredited (venous blood) tests.
This document has been created to guide clinical laboratorians through the rapidly evolving field of patient-centric sampling and how to enable safe working within a routine clinical laboratory.
Keywords
Introduction
Capillary Blood Testing (CBT) in this paper refers to fingerprick/transdermal liquid blood collection by the patient or caregiver, followed by back-to-laboratory analysis. This article does not address current issues with direct-to-consumer testing.1–3 CBT is increasingly being adopted for routine blood tests, fuelled by a major move towards community-based healthcare and the rollout of advanced, patient-focused transdermal collection technology.
CBT presents a promising alternative to traditional in-clinic venous collection methods. This distribution model may significantly enhance the effectiveness of diagnostic services by facilitating the transition of sample collection from clinical to community settings, ensuring the right test for the right patient at the right time and in the right place. This approach can also help bridge health inequality gaps by providing accurate blood diagnostics to those who are unable to access routine blood testing for many reasons, such as needle phobia, learning disabilities, poor venous access, geographical isolation, etc. 4
Given its patient-centric approach and cost-effectiveness, 5 CBT is particularly well-suited to support community-based testing, virtual wards, large-scale population screening programs, and preventive healthcare initiatives.6,7 This can potentially have a significant societal impact, particularly on patients requiring chronic care. 8 Patients often need to attend a phlebotomy location for regular blood tests. The time taken for this brief encounter can include travel time, parking, waiting for the phlebotomist's availability, and potentially time away from work or carer duties. 9 A more patient-centric approach would not only improve access to blood tests but also increase adherence to care plans. Long-term healthcare delivery plans across the UK share similar themes, including community-based care and placing ownership of care with the patient.
The NHS Fit for the future: 10 Year Health Plan for England (June 2025) emphasises three shifts in service delivery:
10
(1) Hospital to Community (2) Analogue to Digital (3) Sickness to Prevention
‘From hospital to community: the neighbourhood health service, designed around you’. The 10 Year Health Plan goes on to state ‘…We need to shift to provide continuous, accessible and integrated care’.
The devolved nations have healthcare delivery plans that address similar themes. The Health and Social Care Service Renewal Framework for Scotland (June 2025) sets out areas for change, which include the following:
11
(1) Delivering health and social care that is people-led and ‘Value Based’ (2) Improving access to services and treatments in the community (3) Redesigning our hospitals as we deliver more care within communities
The Health and Social Care Northern Ireland – Three Year Plan (December 2024) discusses the need to ‘bring care as close as possible and as early as possible to those who need it’, mirroring the three radical shifts in the NHS England plan. 12
The Diagnostics recovery and transformation strategy for Wales 2023 to 2025 (April 2023) has nine themes, one of which focuses on service transformation and ‘pushing less complex diagnostics closer to primary and community care’. 13
All identify areas where CBT with back-to-laboratory analysis can make a difference by providing equitable access to diagnostic blood tests wherever and whenever the patient requires them. This enables a more preventive approach as CBT diagnostics become more accessible to underserved populations and address patients' drive for better access to blood testing. 14
Traditional challenges, such as ease of use and painless collection, have been addressed through advances in the development of transdermal CBT devices.15–18 These devices streamline logistical processes by consolidating all consumables into a single package, thereby facilitating sample collection. Furthermore, they produce samples of sufficient quality and volume to support numerous assays, which can be performed within routine clinical laboratories. 16
The recent introduction of CBT devices has improved the accessibility and usability of CBT, making the integration of self-sampling CBT into routine laboratory practice inevitable. However, it is important to note that there is limited laboratory automation capable of efficiently processing paediatric tubes. 19 Consequently, a substantial increase in this sample type may necessitate certain operational adjustments. Furthermore, very few manufacturers include capillary blood as an approved matrix in their Instructions For Use (IFU). Similarly, there is limited data on the stability of whole blood samples available for those returned to the laboratory by post.
This paper is intended to support routine clinical laboratories in navigating the laboratory process and requirements for producing an accredited, high-quality liquid capillary sampling service that meets the needs of both the clinician and the patient. This document does not cover other capillary blood sample types, such as dried blood spots.
Sample matrix & regulatory awareness
During the COVID-19 pandemic, the Medicines and Healthcare products Regulatory Agency (MHRA) issued Medical Device Alert [MDA/2020/015 2020] concerning laboratories providing COVID-19 testing services in which the sample type has not been validated or verified by the assay manufacturer. 20 The MHRA’s position was that unless the manufacturer had explicitly listed the sample type, the assay was being used off-label and therefore not covered by the CE mark.
The alert addressed tests involving the collection of a capillary blood sample, which was subsequently forwarded to a laboratory for analysis. Although the IFUs indicated that the assays were CE-marked for use with serum/plasma, it should be noted that, unless explicitly specified, laboratory tests are CE-marked and deemed safe solely for use with venous samples. The test manufacturers had not initially validated their assays for use with capillary blood. Once manufacturers began including capillary blood in their IFUs, a change that occurred during the pandemic, laboratories holding ISO 15189:2022 accreditation for serum were required to verify capillary blood and to have this additional matrix incorporated into their UKAS schedule if they wished to claim accreditation for these tests. Prior to including capillary blood in the IFU, the laboratory would have been required to validate capillary blood as an off-label matrix.
Accreditation is, of course, not legislation, and this MDA does not stop accredited or non-accredited laboratories from offering off-label tests. However, if a laboratory or service provider wishes to use tests off-label, they must inform the patient/user, and accredited laboratories must have a process to indicate which tests are and are not ISO accredited. 20
It has been noted that questions have been raised about the accuracy of results from CBT tests due to the lack of rigorous validation. 21 Although CBT methods are still in their infancy, issues with accuracy related to serum separator collection tubes used in CBT have already been published, 22 and it is likely that, as the technology develops, further issues will be found; therefore, each laboratory must undertake its own comparison work to ensure that capillary blood shows equivalence to venous blood.
Capillary blood is a mixture of blood from arterioles, capillaries, and venules, along with interstitial and intracellular fluid. Due to this mix, the concentration of some analytes may differ from that in venous blood. Matrix effects can affect assay performance; therefore, the laboratory must first identify potential sources of these differences, for example, higher protein content in capillary blood due to interstitial fluid, skin contaminants, etc., 23 and if present, are these differences such that they alter the clinical utility of the assay?
CLSI EP35 provides a detailed flowchart to help establish specimen equivalence; we direct readers to this document.
24
However, EP35 is not specifically focused on capillary and venous comparability; therefore, PaCTS have provided a summary (Figure 1). Summary of the variables to be considered when implementing CBT into a clinical laboratory. 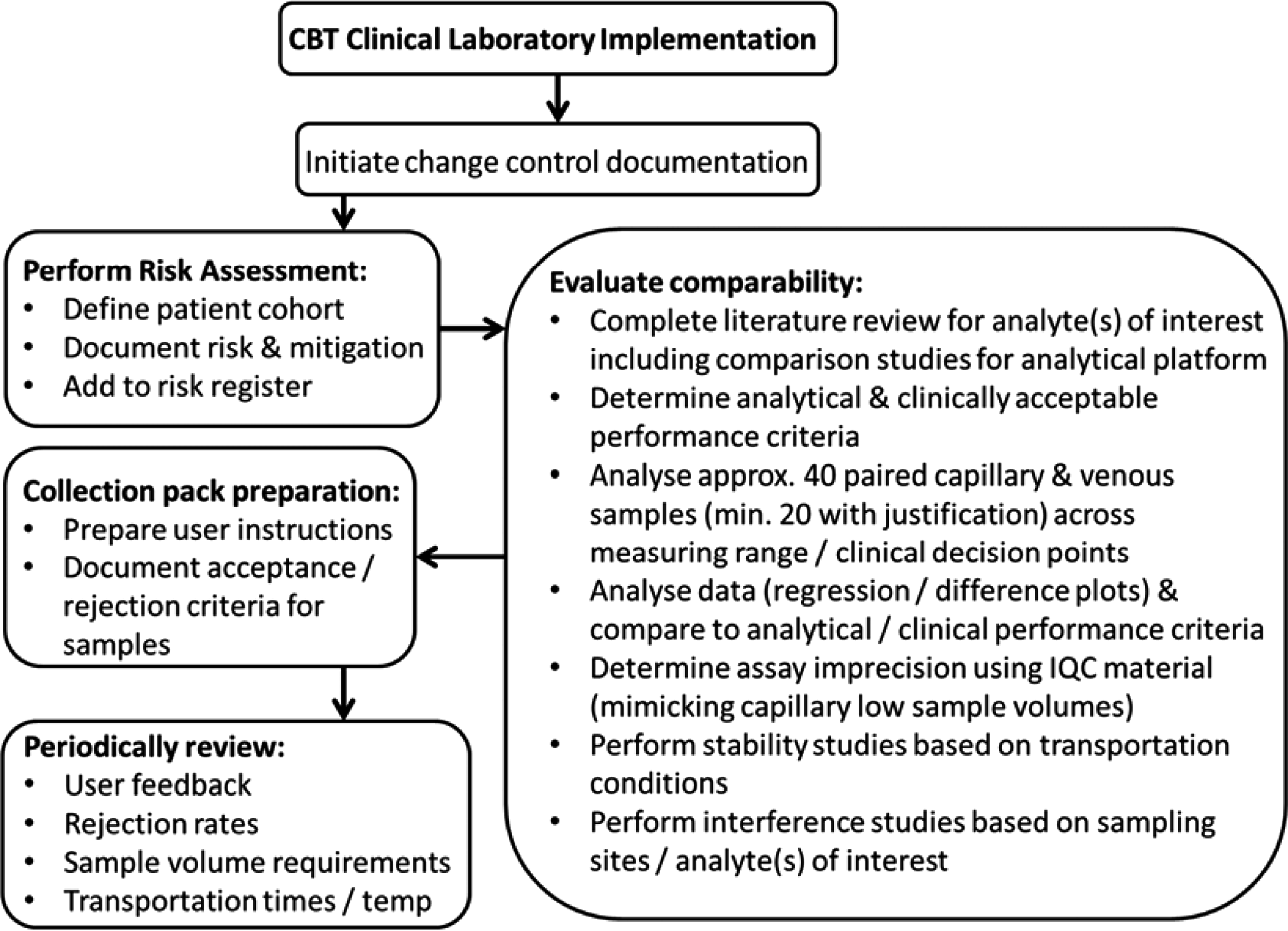
Validation
Validation must be undertaken in the form of comparability studies between serum/plasma from venous collection and serum/plasma from capillary collection, since most IFUs are not CE or UK Conformity Assessed (UKCA)-marked for this purpose. This is fundamental to ensuring that additional sample types (i.e. capillary blood) meet the required performance for valid results used in clinical decision-making. At present, there are no specific validation pathways for the accreditation of serum/plasma from capillary blood; however, CLSI EP35: Assessment of Equivalence or Suitability of Specimen Types for Medical Laboratory Measurement Procedures does provide recommendations for clinically equivalent performance for similar matrix specimen types, and as such, it is recommended as the overarching reference document. 24
An off-label specimen type change may alter assay performance, thereby affecting its clinical utility. Therefore, it is essential to document that the performance characteristics of the new sample type are clinically acceptable and ideally comparable to those of the listed sample type. EP35 states that, for similar specimen types, equivalence can be assessed by comparing observed performance with established performance claims. It is noted that due to the limited sample volume obtained in CBT, singlicate analysis may be adequate for validation studies. 25
As with any validation process in a clinical laboratory, analytical imprecision should be assessed, and the assay’s performance should be considered when presented with small sample volumes. For instance, does the assay or analytical platform yield results comparable to those from venous sample tubes when presented with low-volume capillary samples, possibly in microtainer cups? This can be achieved using Internal Quality Control (IQC) material, applied in the same low-volume process as a capillary blood sample.
Assessing concordance between capillary and venous collections blood should use contemporary collections, and any pre-analytical conditions (such as transport to the lab or time to separation) should be kept the same for both sample types when appropriate. However, experimental design may also need to account for sample stability; for instance, a three-day postal capillary blood sample may need to be compared with a same-day venous sample, if the service being envisaged includes sample postage.
The number of paired capillary and venous samples required depends on practicalities as well as the need for statistical relevance. It is recommended that 40 paired samples be used; a minimum of 20 is acceptable with suitable justification. These samples should cover the analytical range and any clinical decision thresholds, as with any routine validation project.
There is a growing list of published data on comparability between capillary and venous blood, often including sample stability data beyond the IFUs, which will give further help in designing comparability studies. 26 If concordance between venous blood is demonstrated, then reference intervals are interchangeable. However, if a significant bias is observed, further investigation into the cause of the bias and the development of a capillary-specific reference interval may be required.4,23,27,28
Statistical methods and acceptance criteria
There will always be discussion about which statistical methodology is appropriate for ascertaining relationships between two sample types, and there is published guidance recommending the log transformation of data. 29 However, we recommend that the laboratory adopt, as a minimum, two statistical methodologies: Passing-Bablok or Deming regression analysis, and Bland-Altman difference analysis, with systematic differences compared against defined criteria for acceptable bias. This might be the minimum, desirable, or optimal bias, or the reference change value (RCV), based on biological variation data from the EFLM Biological Variation Database, 30 depending on the analyte of interest and the laboratory’s preference for determining clinical acceptance.
While sample comparability studies are being designed, other important variables may need to be considered; these should be included in the change control and risk assessment documentation for the validation project. Other critical areas to consider include sample collection, waste disposal and sample return. Although these may not be issues during the validation phase, they will be critical for service delivery.
Risk assessment
The potential risks to the patient from self-collection must be determined and recorded in a risk assessment. Data from the validation project will provide some indication of potential issues, but it is recommended that the target patient cohort be involved in the patient-facing aspects of the project. Likewise, any shortfalls in the validation should be highlighted, and the risk assessment should be reviewed periodically to ensure it remains valid. We refer the reader to both ISO 15189 and ISO 22367 (Application of risk management to medical laboratories).
Sample collection
The laboratory must provide patients with information and materials for collecting and handling samples. 28 This should include instructions for recording the identity of the person collecting the samples and the date and time of collection. The specimen volume requires careful consideration to ensure an appropriate amount of blood is obtained. It is important to consider the required sample volume and the acceptable failure rate from insufficient samples. When a very limited number of assays are required, failure rates from insufficient sample volume will be low; larger panels may cause downstream patient pathway issues. Therefore, the validation project needs to assess the amount of sample required against what is being obtained. Rejection rates due to insufficient sample volume and haemolysis should be audited as part of the periodic review of the CBT work stream. 4
Waste disposal
It is important to dispose of used blood-collection equipment correctly to prevent injury. However, as many items are CE-marked for self-collection they include robust outer cases and self-retracting safety lancets, which may in some cases be safely disposed of in household waste. Some local councils provide a sharps disposal service by supplying individuals with sharps bins and collecting them when they are full. The validation study should consider which disposal services are applicable for the devices used and review manufacturers’ IFUs for guidance.
Many NHS organisations have sharps policies that set out their requirements for providing sharps disposal services to patients at home. For example, for patients who are carriers of infectious diseases, recommendations usually suggest that suitable arrangements be made to dispose of used articles as contaminated waste.
Sample return
Although capillary blood is ideal for self-collection, and kits are designed to be returned by post to the laboratory, this is not always necessary. Delivery in person to a designated drop-off point, such as a GP surgery, will ensure samples are collected alongside those taken in the clinical setting, making transportation and routine laboratory workflow easier, as samples will be processed within current stability timeframes. For samples posted to the laboratory, understanding the stability of whole blood analytes across different temperature ranges and time scales is essential.
Some analytes are highly robust, whereas others can be affected by even low levels of degradation. Given this, it is recommended that the laboratory conduct sample stability experiments as part of the validation process using whole blood stored at the expected temperatures over the expected transport period. 4 Additionally, it is recommended that these variables, if not measured in real-time for each sample, be monitored and periodically reviewed, taking into account the laboratory’s stability studies.
The acceptable specimen storage period and analyte stability are likely to differ for capillary blood samples due to the small sample volume; therefore, add-on requests are not recommended. This should be evaluated during validation studies.
Reporting results
The report must specify the type of primary sample, i.e. capillary blood. This will be particularly important when investigating spurious results caused by potential sample contamination. Differentiating serum/plasma from venous collection and capillary collection is critical and may depend on laboratory information management system (LIMS) functionality. Possible routes include linking results to the sample type or using capillary-specific test codes. This may also help prevent inappropriate testing of capillary samples and make trending and service management information easier to access.
Conclusions
CBT respects patient privacy and prioritises the patient’s comfort and needs. 28 This enables the right sample to be collected from the right patient at the right time in the right environment.
The recommendations below are a first step toward consensus for the laboratory validation of self-collected capillary samples, enabling this critical patient-centric sample to be included in routine clinical laboratories. By standardising validation processes, this approach aims to promote more effective benchmarking in line with ISO 15189:2022.
Recommendations
Recommendation 1
Comparability studies between venous and capillary blood should be performed or sourced from the literature for the analyte(s) being determined.
Recommendation 2
Comparability studies should use 40 paired venous and capillary samples (minimum 20 paired samples with justification) across the measuring range and clinical decision points.
Recommendation 3
Regression analysis (Deming or Passing-Bablok) and difference plots (Bland-Altman) should be used to assess differences in results obtained from venous and CBT samples.
Recommendation 4
Analytical imprecision from using small sample volumes should be considered. This can be done using capillary samples or IQC material mimicking the low-volume samples expected from CBT sampling.
Recommendation 5
Statistical analysis should be used to determine whether CBT for an analyte is viable and whether different reference intervals may be needed for CBT samples.
Recommendation 6
Capillary (whole blood) stability studies should be conducted at the expected temperatures and for the required time periods for transportation.
Recommendation 7
The target patient cohort(s) should be considered, including potential interference from medications during sample collection, such as topical creams. Review literature or perform interference studies where required. Consider adding advice in the instructions for use for the patient.
Recommendation 8
The laboratory should complete a risk assessment for the use of CBT, which must consider potential risks to the patient from self-collection of samples.
Recommendation 9
The laboratory should prepare concise, unambiguous instructions for use for specimen collection by a patient or caregiver.
Recommendation 10
The laboratory should document acceptance and rejection criteria for CBT samples, with rejection rates periodically reviewed to determine whether changes to procedure or sample collection instructions are required.
Recommendation 11
The laboratory should periodically review the sample volume requirements to ensure that neither too little nor too much blood is collected.
Recommendation 12
A review of sample stability should be performed whenever a new analyte or transport condition is introduced.
Recommendation 13
Where it is not possible to obtain capillary samples with analyte results covering the clinical range of interest, the laboratory should periodically review patient results and assess the risk. Consider additional comparability samples where appropriate.
Recommendation 14
User feedback from the patient population should be periodically reviewed for suggestions and complaints about the sampling process.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
TW.
Contributorship
TW prepared the first draft of the manuscript. TW, SH, and KP compiled the recommendations, figure and second draft. All authors reviewed, edited and approved the final version.