
Abstract

Introduction
Many depressed patients fail to respond to what seem to be perfectly adequate therapeutic interventions. Indeed, non-response or at least partial-response is arguably the norm, with more than two-thirds (67.1%) of patients in real-world settings not responding to their first antidepressant (John Rush et al., 2006). But defining a ‘condition’ by its failure to respond to treatment is problematic, as non-response may simply be a consequence of the underlying condition being different to the suspected diagnosis. That is to say, the illness is not depression and that misdiagnosis is the main reason as to why the condition is not responding to antidepressant therapy. In practice, our reliance on non-response to define treatment-resistant depression (TRD) has meant that the phenomenon has insidiously been reified as a diagnosis in itself – even though its true nature remains a mystery.
Defining TRD
Both clinically and for the purposes of research, discussion regarding the definition of treatment-resistant depression usually centres on pharmacotherapy. But in practice, the treatment of depression also involves psychological therapies such as cognitive-behavioural therapy (CBT), and physical interventions such as electroconvulsive therapy (ECT). However, treatment non-response is rarely framed in either psychological or physical treatment terms. Instead the most widely accepted definition of TRD is based predominantly on pharmacotherapy a and is defined as non-response to two courses of adequate antidepressant therapy (Thase and Rush, 1997). The problem with this definition, and many other similar descriptions of TRD, is that it lacks specificity. Alternatives such as refractory depression are equally non-specific and in addition seem to suggest that ‘resistance to treatment’ is an intrinsic property of the depressive illness itself that confers refractoriness. In other words, there is something about the very nature of the depressive illness that makes it less responsive to treatment. However, in most cases of depression, the explanation for an inadequate clinical response is relatively straightforward, and treatment failure usually arises because of reasons other than lack of antidepressant efficacy (see Table 1) (Malhi et al., 2019). Thus, establishing a meaningful definition of TRD on the basis of treatment alone seems elusive.
Potential Sources of ‘treatment-resistant depression’
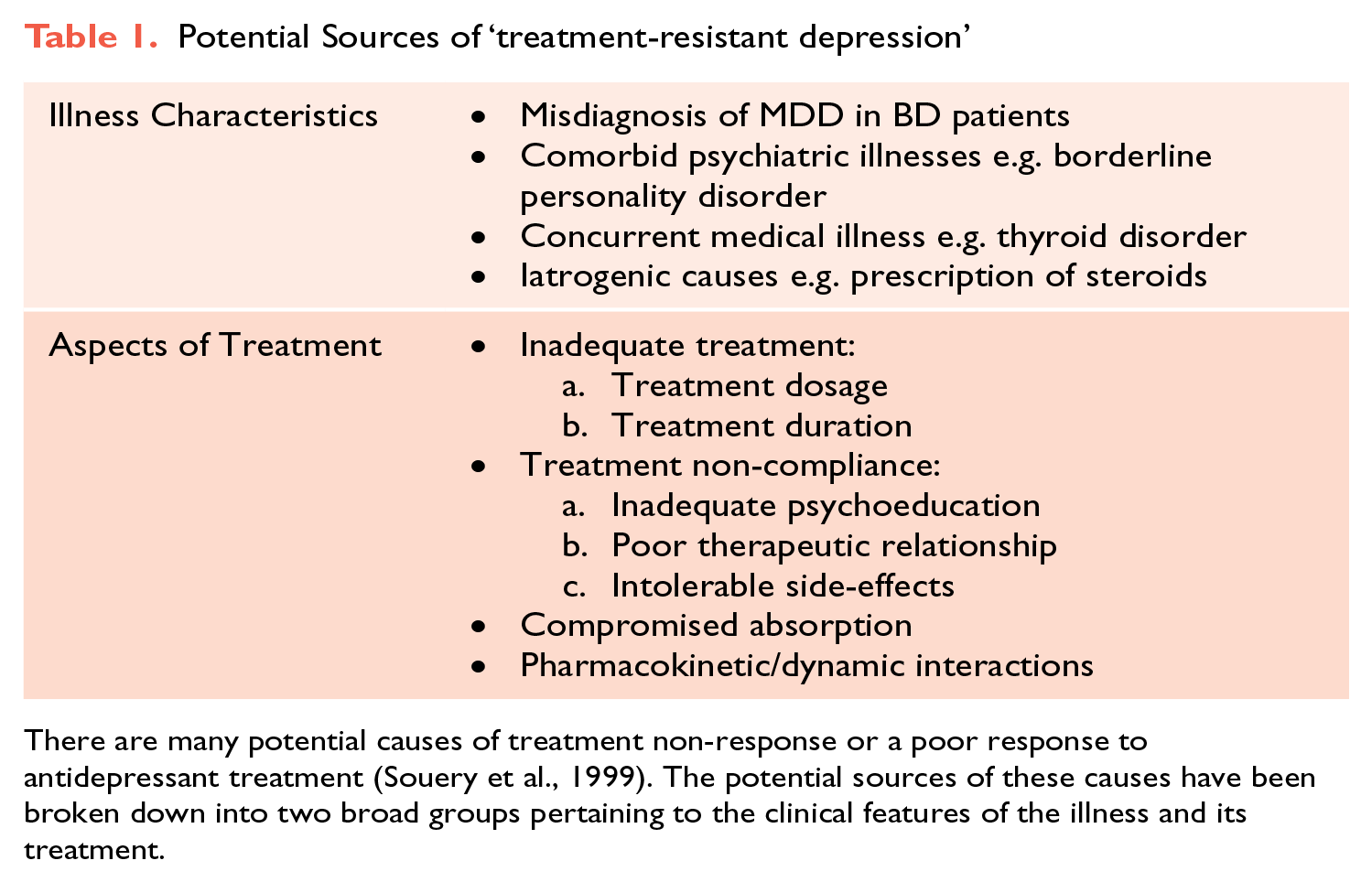
There are many potential causes of treatment non-response or a poor response to antidepressant treatment (Souery et al., 1999). The potential sources of these causes have been broken down into two broad groups pertaining to the clinical features of the illness and its treatment.
Therefore, in this Make News article we have decided not to dwell on critiquing the various descriptions of TRD, but instead devote our time to discussing how to develop a more meaningful definition that may cut through the heterogeneity of this construct and provide a deeper understanding of non-response by revealing new insights into its pathophysiology.
Depression
Clinical Specificity
When considering treatment response in relation to defining TRD it is useful to specify what is meant by the term depression. In practice, depression is defined on the basis of phenomenology i.e. clinical symptoms. But because there are no symptoms that are pathognomonic of depression and most are just features, the clinical syndrome can be defined in many different ways. For instance, some clinicians favouring subtypes of depression, such as melancholia and psychotic depression, and others, degrees of severity e.g. mild, moderate and severe (Malhi and Mann, 2018). Furthermore, the severity of the depressive symptoms that are present can also vary enormously, and this produces myriad symptom patterns – that have been grouped together phenomenologically but may in fact be clinical expressions of different underlying ‘illnesses’. Hence the clinical picture of depression can be easily confused with depressive syndromes caused by other psychiatric disorders and medical illnesses (see Table 1). These ‘phenocopies’ of depression have the appearance of depressive disorders by virtue of expressing a similar symptom profile, even though their aetiology and pathogenesis is very different.
Reversibility
The other key consideration of a depressive syndrome is its reversibility, in particular the extent to which its underlying pathology can be reverted. Empirically, it would appear that in most cases the underlying problem that causes an acute episode of depression can be rectified and that the illness is putatively ‘reversible’, however this is not necessarily the case, and it may be the case that the underlying pathology is irreversible. In such cases the underlying pathophysiological changes are severe, and we have termed this complete irreversibility of function – a catastrophic failure (see Figure 1). However, because we do not know the pathophysiology of depression, and any pathology we have identified is yet to be closely coupled to clinical phenomenology, a depressive syndrome can be erroneously diagnosed as treatment-resistant simply because it appears to be irreversible.
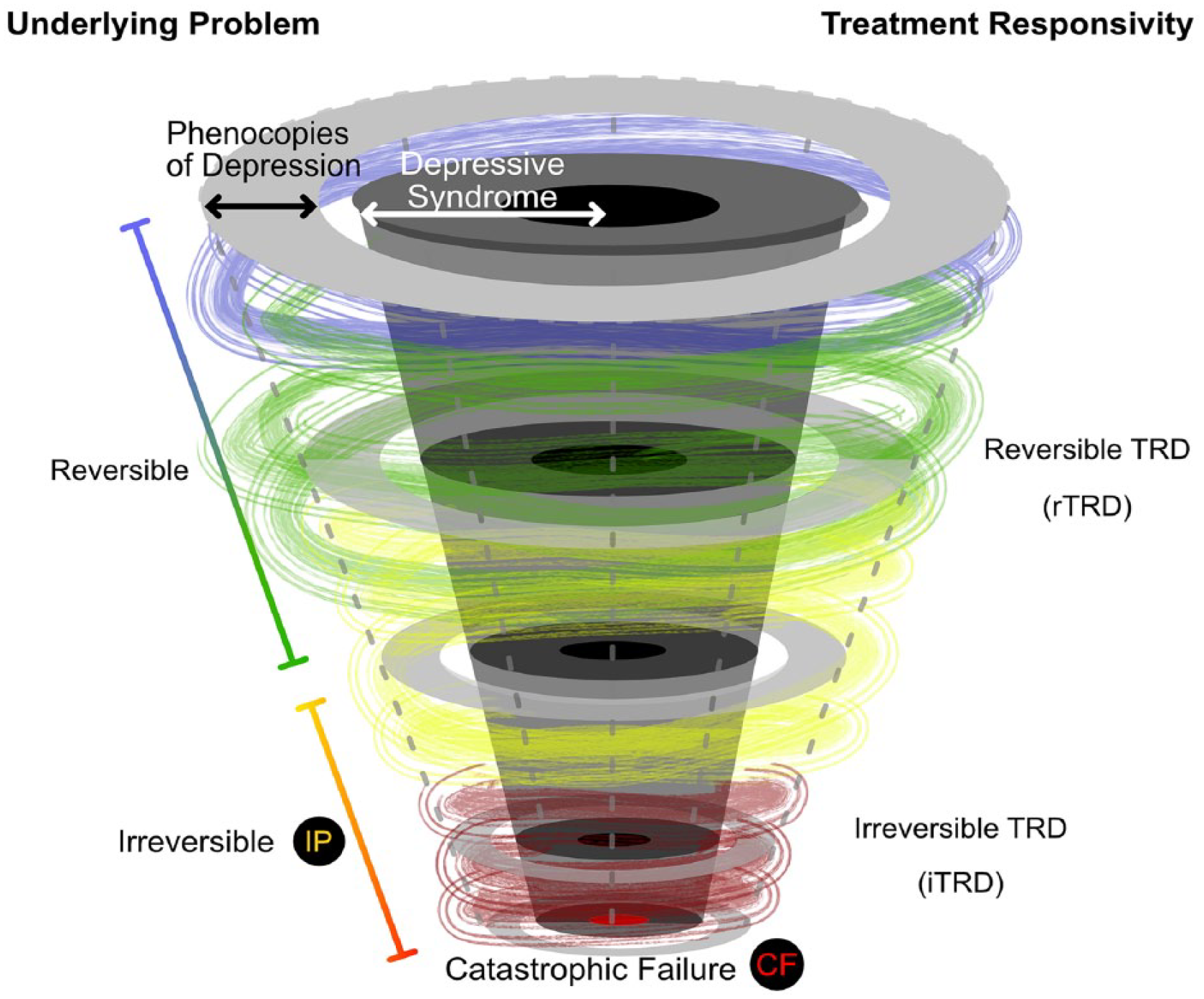
Conceptualizing Treatment Resistant Depression (TRD). Most definitions of TRD are based on non-response, and the number, and kinds, of treatments prescribed. This approach fails to acknowledge that depression is a heterogeneous condition that has many causes, and that some of its manifestations are phenocopies. These definitions of TRD also ignore the possibility that there is a truly non-responsive component of TRD that is underpinned by an irreversible underlying problem (IP). Irreversible TRD (iTRD) is the consequence of a catastrophic failure (CF) and it is this component of TRD that is truly treatment resistant.
Where the clinical syndrome is unequivocally that of depression and the underlying problem is irreversible – this constitutes true treatment-resistant depression. In TRD defined as such there is little or no prospect of future response because of a catastrophic failure within the mechanisms of brain function, be they biological, functional or mental b . The identification of this irreversible subgroup that constitutes a core treatment-resistant depression (irreversible treatment-resistant depression – denoted as iTRD) is essential because it is a significant confound in the treatment of depressive disorders that limits our ability to examine reversible TRD. By characterising and better defining the essence of TRD, the heterogeneity of the treatment-resistant group can be reduced. To achieve this, the first step is to tightly define depression and exclude overlapping, comorbid or conflating diagnoses. The next step is to categorise the severity of the illness and its responsivity, and to determine whether any intervention produces any discernible benefit, thereby gauging the level of treatment-resistance and any potential for treatment response. The final remaining component is then iTRD, which has been caused by an underlying catastrophic failure.
iTRD
In absolute terms iTRD applies to instances in which the brain is irreversibly damaged. This ‘damage’ produces a depressive syndrome but there is little prospect of it being reversed – especially using conventional antidepressant treatments. For example, depressive syndromes in the context of a neurodegenerative process such as dementia, or a stroke may be cases of iTRD. Irreversible TRD may also include cases where the response to treatment is extraordinarily slow because it depends on compensatory and self-reparatory mechanisms. These processes may take months and years and even then, only produce a partial improvement at best. This is different to the effects of usual antidepressant therapies where interventions are able to produce a relatively prompt and discernible response in a matter of weeks and months by facilitating mechanisms that are still functioning (reversible).
Conclusion
The construct of TRD is inherently complicated because it consists of many components. Its definition based on non-response is of limited value as it provides few mechanistic insights. Therefore, defining iTRD is perhaps a more useful first step and one that may lead to a better understanding of TRD as a whole by providing a pathway for researching its reversible counterpart.
In an age where good news and good ideas are difficult to find, this series offers constructive criticism of promising concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
GSM has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. EB declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.